By Dr Samah M Shehata Associate Prof of

By Dr. Samah M. Shehata Associate Prof. of Chest Diseases Faculty of Medicine Zagazig University

Case history A 66 -year-old man with a smoking history of 1 pack per day for the past 47 years presents with progressive shortness of breath and chronic cough, productive of yellowish sputum, for the past 2 years. On examination he appears cachectic and in moderate respiratory distress, especially after walking to the examination room, and has pursed-lip breathing. His neck veins are mildly distended. Lung examination reveals a barrel chest and poor air entry bilaterally, with moderate inspiratory and expiratory wheezing. Heart and abdominal examination are within normal limits. Lower extremities exhibit scant pitting edema.

Definition of COPD v v COPD, a common preventable and treatable disease, is characterized by persistent (not fully reversible) airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and Healthy Alveolus COPD

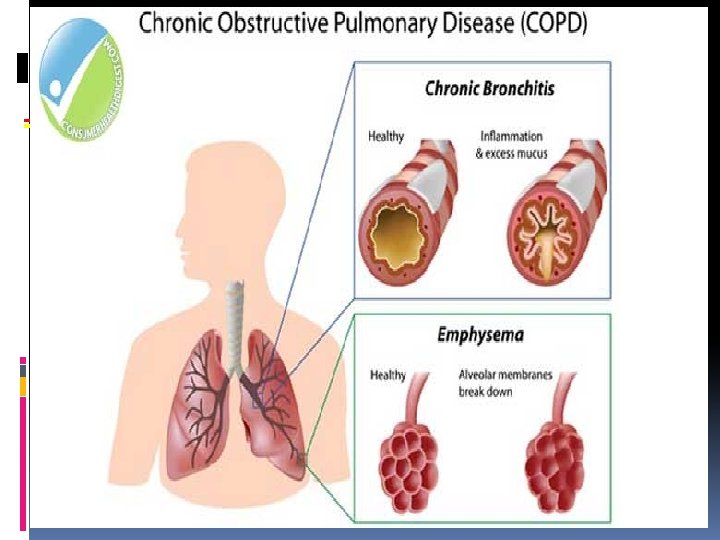
Pathologic Types

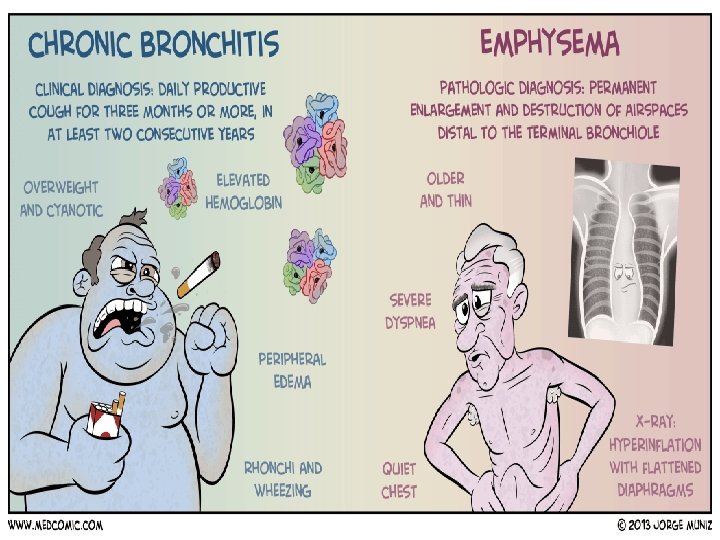
Emphysema Description Abnormal permanent enlargement of the air space distal to the terminal bronchioles Accompanied by destruction of air space

Emphysema

Chronic Bronchitis Description Presence of chronic productive cough for 3 or more months in each of 2 successive years in a patient whom other causes of chronic cough have been excluded

