BUTTS AND GUTS COMMON GASTROINTESTINAL GI ALTERATIONS IN
 ALTERATIONS IN OLDER ADULTS N 310 - Revised")
BUTTS AND GUTS: COMMON GASTROINTESTINAL (GI) ALTERATIONS IN OLDER ADULTS N 310 - Revised Fall 2016 Anne M. Devney, Ed. D. , R. N.

IT ALL STARTS WITH… NUTRITION Quality & quantity of diet – important factors in preventing, delaying onset & managing chronic illnesses – especially with aging. • Longevity + Lifestyle changes = reduced risk of disease • Lifetime of good nutrition –> improve 9/10 leading causes of death. . !

OBJECTIVES Describe age-related requirements Briefly review types of GI diagnostic studies Discuss definition, causes, s/sx, medical interventions & nursing management of several lower & upper GI alterations common in older adults: 1. Malnutrition - Overnutrition 2. Dysphagia 3. Gastroesophageal Reflux Disease (GERD) 4. Diverticulosis/Diverticulitis 5. Colorectal Cancer 6. Motility disturbances

Age-related requirements © Older adults generally need less calories ©Less muscle mass, less active, slower metabolic rates © Still need same or higher levels of nutrients ©Fats – 20 -35% total calories ©Protein – 20 -25% total cals, min. frailty ©Fiber – 25 Gms ©Vitamins & minerals – 5 servings = adequate A, C, E, K+, aging causes less absorption B 12 © Use My. Plate. gov for older adults

My. Plate for Older Adults

Diagnostic Studies related to GI Alterations
 passed through mouth or nose to visualize esophagus")
Upper GI Endoscopy Lighted tube (scope) passed through mouth or nose to visualize esophagus & stomach ©Moderate Sedation ©NPO 8 hours before & 2 hours after ©Monitor for return of gag reflex

Barium Swallow Referred to as an “Upper GI Series” esophagus, stomach, duodenum, jejunum ©NPO x 8 hours ©Drink 3 -4 cups of barium ©X-Ray ©Force fluids, laxative afterward, clay-colored stools

CT Scan of Abdomen Computerized tomography of abdomen ©Thin beam of X-Rays provides multiple image slices of body parts ©Patient lies on motorized table ©Some noise is noticed as equipment moves ©Patient must remain motionless ©Oral contrast administered beforehand ©Force fluids after to prevent renal impairment; may be given oral Mucomyst (free radical scavenger to remove contrast by-products) after ©No metal objects or jewelry

Barium enema -Referred to as “Lower GI series” -Liquid barium administered through enema to coat lining of the intestine & x-rays are then taken to visualize large intestine, colon, and rectum ©Bowel prep (e. g. Go-lytely; clear liquids) ©Stools clay & white colored ©Force fluids following procedure

Colonoscopy, Virtual Colonoscopy & Sigmoidoscopy © Essentially the same principle as an endoscopy except the scope is inserted through the anus to visualize the lower GI tract © Colonoscopy – examines mucosa of colon © Virtual colonoscopy – looks specifically for polyps, precancerous cells & cancer © Sigmoidoscopy – examines sigmoid colon © Bowel prep © Sedation © Will need someone to drive home after procedure

UPPER GI DISORDERS

1. MALNUTRITION

What is MALNUTRITION? Definition: disparity between the amount of food and nutrients that the body needs & the amount that the body is receiving Includes Chronic overnutrition = OBESITY Chronic undernutrition = MALNOURISHMENT

OBESITY

DID YOU KNOW THE UNITED STATES RANKS ____ MOST OBESE COUNTRY in English speaking countries? ? !!! >60% of adults are now overweight… Children, too…!

What is OBESITY? ©Defined as body weight exceeding ideal weight by 20% ©Body mass index of 27 or greater BMI=wt/ht 2 or wt(lb)/ht(in)2 x 703 ©Obesity is a major risk factor for malnutrition ©Associated with stereotypes

CAUSES ©Genetic ©Sedentary lifestyle ©No exercise due to decreased mobility ©Hereditary factors ©High calorie diet ©Hypothyroidism ©Decreased caloric need ©Social isolation ©Declining dentition

COMPLICATIONS ©CVD ©DM ©Dyslipidemia ©Malnutrition ©HTN ©Gallbladder disease ©Arthritis

