By jacob john Etiology of chest trauma Blunt

By jacob john

Etiology of chest trauma Blunt force trauma Ø M. V. A Ø Fall Ø Assault Penetrating injury Ø Shooting Ø Stabbing Ø Iatrogenic

Initial management

Component of chest trauma • RIB fracture • Flail chest • Pneumothorax • Haemothorax • Lung: laceration • Esophageal & Tracheobronchial • Cardiac: contusion, rupture • Aortic : rupture
![Chest wall injury [simple] • Rib fracture most • common Serious in elderly& chronic](http://slidetodoc.com/presentation_image_h/e39a011a1c30c6514eb2cc2046658773/image-6.jpg "Chest wall injury [simple] • Rib fracture most • common Serious in elderly& chronic")
Chest wall injury [simple] • Rib fracture most • common Serious in elderly& chronic lung D/S v. Management • Analgesic • Physiotherapy & early ambulation

Ist & IInd RIB FRACTURE ØSerious chest injury ØHigh energy transfer ØAssociated with major vascular , thoracic & cranial injury v. Management: • Pulmonary toilet • Surgical interference …displaced fragment.

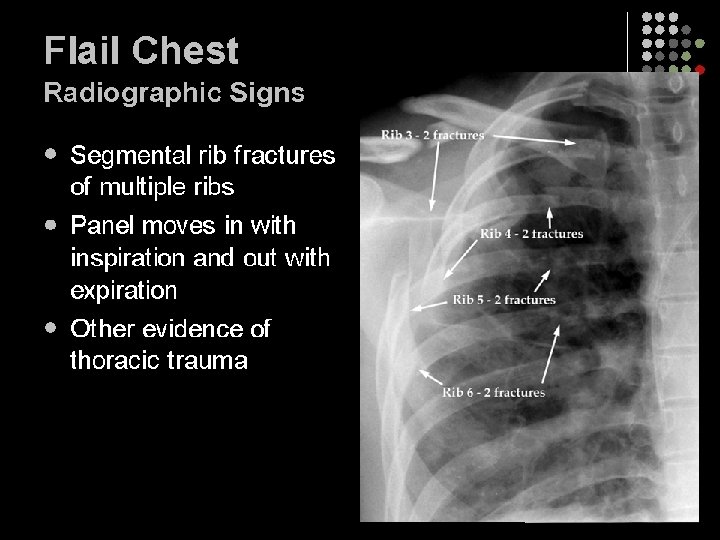
Flail chest • Definition: 3 or more consecutive rib facture in 2 or more place producing free Floating/unstable segment. • Classification: Anterior flail chest Lateral type

Management q. General: • Analgesic • Splinting • Intubation's / ventilation v. Specific: • Pericostal suturing • External/internalfixation • Thoracotomy

Complications: v 22% disability rate with 63% having long term problems v. Persistent chest wall pain v. Deformity v. Dyspnoea on exertion

Sternal fracture • M. V. A • Upper & middle 3 rd q. Clinical feature : - üLocal tenderness üEchymosis üSwelling üCrepitus

Management v. X ray & Echo v. Uncomplicated • Analgesic • Bed rest v. Complicated • Open reduction & internal fixation

Pneumothorax q. Definition: Air trapped within pleural cavity following injury to chest , lung or airway.

v. Clinical presentation ØTachyponea ØHypotension ØRespiratory distress ØBreath sound decreased

Management v. X-ray v. Tube Thoracostomy v. Chest decompression with wide bore needle inserted in llnd I. C. S.

