BY Dr Omar Abd AL Rheem Surgical Anatomy

BY Dr: Omar Abd AL Rheem

Surgical Anatomy n n The anal commences at the level where the rectum passes through the pelvic diaphragm and ends at the anal verge it is 3 -4 cm in length in adult. Development n n The upper fourth : Distal part of the hind gut (endodermal ). The lower part : Proctodaeum (ectodermal ).

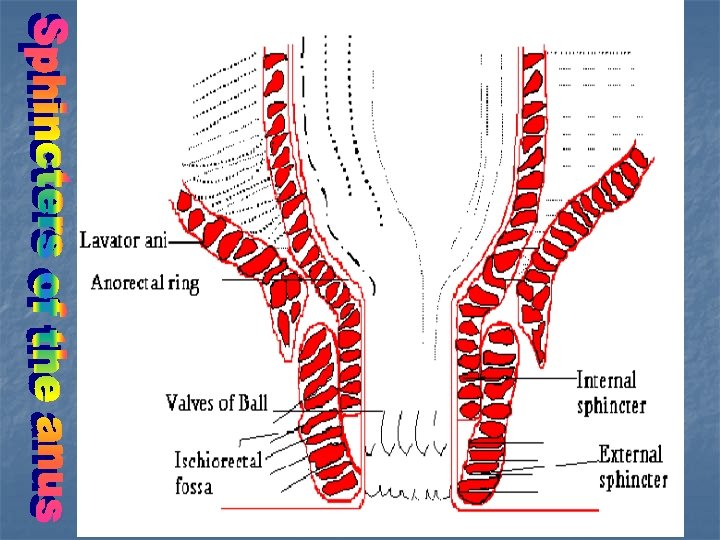
Anal canal musculature 1 -The internal sphincter n n Is a thickened continuation of the circular muscle coat of the rectum 2. 5 cm long and 2. 5 mm thick It is involuntary supplied by autonomic innervation. White in colour (raw chicken )

2 -The longitudinal muscle n n n Is the continuation of the longtudinal muscle coat of the rectum. Involuntary muscle. Its lower fibers are fanning to be attached to the anal and perianal skin where it is termed corrugator cutis ani muscle. 3 - The external sphincter n n Voluntary muscle forms the outermost muscular coat. It is formed of 3 parts , but now it is said to be one muscle. Pink in colour. Origin from the coccyx , inserted into the perineum and supplied by the pudendal nerve

4 -The intersphicteric plane n n Between the internal anal external sphincters It contains the basal parts of 8 -12 anal glands which are the potential sites of infection. 5 - The puborectalis muscle n n Maintaining the angle between the rectum and anal canal. Is the mainstay of continence. U shaped sling originating from the back of the pubis and circuled around the anal canal to form right angle between it and the rectum. Supplied by S 2 -3.

6 -The anorectal ring n n n At the anorectal junction. Formed of puborectalis , upper part of internal anal, external sphincters , and the longitudinal muscle. Its injury leading to major incontinence.

The mucous membrane FThe dentate line : n n IS the site of fusion of the hind gut with the proctodaeum. Above it , the mucosa is low columnar and insensitive. Below it , the mucosa is stratified squamous, devoid of sebaceous glands and hair. The downwards folds of the mucosa are called columns of Morgagni (8 -12 in No. ) The inferior extremities of columns of Morgagni are called the anal crypts where the anal glands open by a narrow ducts.
 Below dentate line Proctodaeum (ectodermal Low")
Above dentate line Development Lining epithelium Hindgut (endodermal) Below dentate line Proctodaeum (ectodermal Low columnar Squamous cell epithelium Venous Drainage Portal Systemic Nerve supply Visceral Somatic Lymphatic Drainage Superior rectal pre-ortic Inguinal

Blood supply FArterial n n n F n n n Superior rectal artery Middle rectal artery Inferior rectal artery inferior mesenteric internal iliac internal pudendal Venous Superior rectal v Middle rectal v Inferior rectal v inferior mesenteric v internal iliac v internal pudental v