Risk Factors for COPD Genes Infections Socio-economic status Aging Populations

Non-Smoker l Smoking causes 80 -90% of COPD. l 50% of smokers develop chronic bronchitis l 15 -20% of smokers develop clinical airflow obstruction (COPD)

Causes of COPD Tobacco smoking is the main risk factor for COPD, although other inhaled noxious particles and gases may contribute. In addition to inflammation, an imbalance of proteases and anti- proteases in the lungs, and oxidative stress are also important in the pathogenesis of COPD ERS-ATS COPD Guidelines

COPD Infection Major contributing factor to the aggravation and progression of COPD Heredity -Antitrypsin (AAT) deficiency (produced by liver and found in lungs); accounts for < 1% of COPD cases Emphysema results from lysis of lung tissues by proteolytic enzymes from neutrophils and macrophages

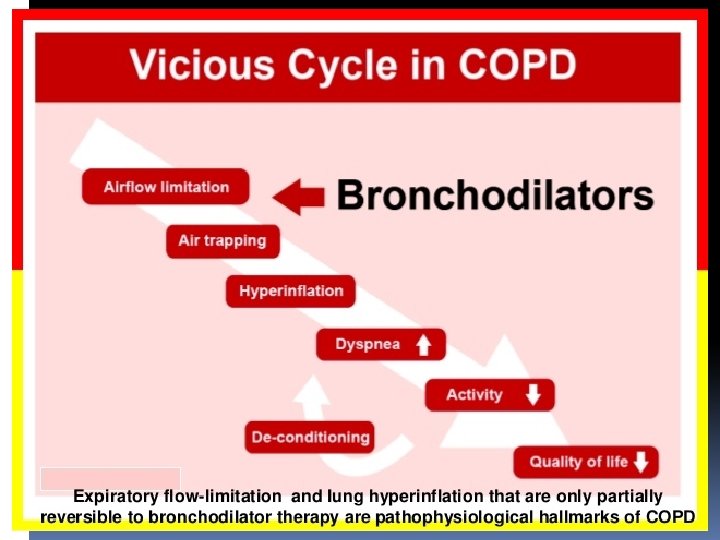
Mechanisms Underlying Airflow Limitation in COPD Small Airways Disease • Airway inflammation • Airway fibrosis, luminal plugs • Increased airway resistance Parenchymal Destruction • Loss of alveolar attachments • Decrease of elastic recoil AIRFLOW LIMITATION

Pathophysiology of Chronic Bronchitis and Emphysema

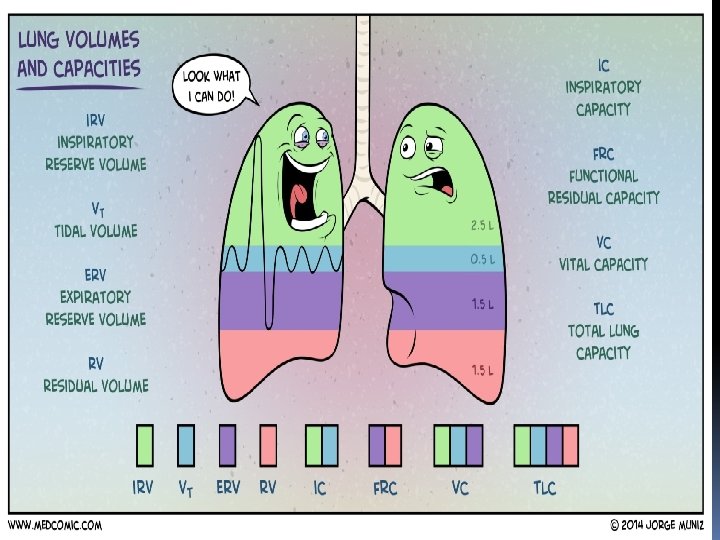
Emphysema Pathophysiology Hyperinflation of alveoli Destruction of alveolar walls Destruction of alveolar capillary walls Narrowed airways Loss of lung elasticity

