BURNS PATHOPHYSIOLOGY LIZ AUGUSTINE 2002 BATCH INTRODUCTION n

BURNS PATHOPHYSIOLOGY LIZ AUGUSTINE 2002 BATCH

INTRODUCTION n COAGULATION NECROSIS OF SKIN AND UNDERLYING TISSUES n DELITERIOUS EFFECTS ON ALL ORGAN SYSTEMS n ORGAN DYSFUNTION PROPORTIONAL TO EXTENT OF BURNS

TYPES § § § Thermal Chemical Electrical Ionising Radiation Cold Injuries

GENERAL FEATURS n A central coagulation area due to the direct action of the burn agent. This causes an immediate protein destruction- Necrosis (pathological death, destruction of cell elements of the connective tissues, tissue necrosis). n A peripheral, stasis area, where the damage caused by thermal energy is less- Ischaemia (stasis and microthrombosis).

n. A third area, external to the others, characterized by hyperaemia where heat action is less. The three concentric areas exist in thickness too, and thus determine the depth of the damage.

TISSUE CHANGES

ZONES OF BURN INJURY
 due to")
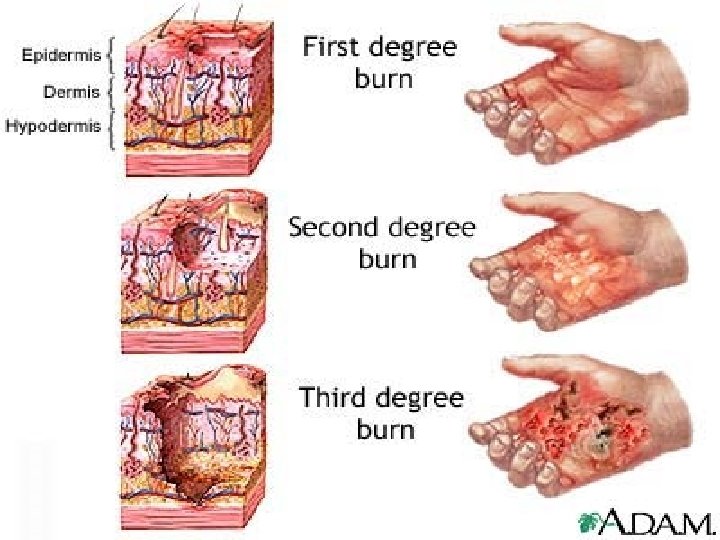
Clinical aspects Degrees of burns n First-degree burns n Simple erythema (redness) due to hyperaemia, arteriolar and capillary dilatation of the dermis. Histologically, it is characterized by a delamination of the stratum corneum, dermal oedema and vessel dilatation. n First-degree burns heal spontaneously after 3 to 6 days without any sequelae. Healing may be followed by a short period of hyperkeratosis and hypermelanosis.

FIRST DEGREE BURNS

n Second degree burns. These burns are characterized by the presence of blisters on a uniformly bright red, moist base. They are the expression of the damage caused to cell elements of the prickle cell layer and the papillary layer with dermo-epidermic detachment and accumulation of transudate from injured capillaries.

n The blisters present a tectum consisting of the epidermis, a uniformly red floor composed of dermal papillae, without epithelium or with some residual degenerated basal cells, and a content composed of plasmatic exudate. Skin adnexae are maintained and sensitivity is increased.

n In superficial second-degree burns healing occurs within 10 - 15 days by spontaneous re-epithelialization of hair adnexae, sebaceous and sweat glands.
![SUPERFICIAL 2 ND DEGREE BURNS [superficial partial thickness burns]](http://slidetodoc.com/presentation_image/15367c0cc2865df94dfd60c7da4d0a12/image-13.jpg "SUPERFICIAL 2 ND DEGREE BURNS [superficial partial thickness burns]")
SUPERFICIAL 2 ND DEGREE BURNS [superficial partial thickness burns]

n Deep second-degree burns n These are characterized by an irregular surface (whitish with minute petechiae), which is the expression of a deeper lesion affecting the papillary layer and much of the reticular layer. The dermal surface is speckled with whitish dots corresponding to areas where dermal papillae are destroyed. The cutis and subcutis present clearly visible oedema
, with formation of")
n takes a longer time to heal (16 - 25 days), with formation of scar tissue. Surgical procedures are often necessary in order to accelerate and improve the healing process and prevent scarring.
![DEEP 2 ND DEGREE BURNS [deep partial thickness burns]](http://slidetodoc.com/presentation_image/15367c0cc2865df94dfd60c7da4d0a12/image-16.jpg "DEEP 2 ND DEGREE BURNS [deep partial thickness burns]")
DEEP 2 ND DEGREE BURNS [deep partial thickness burns]

n THIRD DEGREE BURNS - are full-thickness burns. The appearance of the lesion depends on the burn agent: in flame burns the injured area is dark brown or black, with visible thrombosed vessels; it is yellow-brown and de-epithelialized, with a translucid appearance when fire is the burn agent; and it is ice-white or greyish when caused by hot liquids. Necrosis of the epidermis, dermis and hypodermis, at various levels, is always associated with vascular damage (the vessels may even be totally occluded).
![THIRD DEGREE BURNS [full thickness burns]](http://slidetodoc.com/presentation_image/15367c0cc2865df94dfd60c7da4d0a12/image-18.jpg "THIRD DEGREE BURNS [full thickness burns]")
THIRD DEGREE BURNS [full thickness burns]

n The epidermis and dermis are affected by phenomena of massive necrosis. The epidermal layer is uniformly pale and is coagulated into a single mass with the dermis, forming a whitish or dark, dry, cool thick skin. The lesion may involve tissues as profound as the bone. Superficial and deep dermal vessels are thrombosed. The leucocytic reaction is intense and spreads under the area covered by the eschar. All fibres are destroyed.