MEDICAL MANAGEMENT: Surgical Interventions ©Bariatric Surgery ©Gastric Bypass ©Lap-Band

NURSING MANAGEMENT: Patient Teaching ©My. Plate. gov for older adults ©Increase activity ©i. e. armchair aerobics

NURSING DIAGNOSES ©Imbalanced nutrition: more than body requirements ©Imbalanced nutrition: less than body requirements ©Readiness for enhanced nutrition ©Risk for constipation

MALNOURISHMENT ©Definition: under-nutrition; insufficient quality & quantity of foods, vitamins, and/or minerals ©Potential & serious threat to the older adult

RISK FACTORS AND CAUSES © Risk factors ©Decreased taste and smell; altered smell ©Decreased mastication ©Slower peristalsis ©Decreased hunger contractions ©Decreased gastric acid secretions

RISK FACTORS & CAUSES ©Malabsorption ©Pain ©Nausea or anorexia as med side effects ©Altered mental status ©Socioeconomic factors ©Inadequate hydration

RISK FACTORS & CAUSES ©Alcohol abuse ©Loneliness ©Poor dentition ©Inability to prepare food ©Lack of transportation ©Special diets/restrictions

ASSESSMENT: Tools and Physical To identify nutritional at-risk patients © Mini Nutritional Assessment © Skin turgor © Weekly weights

Mini Nutritional Assessment form – p. 181 * Rising incidence in acute & long-term care & community * Institutionalized adults – high risk due to chronic disease & functional impairments * Increased risk of infection, decubitus ulcers, anemia, hip fractures, hypotension, impaired cognition, increased morbidity & mortality • Can be related to poor intake of nutrients or consequence of inflammation * Comprehensive screening/assessment critical!

ASSESSMENT: Signs & Symptoms § Weight Loss > 5% in past month § Weight Loss 10% in past 6 months § Weight 10% below or 20% above ideal weight § Dermatitis, hair loss, lethargy, fatigue

ASSESSMENT: Deficits and Diagnostics ©Nutrients most deficient § Iron § Vitamins A & C § Calcium § Lab Studies § Decreased serum albumin (3. 5 -4. 8 g/d. L or 35 -48 g/L § Decreased hemoglobin (F 12 -16/M 14 -17. 4) § Decreased hematocrit (F 36 -48/M 42 -52)

COMPLICATIONS ©DEATH ©Dehydration ©Weight loss ©↑ development of frailty ©↓ wound healing ©↑ risk for infection
 A lcoholism")
© Causes for weight loss-- Mnemonic MEALS-ON-WHEELS M edications E motions (depression) A lcoholism L ate life paranoia S wallowing problems O ral problems N osomial infections W andering (dementia) H yperthyroidism, hypercalcemia, hyperglycemia, hypoadrenalism E nteral problems (malabsorption) E ating problems (e. g. tremors) L ow salt, low cholesterol diet S tones (e. g. cholecystitis) (John, 2008)
")
NURSING MANAGEMENT: Interventions and Patient Teaching Meals on Wheels Congregate meals (Senior Citizen Centers) Consult with a registered dietician Offer largest meal at time when hungriest Offer favorite foods; sweet foods Short-term or long-term TPN
")
NURSING MANAGEMENT: Interventions ©Provide between meal snacks ©Provide supplements ©Boost, Ensure, Medpass (serve cold) ©Calorie and protein fortified puddings & jello ©Peanut butter sandwiches ©Coach the older adult while eating

NURSING DIAGNOSES ©Fluid volume deficit ©Altered nutrition: less than body requirements ©Risk for infection ©Knowledge deficit
 & CRP (C reactive protein:")
EVIDENCE-BASED PRACTICES ©Pre-albumin ( good indicator of protein status) & CRP (C reactive protein: a glycoprotein produced by the liver in severe inflammation) OR ©Pre-albumin vs. CRP(C reactive protein)

2. DYSPHAGIA

DYSPHAGIA? ? © Definition: difficulty swallowing solids or liquids © Most common GI disturbance in older adults.

