By Gail Lupica Ph D RN CNE Largest

* By: Gail Lupica Ph. D, RN, CNE

*Largest internal organ in the body *Right upper quadrant in peritoneum *Performs over 400 functions *Blood supply : * 2/3 from the portal circulation (from the intestines, stomach, spleen, and esophagus) * 1/3 from the hepatic artery (which perfuses the organ itself) *

*chronic progressive disease characterized by destruction of the liver parenchymal cells. Fibrous tissue distorts the liver’s normal lobular structure, resulting in impeded vascular flow. *Fibrous/nodular tissue leads to poor cellular nutrition…scar tissue = decreased functioning of the liver. *
 *Postnecrotic cirrhosis is complication of viral,")
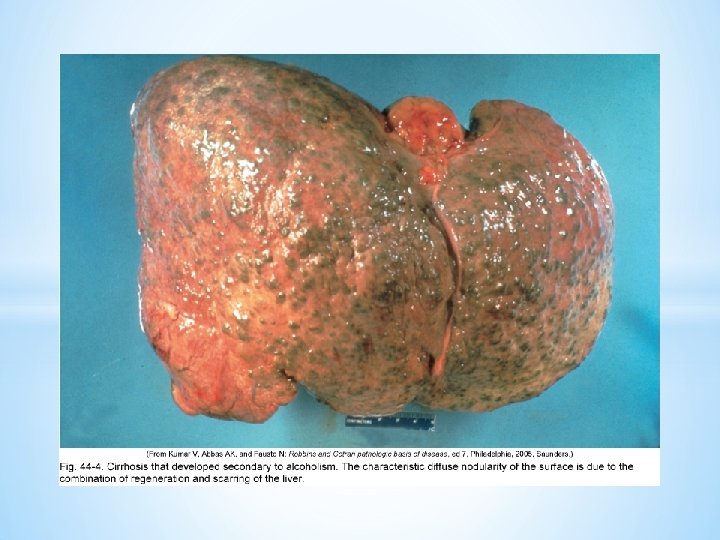
There are four types of cirrhosis *Alcoholic (laennec’s) *Postnecrotic cirrhosis is complication of viral, toxic, or idiopathic (autoimmune) hepatitis. *Biliary cirrhosis is associated with chronic biliary obstruction and infection. jaundice is the main clinical manifestation. *Cardiac cirrhosis results for long-standing, severe right sided heart failure *


*Right healthy liver *Middle fatty liver *Left liver * with cirrhosisswollen

*The portal vein carries blood to the liver. *This blood has a high concentration of toxins and bacteria from the intestines. The Kupfer cells (line the sinusoids of the liver) destroy these toxins and prevent the spread to the systemic circulation. *
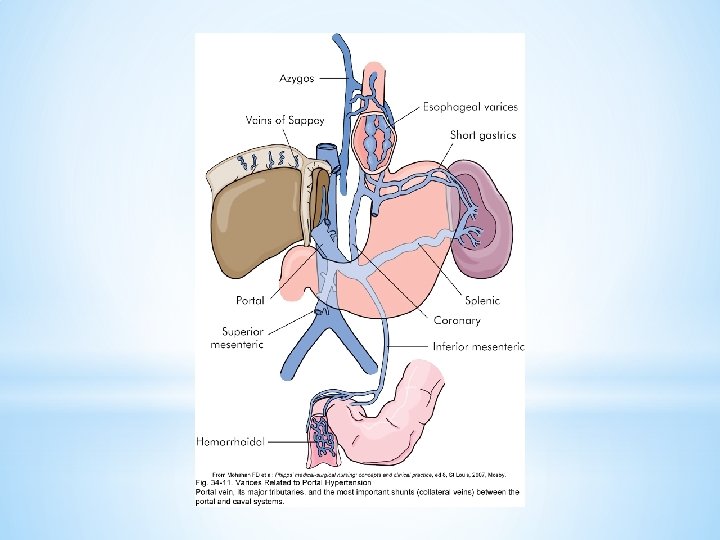