Indications: üSpontaneous /traumatic pneumothorax üHaemothorax üRecurring pneumothorax after removal of chest tube üProphylaxis pre-operatively in flail chest

Complications: • Haemorrhage from IC vessel injury • Subcutaneous emphysema • Injury due to malpositioned tube • Local infection • Pain • Re expansion pulmonary oedema after prolonged collapse & rapid reinflation • Inadequate drainage of pleural space due to clots & plugging or kinking of the tube
![Open pneumothorax [sucking chest] ØDefect in chest wall following trauma. ØAir enter from out](http://slidetodoc.com/presentation_image_h/e39a011a1c30c6514eb2cc2046658773/image-19.jpg "Open pneumothorax [sucking chest] ØDefect in chest wall following trauma. ØAir enter from out")
Open pneumothorax [sucking chest] ØDefect in chest wall following trauma. ØAir enter from out side. ØIntrathoracic pressure raised with mediastinal shift. • Management: Chest tube with occlusive dressing

Tension pneumothorax q. Leaking of air from an underlying pulmonary parenchyma. v. Management; Needle thoracostomy[1416 guage inserted through llnd I. C. S] • Tube thoracostomy

Heamothorax ØDefinition ; collection of blood in pleural cavity. varies from minor to massive based on vessel injured. q. Management: v. Chest tube thoracostomy{>28 F}. v. Thoracotomy.

Thoracotomy q. Indications: Ø 1000 ml drained at insertion of chest drain ØBleeding>100 / 15 min Ø>200 ml/hr for 3 -4 hr ØCardiac tamponade ØMajor bronchus , oesophageal , diaphragm injury

Lung contusion ØLaceration following penetrating or blunt trauma.

Management v. Uncomplicated o Antibiotic o Lasix o Dexamethasone o Bronchodilator o Suction drainage o Physiotherapy v. Complicated o Thoracotomy o Pneumonectomy[hi gh mortality >50%]

Injury to Major Airway ØRare ØHigh mortality v. Pathophysiology: - • Direct compression of airway with closed glottis or injury producing partial or complete avulsion

Management ØAdequate air supply ØEndotracheal intubation ØTracheostomy ØBronchoscopy for definitive diagnosis q. Definitive measure ; restoration of airway with end to end anastomosis. Defect >3 cm proximal and distal mobilization required.

Diaphragmatic injury ØRare ØClinically left side commonly identified ØAutopsy & CT show equal incidence ØIncidental diagnosis v. X-ray • Diaphragmatic distruption • Ipsilateral hemidiaphragm • elevation Abdomen visceral herniation

Management ØLaparotomy : Using continuous or interrupted braided suture ØThoracotomy : Postrolateral injury

Esophageal injury ØRare ØCause: • Sudden increase in luminal pressure. q. Clinical feature: - • Chest pain • Pneumothorax • Intraabdominal free air • Systemic sepsis

Management ØFluid resuscitation ØI. V broad spectrum antibiotic Ømultiple chest tube drainage q. Surgical üWithin 24 hr debridement and primary closure üAfter 24 hr primary closure with autologus tissue transplantation. v. Poor general condition & advanced mediastinitis üEsophageal exclusion & diversion üCervical esophagotomy

Cardiac injury/ myocardial contusion Ø 15 -16%chest trauma show cardiac involvement. ØAssociated with sternal injury. v. Diagnosis • 12 lead E. C. G • Echocardiogarphy • Enzyme elevation

v. Management • Constant monitoring for 48 hr • Resuscitation • Antiarrhythmic

Cardiac rupture ØHigh mortality ØRT atrium & ventricle ØChest pain to collapse v. Sign: • Muffled heart sound • Jugular venous • distension Hypotension

Management • Cardioraphy with or without cardiopulmonary bypass. • Counter pulsation using balloon pump.

Penetrating heart injury v. Causes: • Stabbing • Shooting • Iatrogenic v. Feature: ØHypotension ØTachycardia ØHigh C. V. P ØPulsus paradoxus q. Diagnosis: o E. C. G o Echocardiography

Management • Left anterior Thoracotomy • Aspiration & repair with buttressed suture

Aortic Transection v. Mechanism: - • shearing force • Direct luminal pressure against point of traction. q. Diagnosis • X-ray : widening of • mediastinum with shadow CT


Management v. Thoracotomy: • Via left 4 th I. C. S • Direct suture with or without interposition graft.

Summary: Chest Trauma • • • Common Serious Primary goal is to provide oxygen to vital organs Remember Airway Breathing Circulation Be alert to change in clinical condition

Thank u!
- Slides: 41