CAUSES © Neurological disorders ©CVAs © Endocrine disorders ©Diabetes mellitus © Motility disorders © Muscular disorders ©Achalasia(absent or ineffective peristalsis of the ©Amyotrophic Lateral lower esophagus Sclerosis ©Diffuse esophageal spasm ©Myasthenia Gravis ©Parkinson’s disease © Anatomical abnormalities ©Strictures ©Tumors

ASSESSMENT: Signs & Symptoms ©Report from family of difficulty swallowing ©Difficulty in controlling food or saliva (drooling) ©Choking or coughing during meals ©Eating slowly ©Difficulty swallowing ©Weight loss ©Recurrent pneumonia ©Gurgling voice during or after eating ©Retention or pocketing of food

COMPLICATIONS © Aspiration pneumonia © Malnutrition © Medication-induced esophagitis

Medication-Induced Esophagitis ©“Pill Esophagitis” ©Common in the older adult ©Inflammation of the esophagus due to irritation from medications ©Hint: Dysphagia & Polypharmacy

NURSING MANAGEMENT: Interventions & Patient Teaching ©Add thickener to fluids ©Pureed foods ©Evaluation by speech & occupational therapist ©PEG feeding ©Teach “chin-tuck & swallow” technique ©Small bites

NURSING DIAGNOSES Actual Impaired Swallowing Feeding Self-care deficit Potential Altered Nutrition: Less than body requirements Risk for aspiration
")
3. GASTROESOPHAGEAL REFLUX DISEASE (GERD)

What is GERD? § Definition: common GI syndrome where there is backward flow of gastric contents into the esophagus due to inappropriate relaxation of the lower esophageal sphincter (LES) § In older adults, GERD is associated with weakening of the diaphragm, obesity & kyphosis

RISK FACTORS & CAUSES Risk Factors ©Alcohol ©Smoking ©Obesity ©High levels of progesterone & estrogen Causes ©Medications affecting sphincter pressure ©Caffeine ©Chocolate ©Pregnancy ©Achalasia ©Spicy & fatty foods ©Hiatal hernia
 & indigestion © Dyspepsia (what is this?")
ASSESSMENT: Signs/Symptoms © Heartburn (medical term: pyrosis) & indigestion © Dyspepsia (what is this? __________) © Hypersalivation © Chest pain mimicking angina or MI © Stomach acid regurgitation

COMPLICATIONS © Esophagitis © Esophageal Strictures © Dysphagia © Barrett’s esophagus - ____________ © Respiratory issues © Esophageal ulcers

CLINICAL PROGRESSION OF GERD *If left untreated or treatment fails… Incompetent LES (Lower Esophageal Sphincter) → Regurgitation → inflammation → esophageal erosion → ulcerations → bleeding → scar tissue and decreased ability to accommodate → metaplasia → Barrett’s esophagus → respiratory distress
 © Prevacid © Protonix © Nexium ©")
MEDICAL MANAGEMENT: Medications Proton Pump Inhibitors (PPIs) © Prevacid © Protonix © Nexium © Prilosec Antacids © Mylanta, Maalox © Gaviscon Acid Protective © Carafate H 2 blockers © Pepcid © Zantac © * NO Tagamet* Prokinetics © Reglan Cholinergics © Urecholine

MEDICAL MANAGEMENT: Surgical Interventions Diagnostics --Pill. Cam ESO capsule endoscopy (You swallow a small pill containing a video camera, which transmits images of your small intestine to a recording device. ) --Barium swallow --traditional endoscopy --Ambulatory acid (p. H monitoring) probe tests Surgical Repair 1. Laparoscopic Nissen Fundoplication or Toupet fundoplication 2. Endo. Cinch endoluminal gastroplication 3. Hill’s operation 4. Stretta procedure

NURSING MANAGEMENT: Patient Teaching Lifestyle modifications © Take medications & avoid ASA & NSAIDS © Smoking Cessation © Weight reduction © Elevate HOB 6 -8 inches to prevent nocturnal reflux

NURSING MANAGEMENT: Patient Teaching Nutritional modifications © Avoid foods that affect LES pressure © Avoid very hot, cold, spicy & fatty foods; chocolate; coffee; alcohol; acidic foods/drinks © Avoid nocturnal meals & lying down immediately after eating © Eat 4 -6 small meals per day © Drink adequate fluids with meals © Eat slowly & chew food thoroughly

EVIDENCE-BASED PRACTICES ©PPIs are most effective for reflux ©In acute care, PPIs & H 2 antagonist have been found to cause pneumonia in intubated patients