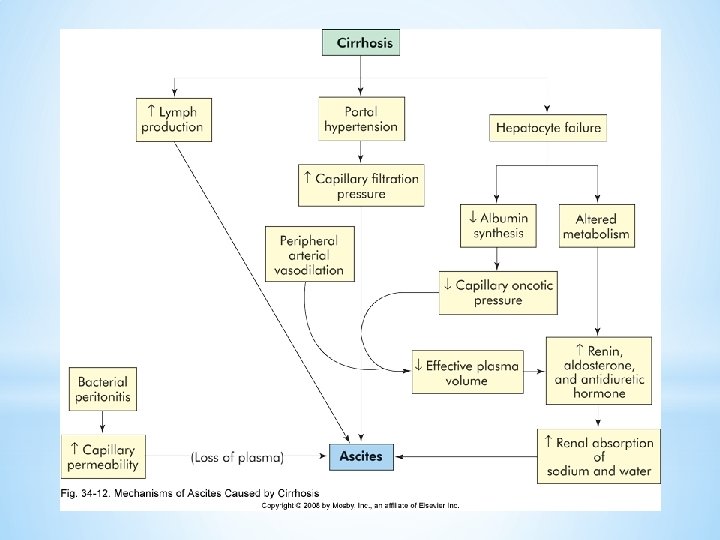
* Blood is forced back up to the surrounding circulation causing PORTAL HYPERTENSION * Blood backs up to the… * Spleen- causing splenomegaly=anemias, thrombocytopenia * Esophageal vessels- esophageal varices * Rectal vessels- hemorrhoids The resistance to blood creates ASCITES The Circulation is now exposed to toxins! *

*The liver synthesizes albumin… *The liver synthesizes prothrombin and fibrinogen

* Insufficient amounts of albumin in the vascular space allows fluid to seep into the tissues = peripheral edema. When circulating volumes are low, which two hormones are released to try and remedy this? *Patients are susceptible to bleeding and bruising with insufficient quantities of prothrombin and fibrinogen. . *

*Bile is formed by the liver and stored in the gallbladder. *Bile is necessary for the absorpsion of fats and fat soluble vitamins. *

*The patient has intolerance to fatty foods = NAUSEA, GI UPSET The pt can not absorb fat soluble vitamins like A, E, D, and K. WHAT HAPPENS WHEN YOU CAN’T ABSORB VITAMIN K? !!!!!! *

*Bilirubin is released in the process of breaking down RBCs. It then travels to the liver bound with albumin and it is transformed into a form that will allow it to cross the liver cell to make bile = CONJUGATION. * (So, it’s transformed from a fat soluble form that is unable to cross the hepatocyte into a water soluble form that the liver can use to make bile. )