Clinical Picture of COPD Cough Expectoration Wheeze, breathlessness Chest tightness Chest pain Haemoptysis
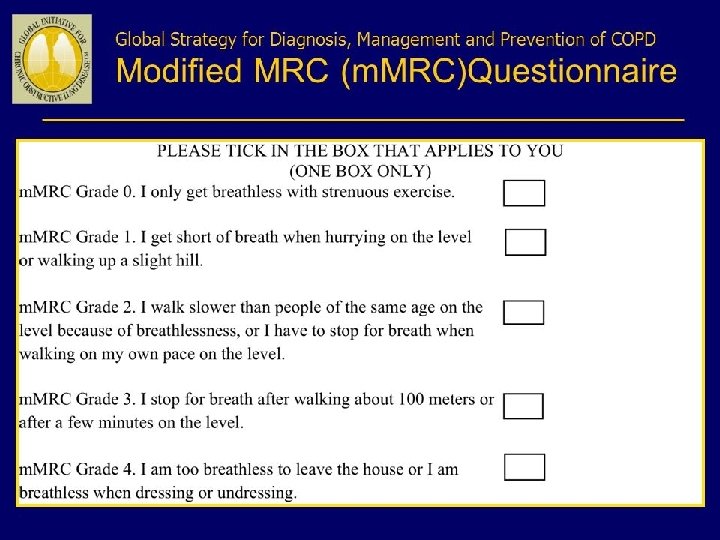

Sign of COPD Inspection/Palpation ↑RR breathing pattern Use of accessory muscles Cyanosis , flapping tremors Barrel chest , tracheal tug Litten ‘s sign, Bilateral Diminished chest expansion
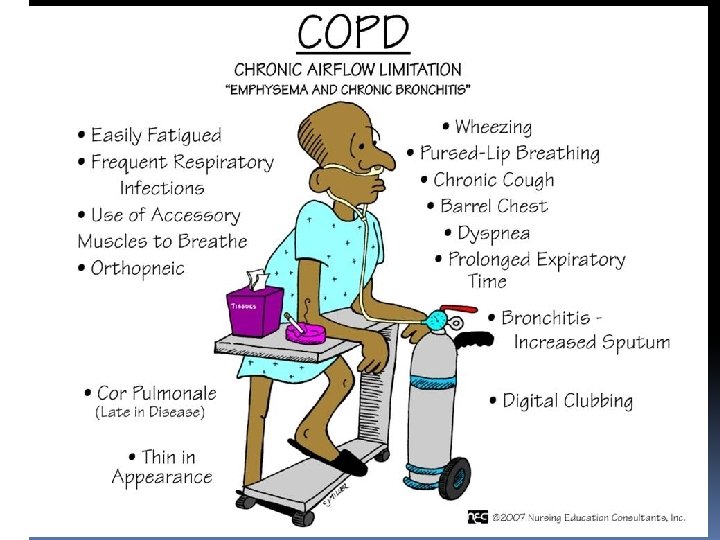

*Percussion : Hyperresonant depressed diaphragm, diminution of the area of absolute cardiac dullness. *Auscultation: Prolonged expiration ; reduced breath sounds; The presence of wheezing during quiet breathing Crackle can be heard if infection exist. The heart sounds are best heard over the xiphoid area.

