By Cori Kopecky BSN RN OCN Gemma Riccardi

By: Cori Kopecky, BSN, RN, OCN Gemma Riccardi, RN Updated 2016 Clara Cebrun, MS, RN, CPN Rhea Herrington, MSN, RN, CCRN

� Review anatomy of tracheostomy and laryngectomy � Review MD Anderson’s standards of practice and policy regarding airway management � Distinguish between early, delayed and emergent complications of tracheostomy � Identify what/service team to notify for airway patients � Identify the different supplies used for emergency bedside tracheostomy � Discuss nursing care and monitoring

Normal Airway Anatomy

Tracheostomy

Cuffed Tracheostomy – Note Balloon

Cuffless Tracheostomy – no balloon

Laryngectomy

Laryngectomy

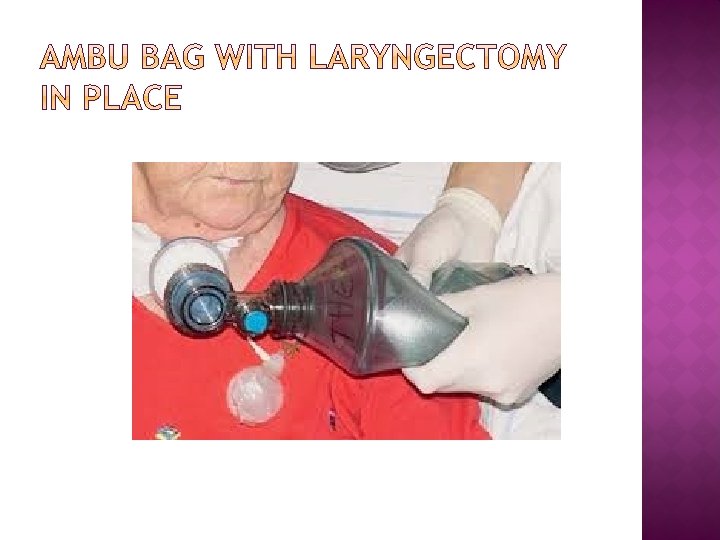
Pre and Post Laryngectomy What’s changed? - Breathes only via Stoma stoma

LARYNGECTOMY Stoma Changes: Patient breathes only through the stoma. Patient no longer breathes by Nasal passage or mouth. Oxygen or ambu bag usage is directly to the stoma.

Print and read policies for understanding of patient care: � CARE OF THE PATIENT WITH AN ALTERED AIRWAY: CLEAN TECHNIQUE POLICY(UTMDACC INSTITUTIONAL POLICY # CLN 1184) � TRACHEOSTOMY STOMA CARE AFTER DECANNULATION (UTMDACC INSTITUTIONAL POLICY # CLN 0866)

IMPORTANT: Learn the names of the parts that make up the artificial airway

Indication: � � Used for patients with tracheal problems Used for patients who are ready for decannulation Recommendation: � � � Save the decannulation plug if the patient is close to getting decannulated. Patient may be able to eat and may be able to talk without a speaking valve. Inner cannula is not disposable. You can reuse it after cleaning it thoroughly.

Indication: � � Used for patients with tracheal problems Used for patients who are ready for decannulation Recommendation: � � � Save the decannulation plug if the patient is close to getting decannulated. Patient may be able to eat and may be able to talk without a speaking valve. Inner cannula is disposable.

Indication: � Used to obtain a closed circuit for ventilation Recommendation: � Cuff should be inflated when using with ventilators. � Cuff should be inflated just enough to allow minimal air leak. � Cuff should be deflated if patient uses a speaking valve. � Cuff pressure should be checked twice a day. � Inner cannula is NOT disposable. Reusable after thorough cleaning.

� Indication: Used for patients who are on the ventilator but are not able to tolerate a speaking valve to speak � Recommendation: There is a high risk for granuloma formation at the site of the fenestration (hole). There is a higher risk for aspirating secretions. It may be difficult to ventilate the patient adequately.

� Indication: Used for patients who are on the ventilator but are not able to tolerate a speaking valve to speak � Recommendation: There is a high risk for granuloma formation at the site of the fenestration (hole). There is a higher risk for aspirating secretions. It may be difficult to ventilate the patient adequately.

Indication: � An economical, off-the-shelf alternative to custom tracheostomy tubes for patients with anatomical challenges. � Unlike most extended-length tracheostomy tubes, Shiley XLT tubes give you the choice of extra length in the proximal or distal portions for a more customized fit. Recommendation: � Disposable inner cannula (DO NOT CLEAN) � Twist and lock inner cannula

Indication: � � � Not used as frequently anymore. Many of the patients who received a tracheostomy years ago still choose to continue using the metal tracheostomy tubes. Used for long term tracheostomy needs Used for weaning/downsizing Recommendation: � � Patients cannot get a MRI. One needs to notify the security personnel at the airport prior to metal detection screening. Removable inner cannula is twist and lock. Should be cleaned at least twice daily.