LOWER GI DISORDERS

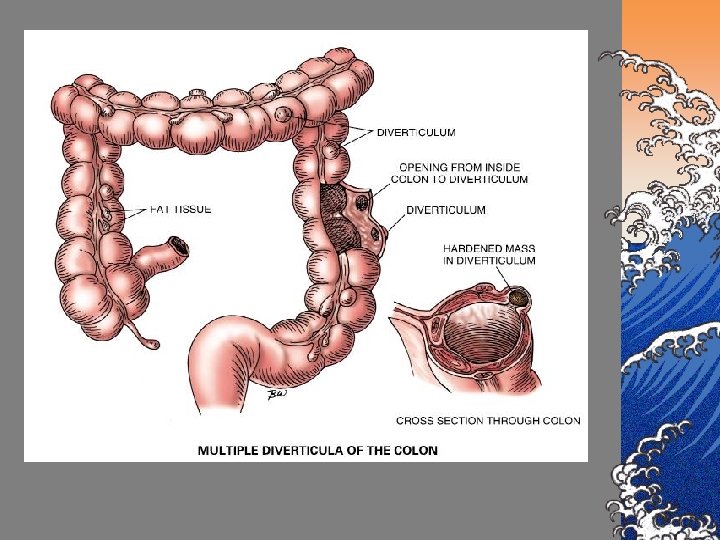
4. DIVERTICULOSIS/ DIVERTICULITIS

DIVERTICULOSIS ©Definition: structural weakening of colonic muscle especially left descending sigmoid colon that contribute to diverticula formation Diverticula: multiple sac-like out pouchings or herniations of the muscle layer of the intestinal mucosa

CAUSES ©Disturbances in motility ©Chronic constipation from low fiber, low fluid diet ©Neurologic disorders ©Mobility impairment ©Obesity ©Atrophy of intestinal muscle

ASSESSMENT: Signs & Symptoms © Frequently asymptomatic © Constipation © Bowel irregularity & diarrhea © Cramping pain in left lower quadrant © Low-grade fever © Nausea & anorexia © Bloating or abdominal distention © Slight bleeding © Palpable mass

COMPLICATIONS ©Diverticulitis ©Obstruction ©Perforation → GI bleeding ©Peritonitis ©Abdominal pain, a rigid boardlike abdomen, loss of bowel sounds, & S/Sx of shock ©Septicemia, if left untreated
 ©Computerized tomography (CT)")
ASSESSMENT: Diagnostics ©Pill. Cam SB capsule endoscopy (to visualize small intestine) ©Computerized tomography (CT) scan (procedure of choice) ©X-Ray Studies (barium enema) ©Colonoscopy ©Complete blood count (WBC & sedimentation rate are elevated)

NURSING MANAGEMENT: Interventions & Pt. Teaching ©Prevention ©Prevent constipation ©High fiber, low fat diet ©Good hydration ©Exercise… stress management

DIVERTICULITIS ©Inflammation & infection of diverticula due to trapped food residue, fecal matter, and/or bacteria

Excess fecal volume in colon from constipation lead to increased intraluminal pressure Weakening of colonic muscle wall Herniations or outpouchings of intestinal mucosa develop Entrapment of fecal matter, undigested food, and/or bacteria lead to infection & inflammation This can lead to scarring, further muscle wall weakening, abscess formation, perforation, hemorrhage & peritonitis

SIGNS & SYMPTOMS ©Signs & Symptoms ©Cramps, narrow stools, ^ constipation ©Occult bleeding ©Weakness, fatigue, anorexia ©Tenderness, a palpable mass, ^ WBC ( signs of abscess development)

MEDICAL MANAGEMENT: Interventions MILD TO MODERATE ©Clear liquids until inflammation subsides, then a high-fiber, low-fat diet ©Antibiotics for 7 -10 days ©A bulk-forming laxative

MEDICAL & NURSING MANAGEMENT: Interventions SEVERE CASES ©Rest the bowel through NPO ©IV fluids ©NG Suctioning ©Antibiotics & analgesics ©Increase oral intake as s/sx subside ©Low fiber diet until signs of infections decrease ©Antispasmodics for spastic pain ©Bulk laxatives, stool softeners ©Monitor for complications like perforation, peritonitis & fistulas
 © ciprofloxacin (Cipro)** © clarithromycin (Biaxin)")
MEDICAL MANAGEMENT: Pharmacotherapy © Antibiotics © metronidazole (Flagyl) © ciprofloxacin (Cipro)** © clarithromycin (Biaxin) © Analgesics © hydromorphone (Dilaudid) © Morphine © Anticholinergics © Atropine © Antispasmodics © Many antispasmodics are contraindicated on BEERs criteria & some cannot be used jointly with antibiotics