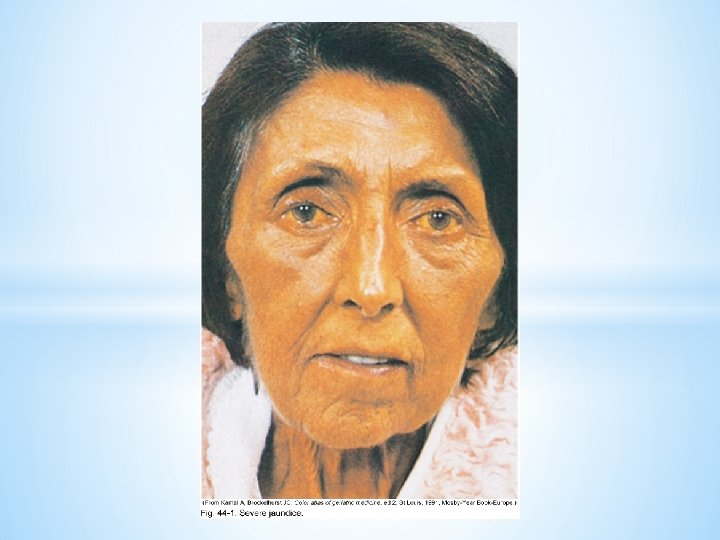
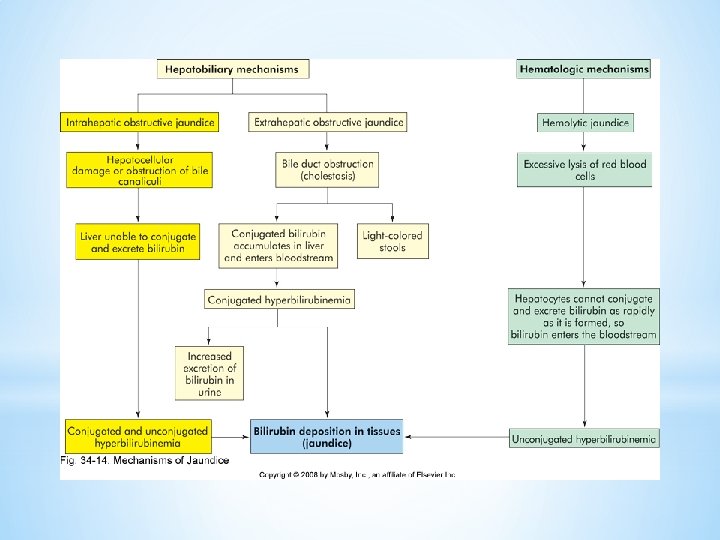
*Bilirubin is not made into its usable form. Bile is not made from bilirubin and this unconjugated bilirubin is left to seep into the tissues. The skin absorbs this bilirubin = JAUNDICE & PRURITIS. *When bile is not made from bilirubin and emptied into the duodenum for digestion our stool loses pigment = CLAY COLORED STOOLS. *

* Jaundice a yellowish discoloration of body tissue, results from an alteration in normal bilirubin metabolism of flow of bile into hepatic or biliary duct systems. (it is symptom rather than disease) * Hemolytic Jaundice is due to an increased breakdown of RBC, which produces an increased amount of unconjugated bilirubin in the blood. * Hepatocellular Jaundice results from the liver’s altered ability to take up bilirubin form the blood or to conjugate or excrete it. * Obstructive jaundice is due to impeded or obstructed flow of bile through the liver or biliary system. Obstruction could be intrahepatic or extrahepatic *

*Proteins in the gut are acted upon by the normal bacteria present there = degradation… and ammonia (NH 3) is the by-product. * The portal circulation carries the waste filled blood to the liver where ammonia is converted to urea. Urea is a waste product that is easily excreted by the kidneys. *

*Ammonia builds up b/c the liver can not convert into urea. NH 3 crosses blood-brain barrier and is a CNS toxin causing lethargy, confusion…. -coma. HEPATIC ENCEPHALOPATHY *What effect do you think that bleeding esophageal varices has on this problem? *

*The liver transforms and/or inactivates meds and hormones like *ALDOSTERONE *ESTROGEN *TESTOSTERONE *

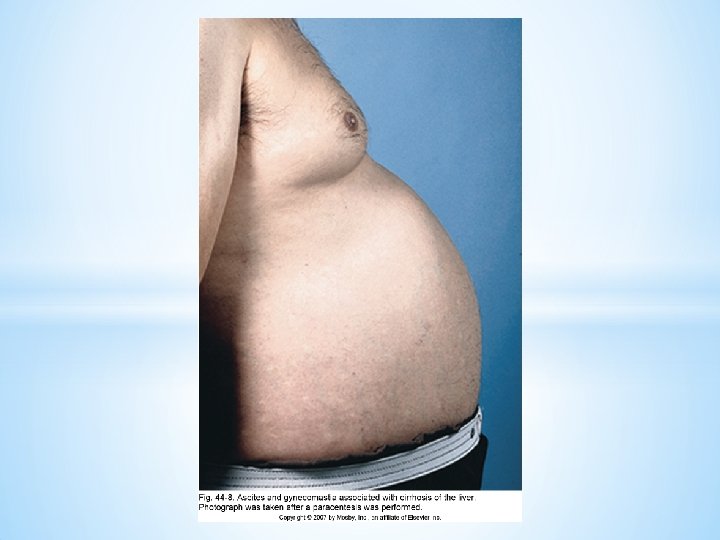
* There is an increase in circulating Aldosterone. Body will hold on to even more Na+ and water. What clinical manifestations will you see? * Increases in estrogen in males will lead to development secondary sex characteristics. * PECTORAL ALOPECIA * GYNECOMASTIA * TESTICULAR ATROPHY * IMPOTENCE * PALMAR ERYHTEMA * Greater sensitivity to drugs like tylenol and ETOH. * of