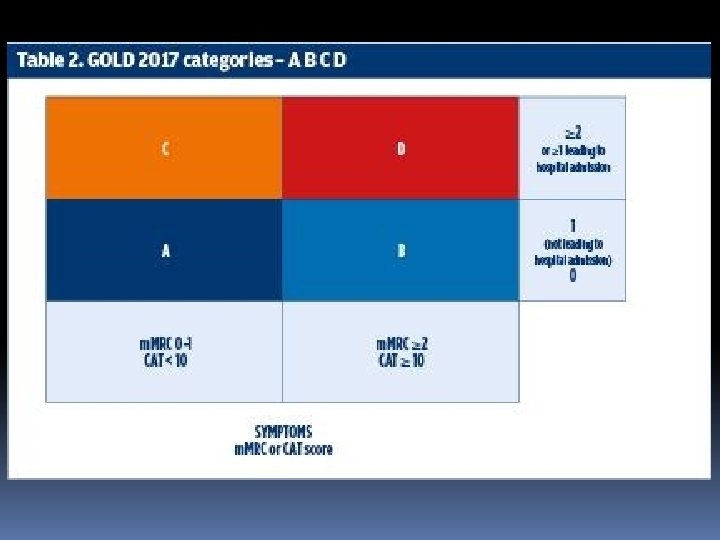
Diagnosis of COPD SYMPTOMS cough sputum shortness of breath EXPOSURE TO RISK FACTORS tobacco occupation indoor/outdoor pollution SPIROMETRY

Spirometry

Chest X-ray üChest findings are also variable. üMarked over inflation is noted with flattend and low diaphragm üIntercostal space becomes widen üA horizontal pattern of ribs üA long thin heart shadow üDecreased markings of lung peripheral vessels

Chest X-Ray

C. X-ray Ch Bronchitis Non apparent abnormality Thickened and increased of the lung markings are noted.
 greater sensitivity and specificity for emphysema than CXR , especially for")
CT (Computed tomography) greater sensitivity and specificity for emphysema than CXR , especially for the diagnosis of bronchiectasis and evaluation of bullous disease

Computed Tomography
")
COPD Diagnostic Studies ABGs Pa. O 2 Pa. CO 2 (especially in chronic bronchitis) p. H (especially in chronic bronchitis) Bicarbonate level found in late stages COPD

COPD Complications Pulmonary hypertension Cor pulmonale (Rt ventricular enlargment + failure resulting from dis. that affect structure or function of the lungs) Pneumonia Pneumothorax Acute Respiratory Failure Lunge cancer Bronchiectasis

Other presentations

Other presentations include weight loss, hemoptysis, cyanosis, and morning headaches and asterixis secondary to hypercapnia. Physical examination may demonstrate hypoxia, use of accessory muscles, paradoxical rib movements, distant heart sounds, lower-extremity edema and hepatomegaly secondary to cor pulmonale, Patients may also present with signs and symptoms of COPD complications e. g. severe shortness of breath, severely decreased air entry, and chest pain secondary to an acute COPD exacerbation or spontaneous pneumothorax. Patients with COPD often have other comorbidities, including cardiovascular disease, skeletal muscle dysfunction, metabolic syndrome and diabetes, osteoporosis, depression, lung cancer, gastroesophageal reflux disease, bronchiectasis, and obstructive

