By Dr Tanmoy Majumder 3 rd yr PGT

By Dr Tanmoy Majumder 3 rd yr PGT, Dept Of Paediatric medicine Calcutta national medical college

� B/O Sahanara Parveen, nine day old male term baby admitted on day 9 of life with C/O drowsiness for two days which is gradually increasing along with refusal to feed.

� The baby was delivered at Kakdwip SSH by normal vaginal delivery at 39 completed gestational wks. � Birth weight was 2. 6 kg. � Baby cried at birth. � Baby was on breast feeding since birth.

� As per mother baby was apparently well till 7 days of life and was breast feeding normally. � Then mother noticed that baby was becoming increasingly lethargic and not taking feed well and also there was less spontaneous eye opening. � Child was not crying or active as per mother. � There is no history of rise of temperature or convulsion. � Stool and urine passed normally.

� Mother is a primigravida. � 22 yrs old , belongs to low socioeconomic conditions. � No H/O of consanguinity. � Mother taken IFA tablet regularly. � No significant H/O of drug intake antenatal period. � No H/O of fever, rash, joint pain in antenatal period. � NO history of hypertension, gestational diabetes.

� No family H/O of congenital anomaly or any neurological disease. � There is H/O of 2 abortions in elder sister of mother.

� Baby’s colour was pink, periphery was warm. � Heart rate=134/minute. � Respiratory rate=43/minute. � Capillary refill time <3 seconds. � Spo 2 96% on room air. � CBG=72 mg/dl.

� Weight=2. 7 kg. (weight is between 3 rd and 50 th percentile a per WHO growth chart) � Length=49 cm(height for age is between 3 rd and 50 th percentile as per WHO growth chart) � HC=32 cm(Head circumferance as per age is less than 3 rd percentile as per IAP- WHO growth chart). � Head size of both parents was normal.

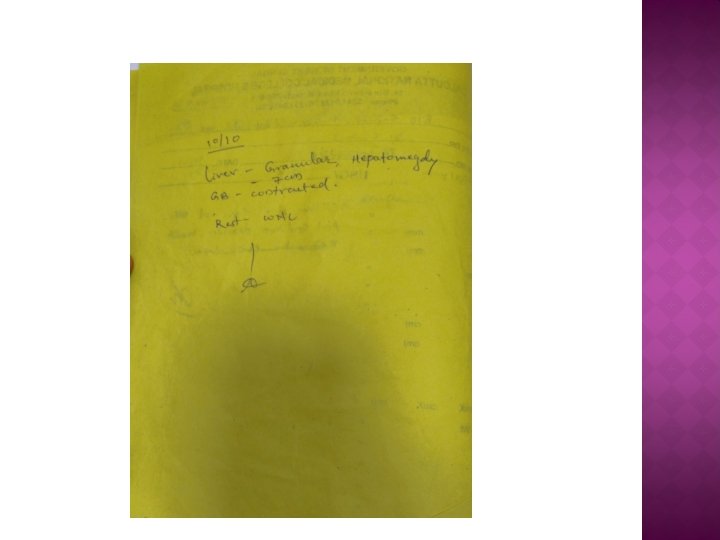
Head to toe examination � Facies normal. � No change in hair colour, � No obvious eye changes/skin changes � Spine: normal � Respiratory system=NAD � GI system = hepatomegaly( liver span: 6 cm) � CVS =NAD

� Baby was lethargic. � Responding to painful stimulus only. � Microcephaly was present. � Anterior fontanelle was open but not bulged, size 2. 5 x 2 cm. � posterior fontanelle was also open. � Tone was decreased.

� Congenital hypothyroidism. � Neonatal sepsis. � Electrolyte imbalance. � Inborn error of metabolism. � Congenital infection. � Genetic disorder.

� Serum TSH was sent. � Blood culture was sent and empirical antibiotics started. � Serum electrolytes were sent.
.")
� Initially � IV treatment started with FLUIDS � IV ANTIBIOTICS(AMPICILLIN).

� BLOOD SAMPLES sent for � Complete blood count. � CRP. � Urea, creatinine. � Blood ammonia level. � Planned for IEM panel. � TORCH screening.

� Pts remains almost same, no rise of temperature, not taking feed, non arousable… � Blood reports shows � Total count=18, 400/cmm. � Hb=18 gm/dl. � Na=93 m. Eq/L, k=5. 4 m. Eq/L, Ca=1. 31 m. Eq/l � Urea=18 mg/dl, Creatinine=0. 9 mg/dl.

� It was a case of HYPONATREMIA � We � To started IV sodium correction. rule out late onset sepsis, we performed CSF study which came out to be normal.

� Even after sodium correction, patient remained lethargic. Repeat Na=128 m. Eq/L � CBG was normal during the entire course. � Thyroid screening came to be Normal. � TORCH Screening: Negative(mother&baby)

. Then we performed a")
� Blood ammonia level high on day 3 evening(250 U/L). Then we performed a Arterial blood gas considering strong suspicion of IEM…. p. H=7. 280 Hco 3=18 mmol/L. p. CO 2=43 mm. Hg Na =134 mmol/L p. O 2= 102 k =4. 6 mmol/L Then we send blood for IEM panel.

� On Day 5: oral feeding started and baby was gradually improving but still the baby remains excessive sleepy and activity was not upto mark.

� The baby was improving gradually, on antibiotics. � Awaiting for IEM panel. � Which came on day 15.