Indication: � TTS – Tight to Shaft means that the cuff deflates completely to the shaft � This tube can be adjusted for horizontal and vertical shaft drop to accommodate unusual anatomy or pathology. Recommendation: � No inner cannula. � Suction to prevent secretion build up in the tube. � When cuff is deflated- the trach looks cuffless.
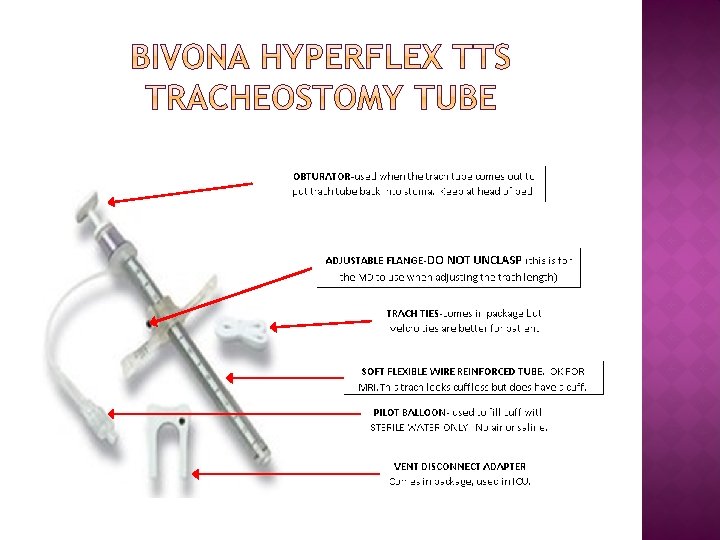

DOES NOT HAVE AN INNER CANNULA FREQUENT SUCTIONING REQUIRED � � CARE OF THE TRACH TUBE: Suction trach tube every 4 hours and as needed. Clean around the stoma and apply a clean dressing twice a day and prn. Ensure trach ties are properly secured with 1 -2 fingers under trach ties. If patient has thick secretions, consider ordering a mucolytic or an expectorant to prevent mucus plugging.

FRESH TRACH PRECAUTIONS DO NOT MANIPULATE TRACH FOR 24 HRS DO NOT REMOVE TIES OR SUTURES DO NOT REMOVE OR MANIPULATE BIVONNA TRACHEOSTOMY DATE: _________ PHYSICIAN: ______________ _ BRAND & SIZE TRACH: _________ **USE CAUTION WHEN MOVING PATIENT**

� Hydrogen peroxide � Sterile saline � Sterile gloves � Clean scissors (if ties must be replaced) � Trach brushes � Trach ties (Velcro if available) � 4" X 4" gauze or drain sponge � Cotton swabs � Suction kits

� Gather supplies – “Suction Kit” � Don PPE – clean gloves, prn (Mask, Gown) � Position patient in upright position � Stand to patient’s side

• Position patient in upright seated position – 45 degrees • Wall suctioning 110 -150 mm. Hg for adults • Sterile water from Suction Kit -Lubricate catheter • Instruct patient to take couple of deep breaths • Pass catheter up to 6 -7 inches • Rotate catheter on removal on withdrawal, not to exceed 10 seconds • Encourage cough • Repeat suctioning up to 3 passes during episode, instructing patient to take deep breaths • Clean inner cannula • Care of the Patient with an Altered Airway: Clean Technique #CLN 1184
")
� Should utilize 2 people to change and secure new tracheostomy ties (per policy) � Do not remove old tracheostomy ties before securing new ones if the procedure is done without assistance
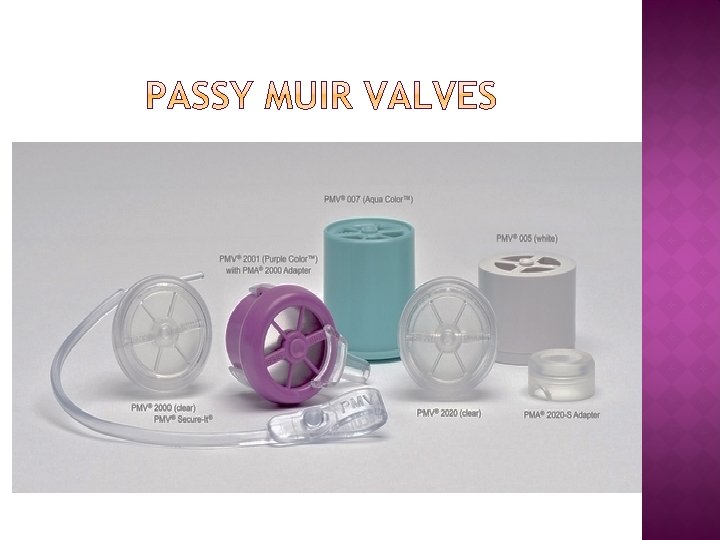