Puborectalis
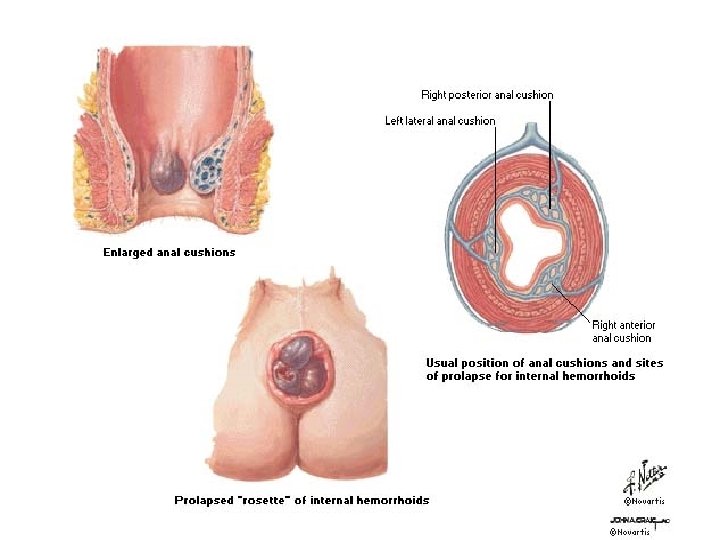

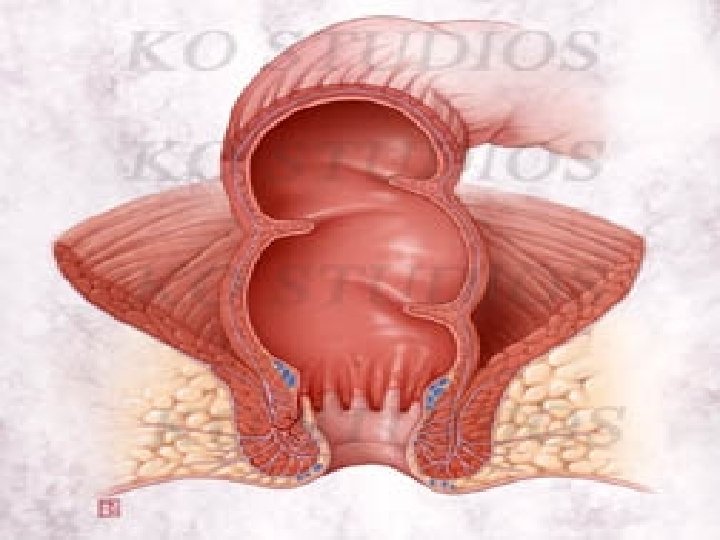
Anal Cushions n n The 3 terminal branches of the superior rectal vessels from a vascular plexus below the mucosa of the anal called the anal cushions. These cushions arranged usually at 3, 7, 11 O'clock inside the anal canal. FImportance Play an important role in continence n Their congestion and enlargement Haemorroids n

Surgial physiology Physiology of defecation 1 - Mass peristalsis movement. 2 -Sampling reflex (the distention of the rectum). 3 - Relaxation of the puborectalis and external sphincter. 4 - Increase intraabdominal pressure.

Physiology of continence F Factors maintaining continence to stool and flatus are : 1 - Anal sphincters Internal sphincter 80% of resting anal pressure n external sphincter 20% of resting anal pressure 2 - Puborectalis and anorectal angle (right angle ) n -Damage of puborectalis gross faecal incontinence. n
 Anorectal sensation n Present in stretch receptors ( in puborectalis , external sphincter")
3) Anorectal sensation n Present in stretch receptors ( in puborectalis , external sphincter and mucosal lining in the upper part of the anal canal ). 4 - Neuromuscular reflexes n In the pelvic floor and external sphincter , in relation to contraction of abdominal wall musculature during straining or coughing. 5 - Folds of Houston 3 in No. n called valves of Houston. 6 - Anal Cushions

BY Dr: Omar Abd AL Rheem

(Haemorrhoids (Piles FDefinition: In Greek , haima mean blood, while rhoos means flowing. n In Latin pila means a ball. n So , if the main complaint is bleeding called haemorrhoids or piles , if the main problem is prolapse. n

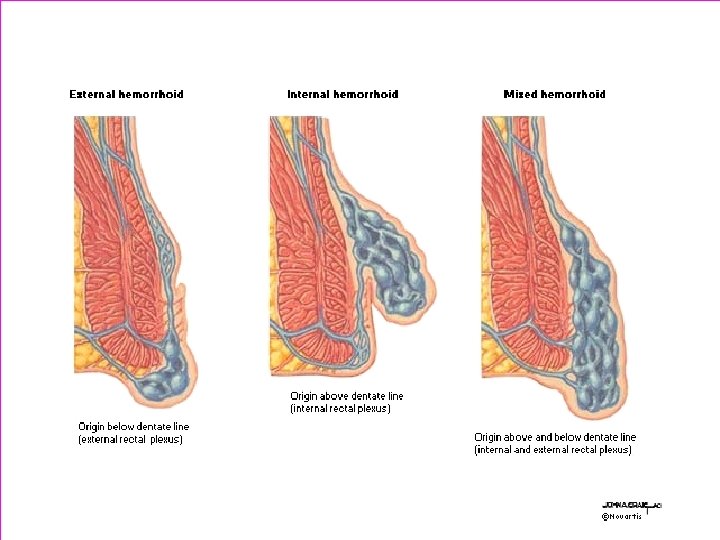
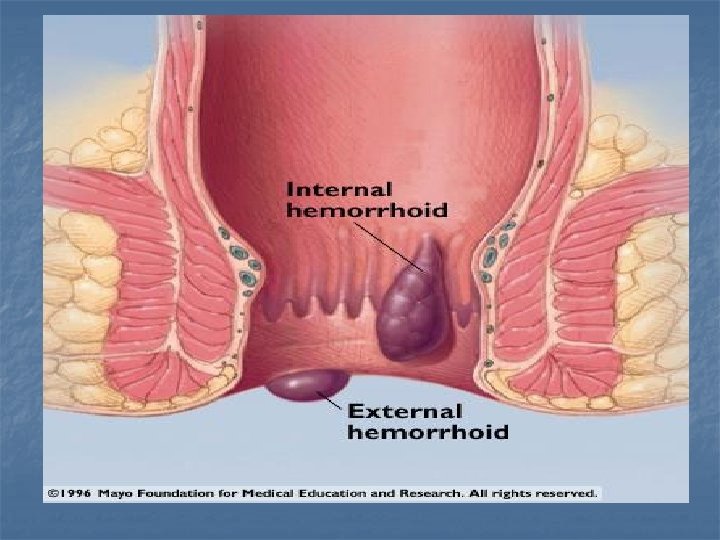
Morbid anatomy n The anal cushions play an important role in the continence mechanism. n Congestion, enlargement or prolapse of these cushions lead to haemorrhoids n -They may be internal (above the dentate line ) or external (below it ) or mixed (interno-external).
Primary haemoorrhoids n Predisposing factors : 1 - Congenital mesenchymal weakness 2 -")
Aetiology I)Primary haemoorrhoids n Predisposing factors : 1 - Congenital mesenchymal weakness 2 - Anatomical factors: The anal cushions may contribute to the development of haemorrhoids as : Ø - not supported by submucosa Ø - penetrate the internal anal sphincter that may compress its venous drainage n Ø - no valves in the portal circulation 3 - chronic straining (sliding theory)
Secondary haemorrhoids 3 P npregnancy npelvic tumour as cancer rectum nportal hypertension")
II)Secondary haemorrhoids 3 P npregnancy npelvic tumour as cancer rectum nportal hypertension