Differential Diagnosis: COPD and Asthma COPD • Onset in mid-life • • Symptoms slowly progressive Long smoking history ASTHMA • Onset early in life (often childhood) • Symptoms vary from day to day • Symptoms worse at night/early morning • Allergy, rhinitis, and/or eczema also present • Family history of asthma
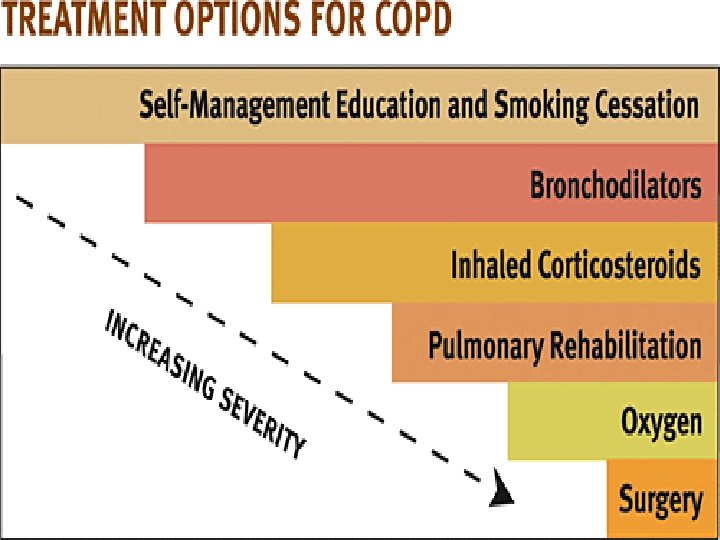
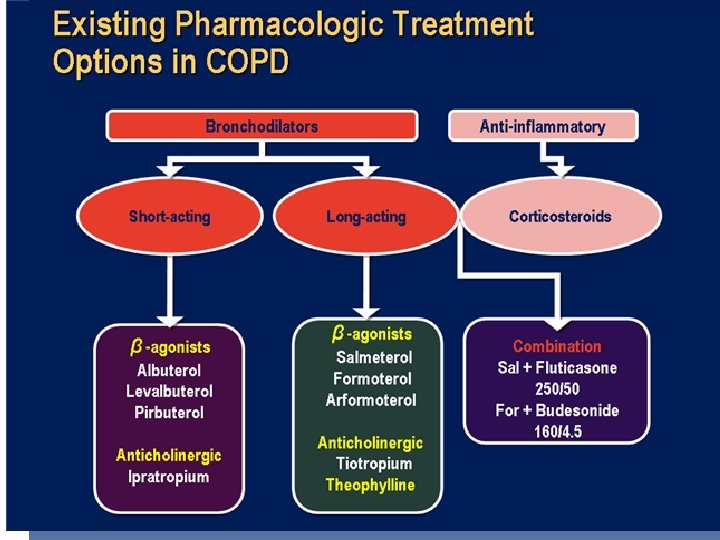

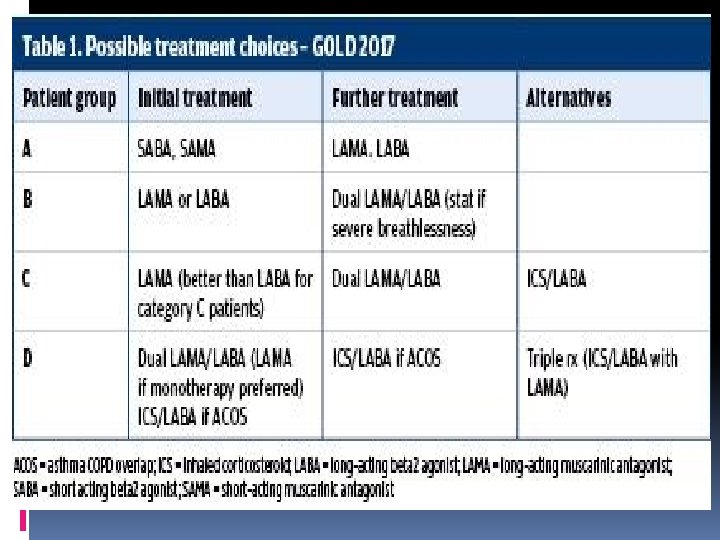
Therapeutic Options: COPD Medications Beta 2 -agonists Short-acting beta 2 -agonists Long-acting beta 2 -agonists Anticholinergics Short-acting anticholinergics Long-acting anticholinergics Combination short-acting beta 2 -agonists + anticholinergic in one inhaler Methylxanthines Inhaled corticosteroids Combination long-acting beta 2 -agonists + corticosteroids in one inhaler Systemic corticosteroids Phosphodiesterase-4 inhibitors