MEDICAL MANAGEMENT: Surgery ©If medical management is unsuccessful, perforation, peritonitis, abscess formation or obstruction occurs ©Colon (bowel) resection with anastomosis ©Temporary or permanent colostomy (see packet for care of colostomies)

NURSING MANAGEMENT: Interventions & Patient Teaching © Auscultation of bowel sounds to assess for perforation © Avoid indigestible roughage or gas inducing foods like seeds, nuts, corn, popcorn © Avoid activities that increase abdominal pressure (i. e. valsalva maneuver, lifting, or bending) © Consume a small amount of bran daily to increase stool mass

5. COLORECTAL CANCER

Colorectal cancer is the 3 rd leading cause of cancer in the WORLD!!!

Colon & Rectal Cancer = Colorectal cancer ©Definition: malignancy of the colon & rectum © 95% adenocarcinoma ©Incidence of colon cancer twice that of rectal cancer

RISK FACTORS ©Age > 85 ©Family history ©History of inflammatory bowel disease ©Diet high in fat, protein, beef & low fiber ©Hx of Polyps

DIAGNOSIS ↔ PROGNOSIS © 3 out of 4 patients could be saved by early diagnosis & prompt treatment ©Low 5 year survival rate due to late diagnosis

ASSESSMENT: Signs & Symptoms © Many patients are asymptomatic for long periods of time & do not seek medical help © Presenting Symptom: changes in bowel habits or appearance © 2 nd most common symptom: passage of blood in the stools © Unexplained anemia, anorexia, wt. loss & fatigue © Jaundice © Epigastric pain
")
ASSESSMENT: Signs & Symptoms ©R sided lesions…dull abdominal pain & black, tarry stools (melena) ©L sided lesions…associated with obstruction (abdominal pain & cramping, narrowing stools, constipation, distension & bright red blood in the stools

ASSESSEMENT: Signs & Symptoms ©Rectal lesions…ineffective painful straining at stool, rectal pain, feeling of incomplete evacuation after a bowel movement, alternating constipation & diarrhea & bloody stool ©Signs of complications ©Bowel obstruction, tumor extension into surrounding blood vessels>>>sepsis
 © Fecal occult blood testing ©")
MEDICAL MANAGEMENT: DIAGNOSTICS © Digital rectal exam (DRE) © Fecal occult blood testing © Air contrast barium enema © Proctosigmoidoscopy © Colonoscopy

DIAGNOSIS: Colorectal Ca ©If cancer is dx, the older adult will need: ©CT of abdomen & pelvis ©Chest radiograph ©Routine blood work ©Carcinoembryonic (CEA) level

MEDICAL MANAGEMENT: Surgery ©Surgery: primary treatment ©depends on location & size of tumor ©YAG laser effective in some lesions ©Partial Colectomy or Hemicolectomy - Bowel resection with anastomosis with possible temporary or permanent colostomy
 ©Full liquid diet 24 -48 hours preop ©Parenteral nutrition")
NURSING MANAGEMENT: Interventions Pre-op (EBP) ©Full liquid diet 24 -48 hours preop ©Parenteral nutrition if prescribed ©Antibiotics, laxatives, enemas or colonic irrigations as ordered ©Nasogastric tube ©Intravenous management ©I&O

NURSING MANAGEMENT: Interventions and Pt. Teaching Pre-op ©Monitor for S&Sx of obstruction or perforation ©^ abd distension, high-pitched or loss of bowel sounds, pain, rigidity ©Patient teaching…ostomy ©Provide emotional support/support body image ©Nurs dx: Disturbed body image

NURSING MANAGEMENT: Post-op & Patient Teaching © Examine wound dressing frequently during first 24 hours checking for infection, dehiscence, hemorrhage & excessive edema © VS © IV therapy © Bowel sounds © PAIN? ? © Discharge teaching

EVIDENCE-BASED PRACTICES ©See slide 83 – surgery, etc. ©Chemo after surgery is recommended to reduce recurrence