� Medical device used by tracheostomy � Redirects air flow through the vocal folds, mouth, and nose enabling voice and improved communication � Improves swallowing, secretion management and oxygenation � Contact your Speech Language Pathologist, Denise Perez for P 11 patients


� Perform hand hygiene and don PPE. � Suction airway per policy. � Inspect the stoma with a flashlight/penlight for the presence of a mucus plug or crusting. � If a mucus plug or crusting is present, instill 3 -5 m. L’s of 0. 9% Normal saline for inhalation (pt holds breath)(e. g. , saline jet) and allow the patient to cough. � If unable to clear the airway, repeat the instillation of normal saline and gently remove any crusting or plug with forceps and/or suction catheter.

� Try to remove the plug by suctioning. Saline may helpful � Remove the inner cannula � Clean inner cannula and remove any mucous plugs or blood clots � If a resuscitation bag is available, use it � Notify respiratory therapist � Deflate the cuff and try to suction again � If this does not work, cut the ties, remove the tube, and replace it with a new one

IS � Insert a clean, lubricated trach tube in the stoma using the guide (obturator) � Hold the tube in place with your fingers. � Pull out the obturator. � Replace the ties. �OBTURATOR SHOULD BE TAPED TO MIRROR IN ROOM

� Remove the inner cannula from the outer cannula � Insert obturator in the outer cannula � Insert outer cannula with obturator in stoma � Remove obturator � Insert inner cannula
 may stay open for a short")
IS NOT � � The stoma (neck opening) may stay open for a short period of time If possible, reinsert the old tracheostomy tube using obturator If you can not insert the old one, insert and hold a hollow tube such as an endotracheal tube, suction catheter, inner cannula, or straw into the stoma. Sometimes the smaller inner cannula can be inserted until emergency help arrives. If using an endotracheal tube, suction catheter, inner cannula, or straw replace with a new tracheostomy tube as soon as possible.

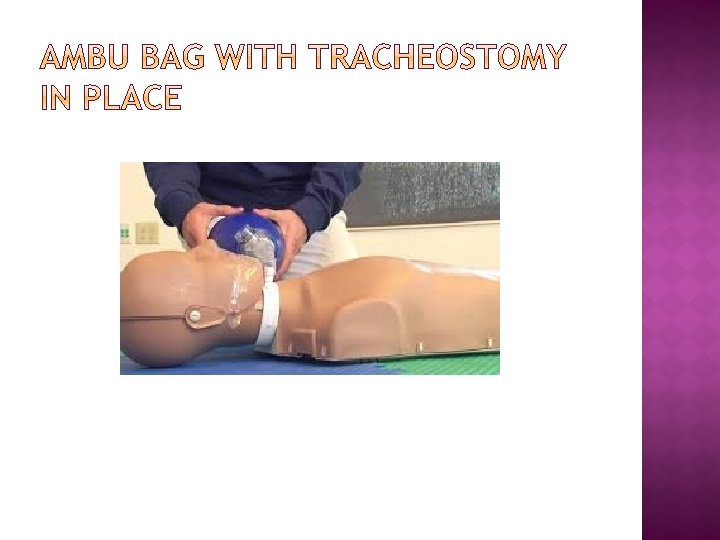
If your patient is not breathing: Prepare to provide Oxygen. If necessary, Call a Code � Attach Ambu-bag to Oxygen supply � Allow Ambu-bag to fill with oxygen then “bag patient’s airway” � Tracheostomy: Attach Ambu-bag without the mask connection directly to the tracheostomy cannula � Laryngectomy (Stoma only) : Bag stoma with Pedi-mask attached to Ambu bag Obturator

� Cardiopulmonary arrest secondary to hypoxia � Hemorrhage and injury to the thyroid gland, esophagus, laryngeal nerve, great vessels, or trachea � Pneumothorax, � False pneumomediastinum passage of the tube into the pleura, esophagus, or surrounding vessels 3

� Bleeding � Injury to recurrent laryngeal nerve � Blockage of trach tube (clots, mucus, pressure) � Bradycardia or hypotension secondary to hypoxia � Inadvertent decannulation of the tracheostomy