1. Esophageal Varices 2. Ascites 3. Hepatic Encephalopathy What to do? *

Esophageal Varices *
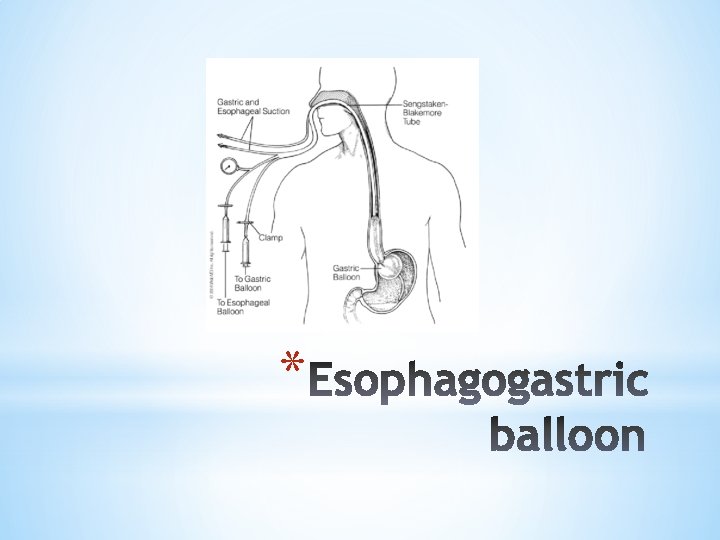
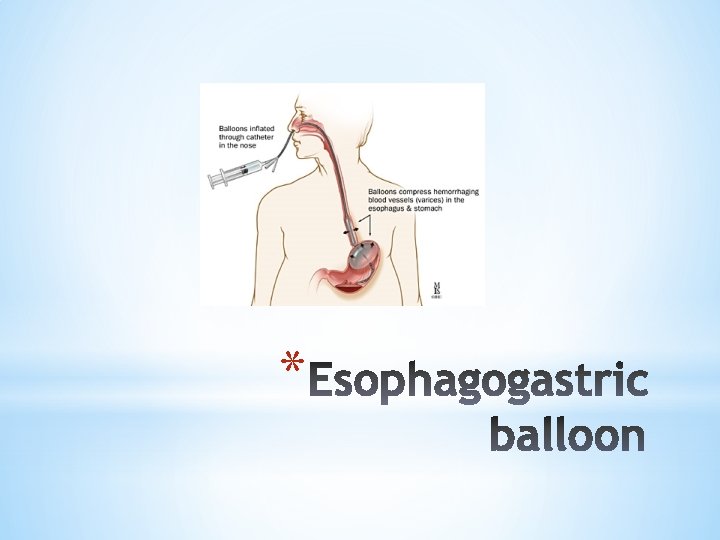
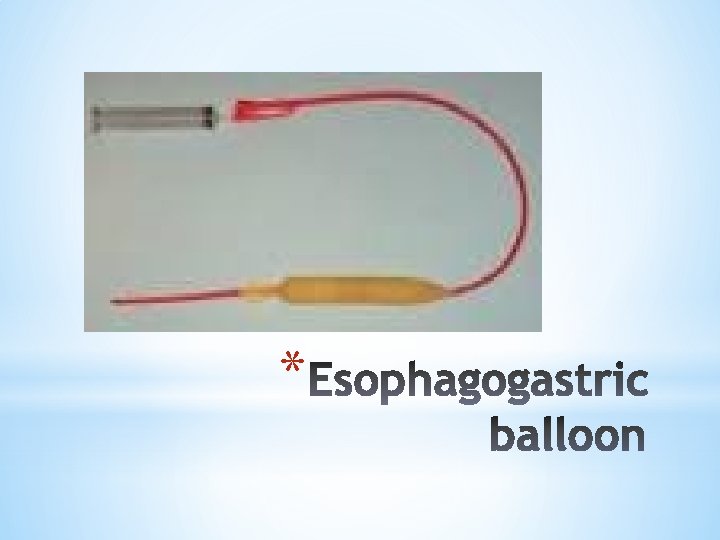
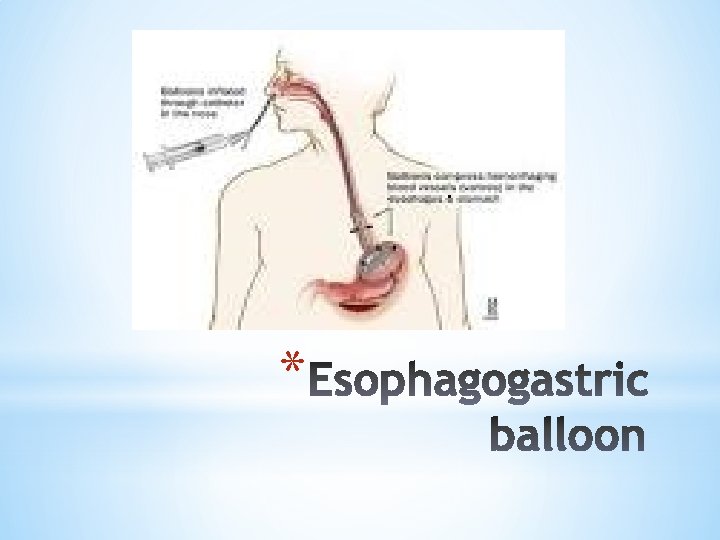
- vasopresses surrounding vessels *Endoscopic sclerotherapy or ligation Implications? *Balloon")