Classification into four degrees First degree n Second degree n Third degree n Fourth degree n Bleed , no prolapse Prolapse reduced spontaneously Reduced manually Permanent prolapse
Symptoms: n n n Bleeding - Fresh bright red - At the")
Clinical picture I)Symptoms: n n n Bleeding - Fresh bright red - At the end of defecation - Separate from stool Prolapse - Determine its degree Discharge Itching Soiling Pain in - Thrombosed piles - Perianal haematoma. - Associated other lesions e. g. Fissure , infection
 Signs n Proctoscopy in early cases bluish bulges. n Prolapsed piles can be")
II) Signs n Proctoscopy in early cases bluish bulges. n Prolapsed piles can be seen compressible. n PR to exclude rectal cancer. n Sigmoidoscopy in suspected high rectal cancer.


Complications Bleeding n Thrombosis n Strangulation n Ulceration n Gangrene n Suppuration n Portal pyaemia n
Primary haemorrhoids: n I and II degrees : - Conservative treatment - Injection")
Treatment I)Primary haemorrhoids: n I and II degrees : - Conservative treatment - Injection sclero -therapy - Rubber Band ligation - Photo coagulation -Cryo surgery n III and IV - Surgical Haemorrhoidectomy - Stapled Haemorroidetomy
 Secondary haemorrhoids n Treatment of the cause. III)-Treatment of complicated piles. Conservative treatment")
II) Secondary haemorrhoids n Treatment of the cause. III)-Treatment of complicated piles. Conservative treatment - High fiber diet - Laxative -Avoid Straining - Local ointment or suppositories contain -Decongestants -Astringents -Small doses of corticosteroids

Injection Sclerotherapy n n n Indications : I and II Method: 2 -3 cc of 5% phenol in almond oil are injected in the submucosa above the dentate line. Can be repeated after 2 ws. n Complications - Pain - Necrosis - Haematuria - Infection
 n n Indication: II and EARLY III")
Rubber band ligation (Barron's band ligation ) n n Indication: II and EARLY III Idea: application of elastic tight rubber band around the pedicle of the haemorrhoids ischaemic necrosis and separation Photocoagulation Infrared photocoagulation n Laser Cryo surgery n necrosis. coagulative

Surgical treatment 1 -Haemorrhoidectomy : III and IV n Transfixing ligation and excision of the main piles whether by open or closed method 2 - Stapled Haemorrhoidectomy III and IV 3 - Diathermy Haemorrhoidectomy III and IV (electrocautery) n By Harmonic scalpel or ligasure

Open hemorrhoidectomy

Closed hemorrhoidectomy
")
Closed hemorrhoidectomy (Ligasure)
")
Hemorrhoidectomy (Circular stapler)

Complications of surgery n Early - Pain - Acute retention of urine -Raectionary haemorrhage n Late - Secondary Haemorrhage - Anal fissure -Anal stenosis - Incontinence

Treatment of complicated piles 1 -Sever haemorrhage - Anticoagulant - Replacement therapy - Local compress containing adrenaline - Followed by surgery 2 - Strangulated piles - Rest - Antibiotics -Analgesics - Frequent warm baths - Decongestant ointments and local compresses by lead subacetate lotion

3 - Perianal Haematoma n n n 5 -Day , painful, self –curing lesion occurred due to rupture of dilated vein Clinically tense, tender, bluish perianal swelling Fate n n Usually resolves Suppuration Ulceration Fibrosis Treatment n n Within 36 hours urgent treatment is carried conservative
- Slides: 42