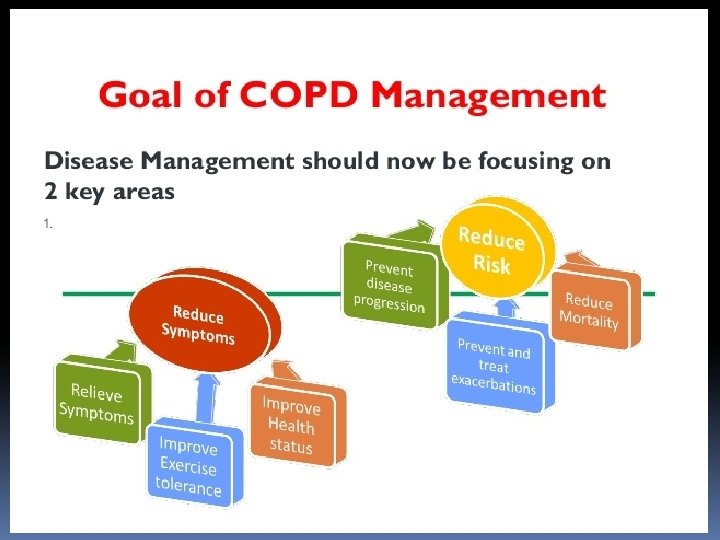
Therapeutic Options: Key Points Smoking cessation has the greatest capacity to influence the natural history of COPD Pharmacotherapy and nicotine replacement reliably increase long-term smoking abstinence rates. All COPD patients benefit from regular physical activity should repeatedly be encouraged to remain active. Appropriate pharmacologic therapy. Influenza and pneumococcal vaccination should be offered depending on local guidelines.

Therapeutic Options: Other Pharmacologic Treatments v. Influenza vaccines can reduce serious illness. Pneumococcal polysaccharide vaccine is recommended for COPD patients 65 years and older and for COPD patients younger than age 65 with an FEV 1 < 40% predicted. v. The use of antibiotics, other than for treating infectious exacerbations of COPD and other bacterial infections, is currently not indicated.

Therapeutic Options: Other Pharmacologic Treatments Alpha-1 antitrypsin augmentation therapy: not recommended for patients with COPD that is unrelated to the genetic deficiency. Mucolytics: Patients with viscous sputum may benefit from mucolytics; overall benefits are very small. Antitussives: Not recommended. Vasodilators: Nitric oxide is contraindicated in stable COPD. The use of endothelium-modulating agents for the treatment of pulmonary hypertension associated with COPD is not recommended.

Oxygen Therapy Chronic O 2 therapy at home Improved prognosis Improved neuropsychologic function Increased exercise tolerance Decreased hematocrit Reduced pulmonary hypertension

Therapeutic Options: Other Treatments Oxygen Therapy: The long-term administration of oxygen (> 15 hours per day) to patients with chronic respiratory failure has been shown to increase survival in patients with severe, resting hypoxemia. Ventilatory Support: Combination of noninvasive ventilation (NIV) with long-term oxygen therapy may be of some use in a selected subset of patients, particularly in those with pronounced daytime hypercapnia.
 is more efficacious than medical")
Therapeutic Options: Surgical Treatments Lung volume reduction surgery (LVRS) is more efficacious than medical therapy among patients with upper-lobe predominant emphysema and low exercise capacity. LVRS is costly relative to health-care programs not including surgery. In appropriately selected patients with very severe COPD, lung transplantation has been shown to improve quality of life and functional capacity.

Manage Exacerbations An exacerbation of COPD is: an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal dayto-day variations and leads to a change in medication. ”

Manage Exacerbations: Treatment Options Oxygen: titrate to improve the patient’s hypoxemia with a target saturation of 88 -92%. Bronchodilators: Short-acting inhaled beta 2 agonists with or without short-acting anticholinergics are preferred. Systemic Corticosteroids: Shorten recovery time, improve lung function (FEV 1) and arterial hypoxemia (Pa. O 2), and reduce the risk of early relapse, treatment failure, and length of hospital A dose of 30 -40 mg prednisolone per day for 7 days is recommended. stay.

Manage Exacerbations: Treatment Options Antibiotics should be given to patients with: Three cardinal symptoms: increased dyspnea, increased sputum volume, and increased sputum purulence. Who require mechanical ventilation.
- Slides: 54