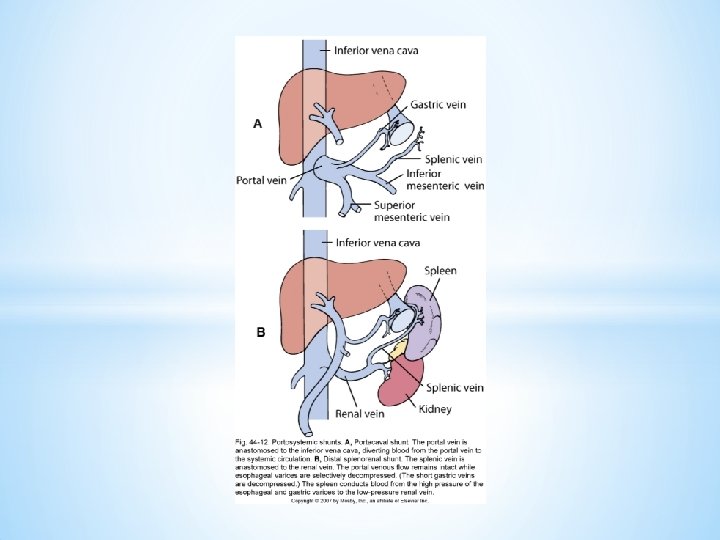
*B-adrenergic blockers- why? *Sandostatin (octreotide)- vasopresses surrounding vessels *Endoscopic sclerotherapy or ligation Implications? *Balloon tamponade Explain. What NEEDS to go at the bedside? *Surgical shunting procedure what is shunted? What’s made worse? (Transjugular intrahepatic portosystemic shunt) *