� Accidental � Infection � Damage decannulation: Respiratory Distress in trachea or around the tube to windpipe

� Subglottic stenosis � Granulation � Tracheal stenosis � Tracheomalacia � Tracheoinnominate artery erosion � Tracheoesophageal fistula � Aspiration and pneumonia

� Only a physician with clinical privileges to perform a tracheostomy can do this procedure � Must follow invasive procedures outside the operating room policy (policy related to universal protocol) (UTMDACC INSTITUTIONAL POLICY # CLN 0516) if non-emergent

Nursing Management, Intervention, and Documentation
")
� Daily nursing assessment of tracheostomy/airway tube, size, position documented in EHR (One. Connect) � Tracheostomy tube, size, last time inner cannula was changed, and position should be passed along in nursing shift change report � Tracheostomy care teaching can be documented in patients’ daily care plans (CPG)

Typically, nursing documentation of airway teaching includes: Ø Patient/family watching airway care video Ø Nurse demonstrates airway care (suctioning, inner cannula care, cleaning) to the patient or family Ø Patient or family attends airway care class Ø Patient or family performs hands on practice and an acceptable return demonstration of airway care

� If the patient discharges with altered airway in place, the following supplies must be ordered for the patient: �Suction kit (see tracheostomy care supplies) �Suction machine �Disposable inner cannulas �For questions, contact Charge Nurse or Case Management

� Decannulation: the process whereby a tracheostomy tube is removed once the patient no longer needs it �The initial indication for a tracheostomy no longer exists �Medical Surgical Team removes tracheostomy

� The �Is patient: alert and responsive �Manages oral secretions without risk of aspiration �Coughs and clear tracheal secretions �Tracheostomy tube downsized to 4 Shiley or “capped” and breathes without difficulty

The medical-surgical team will decannulate the patient’s airway. Supplies needed for decannualation at the bedside: � ½ inch steri-strips � Tegaderm � Benzoin � 4 x 4 gauze



Patient Education > Type in “Tracheostomy”

Patient/Caregiver Handout * Available in English/Spanish * Tracheostomy Video # 170 * Available in English/Spanish *

If you are not sure or do not know, � Clinical �X Staff on P 11 26550 or x 26555 � Patient Education Online � Respiratory � Speech Therapists ASK…. .

� 50 yr. old full code, male patient with oral cavity admitted to P 11 Head and Neck, Breast and Reconstrion � 6 Fr Shiley Tracheostomy with Obturator � Patient needs suctioning. The patient is coughing but cannot clear his airway.

� Gather Suction Kit � Suction patient as needed � Deliver humidified oxygen as needed � Is tracheostomy cannula (plugged? ) � Rinse inner cannula use trach brush � Change disposable inner cannula as needed – Do not use the trach brush � Clean and dress site as needed per policy

� Suctioning based on the patient assessment � Frequent suctioning may be necessary in a patient with a new tracheostomy or laryngectomy � Saline jet should not be used routinely for tracheostomy (use with thick or copious secretions) � Saline jet is more necessary with laryngectomy patients – dry airway � Suction according to institutional policy
")
Assemble supplies and equipment: � Tracheostomy brush (DO NOT use on disposable inner cannula) � Disposable inner cannula if indicated � Liquid soap � Hydrogen peroxide � Cotton-tipped applicators � 4 x 4 pre-cut fenestrated gauze � 4 x 4 gauze for stomal curtain � Tracheostomy tube holder with VELCRO® brand fastener (if indicated) � Suction kit with catheters � Normal saline jet(s) – mucus plugs � Wall suction with connecting tubing � Suture removal kit (if indicated)

The following equipment should be readily available for patients with Altered Airways: � Ambu bag � Extra intraluminal device of the same size � Appropriately sized suction catheter � Lubricant � 10 cc syringe � Velcro tracheostomy holder � Skin cleanser. � Non-sterile gloves. � Yankauer oral suction.

� Wall suction not functioning properly � Cannot locate pre-assembled tracheostomy kit in supply rooms (use tracheostomy tray in crash cart) � Patient has cardiopulmonary arrest � Bleeding

� Document patient encounter and outcome �Nursing assessment of tracheostomy �Tracheostomy tube size �Tracheostomy suction �Tracheostomy patient education
. Tracheostomy. Retrieved from http: //mns. elsevierperformancemanager. com Adapted from Wiegand,")
Mosby’s Nursing Skills (2015). Tracheostomy. Retrieved from http: //mns. elsevierperformancemanager. com Adapted from Wiegand, D. L. (2011). AACN procedure manual for critical care (6 th ed. ). St. Louis: Saunders
- Slides: 70