� On DAY 15 of admission IEM Pannel reports came to our hand which shows…. Carnitine palmitoyl transferase II(CPT 2)deficiency or Carnitine: Acylcarnitine Translocase Deficiency
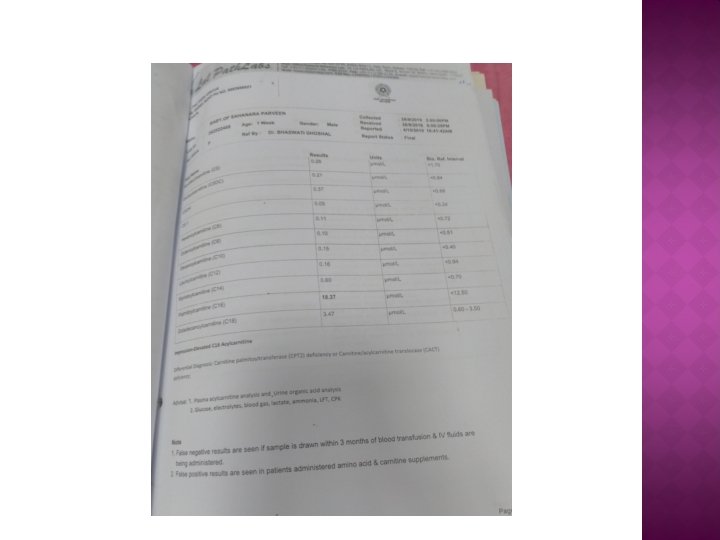

� So finally we diagnosed it as a case of INBORN ERROR OF METABOLISM due to Carnitine Palmitoyl transferase II or Carnitine: Acylcarnitine Translocase deficiency presenting with hyponatremia, lethargy, microcephaly and hepatomegaly. � We then started L-carnitine therapy orally.

� We also undergone further investigations � USG W/A shows hepatomegaly, kidney =WNL. � USG cranium =NAD. � Echocardiography shows=tiny foramen ovale otherwise NAD. � LFT Shows Bilirubin=2. 57 mg/dl(conjugated 1. 50 mg/dl), AST=368 U/L, ALT=86 U/L. � CPK =130 U/L � Repeat electrolyte , CBC returns to normal limit.

� Baby was finally discharged on day 29 of life, baby was taking breastfeeding normally then. � Baby was discharged on oral Lcarnitine. (Dose 100 mg/kg/day but we started at low dose 50 mg/kg/day)

� The infant was reviewed at 5 month of age , � vital: stable. � Wt=6. 5 kg. � Length=60 cm, � HC=38 cm. � Developmental milestones are as per age. � No significant illness in between. � Repeat USG W/A =NAD. � Echocardiography =NAD.

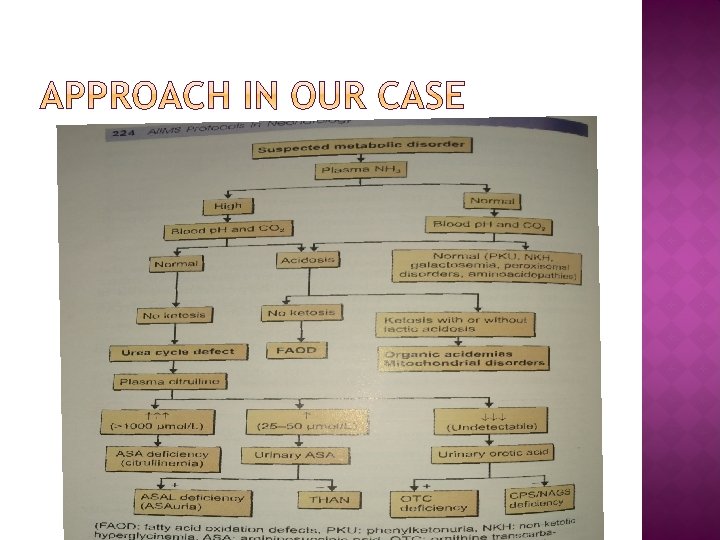

suspected metabolic disorder � plasma NH 3 HIGH NORMAL BLOOD Ph and Co 2 NORMAL ACIDOSIS NO KETOSIS FAOD IEM PANEL

It is the most common type of mitochondrial fatty acid oxidation disorder. � Autosomal recessive disease. � CPT 2 main function is transesterification of long chain fatty acid that allows inner mitochondria transport where β-oxidation take place. � There is mainly 3 types of presentation…. � � The severe neonatal lethal form is associated with severe enzyme deficiency presenting with encephalopathy, dysplastic kidney, cerebral malformation.

� The second adult presentation is associated with episodic rhabdomyolysis, 1 st episode usually not occurred until late childhood or early adulthood, attack may be precipitated by prolonged exercise. � The third intermediate form of CPT 2 deficiency presents in infancy or childhood with fasting induced hepatic failure, cardiomyopathy and skeletal myopathy with hypoketotic hypoglycaemia. But does not have the severe developmental changes seen in neonatal lethal presentation.

� This is defect of inner mitochondrial membrane carrier proteinfor fatty acylcarnitine s blocks entry of long chain fatty acid for oxidation. � Anewborn may presents with fasting induced hypoglycaemia, hyperammonemia and cardiorespiratory collapse. � Several patients with partial translocase deficiency and milder disease without cardiac involvement have been identified. � Diagnosis can be confirmed by genetic analysis.

� Every newborn presents with sudden onset deterioration with unexplained sleepiness should always be screened for INBORN ERROR OF METABOLISM. � Counselling regarding future pregnancy Should be done.

THANK YOU
- Slides: 39