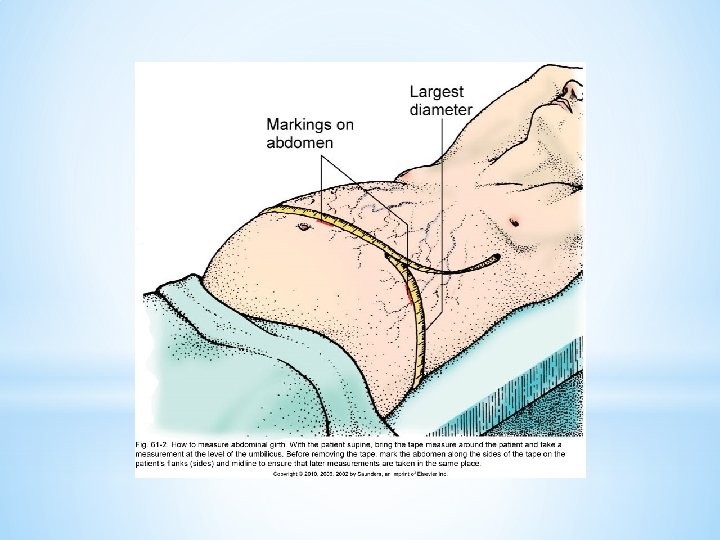
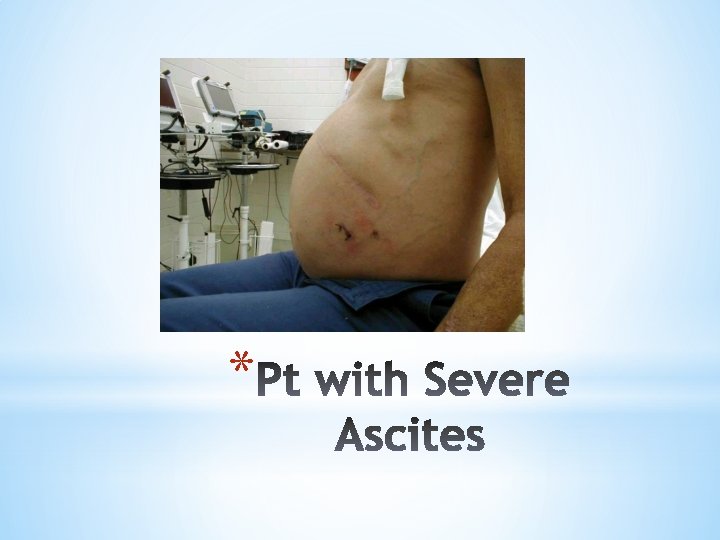
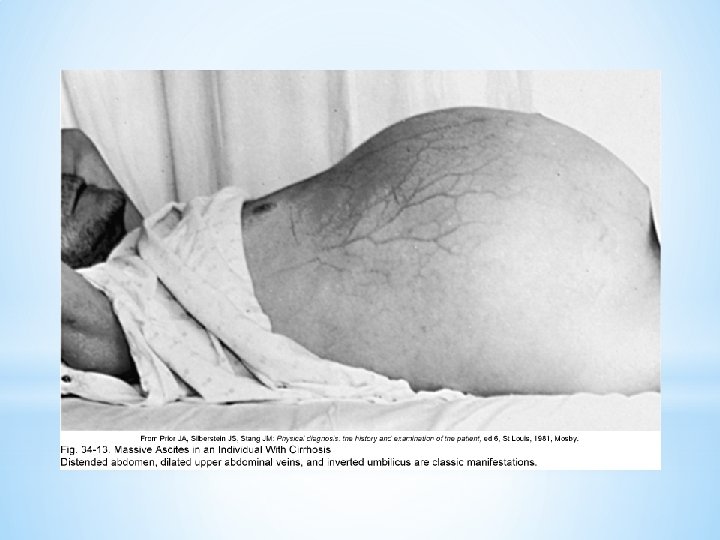
ASCITES *