6. MOTILITY DISTURBANCES Includes -Constipation Diarrhea Fecal Incontinence

CONSTIPATION “ I have to have a bowel movement everyday. ” – Anonymous Older Adult

CONSTIPATION ©Decrease in frequency of bms from the individual “normal” ©Normal frequency for any age is 3 x/day to 3 x/week? ? ? ©Painful defecation of hardened stools

CAUSES © Not enough water AND fiber © Immobility © med side effects © Obesity © enlarged prostate gland © delayed defecation (encopresis) ©Safe toilet syndrome © stress © Hypothyroidism © hypercalcemia © Chronic laxative use ©Cathartic colon syndrome

ASSESSMENT: Signs & Symptoms ©Abd distention ©Abd pain ©Increased flatulence ©Nausea ©Headache ©Anorexia ©Tenesmus - ___________ ©Stool with blood ©Depression

COMPLICATIONS ©Hemorrhoids ©Anal fissures ©Rectal prolapse ©Mega colon ©Fecal impaction ©Overflow fecal incontinence ©Valsalva maneuver complications

Nursing Management: Interventions & Pt. Teaching ©Force fluids ©Prune juice; Hot coffee or tea ©Leg exercises, ambulation ©Increase fiber (bran, fruits, broccoli…) ©Laxatives, suppositories, enemas ©Digital removal or fecal impaction ©Appropriate laxative use ©NO MINERAL OIL!! ©Bowel training program

EVIDENCE-BASED PRACTICES © Daily Bowel training program: purpose is to overcome inhibition of gastrocolic reflex; a behavioral training ©Encourage to have a BM immediately after first meal of the day (breakfast most likely) ©No bm immediately after bkfst, give an enema. ©Keep a log or chart of bms (#, consistency, time) ©Training is usually successful by 3 rd to 5 th day without rectal stimulation ©Can be done in cognitively impaired elderly as well (Cassel, 2006; Eliopoulos)

NURSING DIAGNOSIS ©Chronic constipation ©Impaired bowel elimination ©Pain In paralyzed older adult ©Risk for autonomic dysreflexia

DIARRHEA Definition: frequent passage of difficulty to control loose, watery stools Acute or Chronic

CAUSES © Food intolerances © food poisoning © lactose intolerance © Alcohol © High volume, continuous tube feedings © Medication SE; Long term antibiotic use & excessive laxative use © Bowel Disorders © Crohn’s Disease © Irritable Bowel Syndrome (IBS) © Intestinal Obstruction (fecal impaction) © HIV/AIDS; Bacterial Infections (e. g. C. Difficile; salmonella; E. Coli; giardia ) © Stress & Emotions

ASSESSMENT: Signs And Symptoms ©Cramping ©Fever-- sudden or slow onset ©Green or yellow stools, mucous or blood in stool ©Frequent and “runny” stools ©Bloating

NURSING MANAGEMENT: Interventions & Pt. Teaching § Treatment § D/C Meds § Use bulking agents (bran; Metamucil) § Avoid foods which cause diarrhea (lactose) § Bowel sounds; observe for peristaltic movements § Antidiarrheals – caution with these b/c you want the body to rid itself of any infectious agent § Potential emergency>>>>fluid and electrolyte imbalance § Hydration (IV or oral- Gatorade or Pedialyte)

FECAL INCONTINENCE ©Definition: Inability to retain a BM or know when one occurs; involuntary defecation ©Major reason for institutionalization ©Causes ©Tumors ©Neurological ©Mental status

CAUSES ©Fecal impaction ©Tumors ©Neurological impairment ©Mental status impairment ©Reduced reservoir capacity

NURSING MANAGEMENT: Interventions ©High fiber diet ©Respond timely to toileting request ©Remove fecal impaction (if applicable) ©Bowel Training
 Deficient fluid volume")
NURSING DIAGNOSES ©Diarrhea ©Impaired skin integrity ©Disturbed body image ©(Risk for) Deficient fluid volume ©Pain ©Impaired social interaction

© Your 83 -yr old patient has a poor appetite and distended abdomen. She complains of abdominal discomfort and small amounts of diarrhea. You notice fecal matter on her gown. Your best action is to consult with the physician regarding the need for: a. An anti-diarrheal medication b. A digital rectal examination c. Lower GI studies d. Stool cultures
- Slides: 105