*Paracentesis-needle puncture of the abdominal cavity to remove fluids in pt with severe ascites and respiratory problems *Peritonovenous shunt -provides continuous reinfusion of ascitic fluid into the venous system (dialysis) *
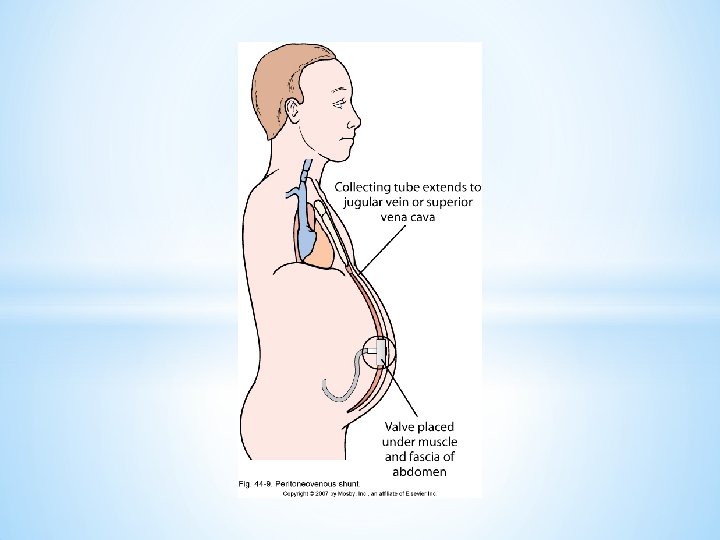

*Paracentesis- potential complications? *Peritonovenous shunt -potential complications? *

What to do? �Give Lactulose- purge the gut of ammonia forming wastes (goal is 2 -3 soft stools/day) �Give Magnesium Citrate -Laxative= purge the gut! �Back off on protein in your diet Why? ? �Give Neomycin Sulfate- antibiotic that’s absorbed only in the gut. It kills the bacteria that acts on he protein that has ammonia as the by-product.
 SGOT (serum glutamic oxaloacetic transaminase) 3. ALT")
1. Alkaline phosphate 2. AST (Aspartate aminotransferase) SGOT (serum glutamic oxaloacetic transaminase) 3. ALT (alanine aminotransferase) SGPT (serum glutamate pyruvate transaminase) 4. GGT (gamma glutamyl transferase) *

*Bilirubin, total, unconjugated, conjugated *Ammonia *PT/INR *H/H *Platelets *Albumin *NH 3 *

*B-complex vitamins- WHY? *Rest WHY? *Avoidance of alcohol and aspirin-- WHY? *Management of ascites (sodium restriction) WHY? *Diuretics WHY? * Lasix * Aldactone *

*HRS is a serious complication of cirrhosis THE LIVER IS FAILED AND THE KIDNEY The kidney can no longer keep up with the wastes not metabolized by the liver! Renal failure is relieved by a liver transplantation. * *

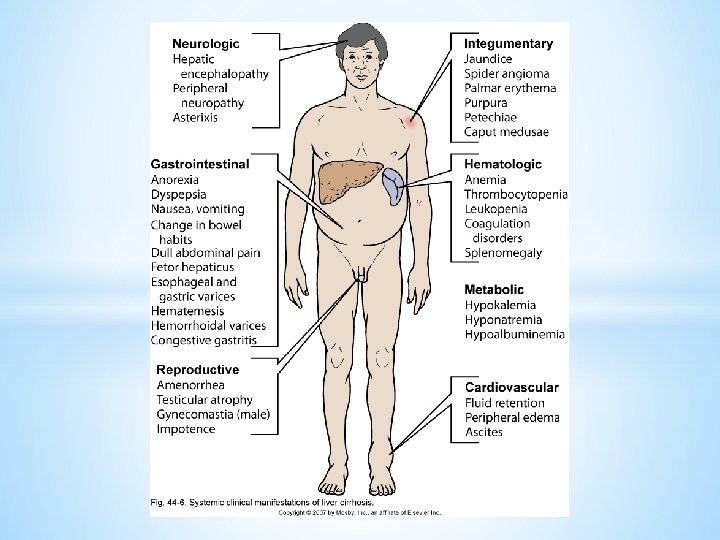
*Jaundice *petechia * spider angiomas *shallow, rapid respiration, *A LOC *Gynecomastia *thrombocytopenia *High prothrombin time *Edema. . peripheral *
- Slides: 53