n Spontaneous healing in third degree burns is due to two processes: n Regeneration: epithelial cells at the margin of the lesion proliferate centripetally, and slowly bring about healing. In the connective and endothelial structures, there are tumultuous proliferation phenomena which cause the formation of excessive granulation tissue.

n Contraction: this reduces the extent of the burn lesion. It depends on forces linked with the contraction of myofibroblasts. Thus the margins of the lesion begin to come closer to the centre of the injury. n Spontaneous healing is thus a slow process, with gradual remodelling of the scar, which due to contraction phenomena may lead to serious deformity. It is therefore necessary to intervene with well planned surgical procedures

BIOCHEMICAL AND MICROCIRCULATORY ASPECTS n Inflamn originates in areas with circulation n Cell damage consists of: 1. Mitochondrial lesions 2. Lysosomal lesions 3. Release of enzymes 4. Lesions of ER 5. Lesions of cell membranes

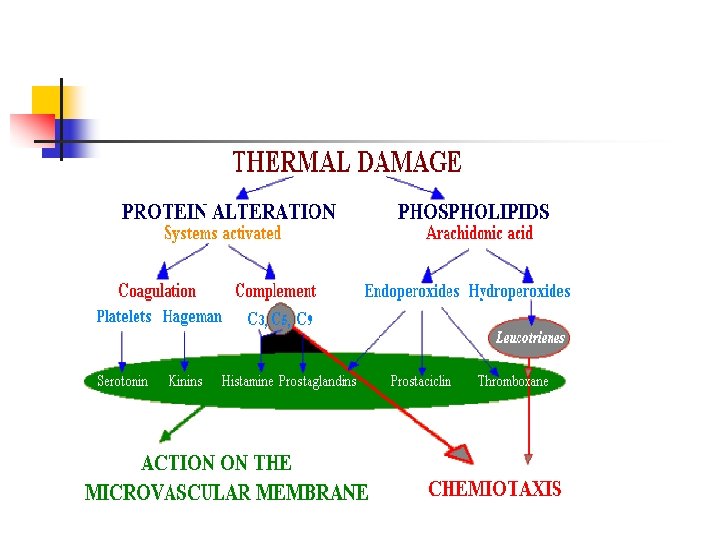
Capillary permeability increase by 2 phases: 1 st phase: Thermal damage Protein alteration Activation of coagulatn & complement n Kinin&serotonin C 3, C 5, mast cell degranulation histamine release vasodialatation

2 nd phase: Chemotactic factors- activatn of arachidonic acid cascade Adhesion of leucocytes to endothelium Their migration to interstitium Release of O 2 free radicals Further activatn of oxidatn of arachidonic acid Formn of LTB 4 , LTC 4 , LTD 4 Chemotactic activity , increase vascular permeability

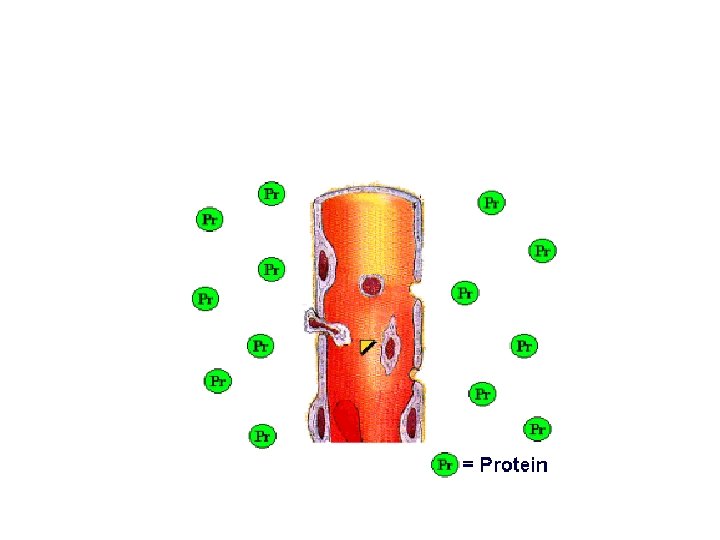
Endothelial Alterations n n n n In endothelial cytoplasm vacuoles increase Wide gaps in endothelium Permeability to macromolecules Decrease Na-Ka pump activity in endothelial cells Increased Na & water uptake into cells Cells swell End gaps are seen in post-capillary venules

Local oedema formation n While burning - transitory decrease in blood flow - marked arteriolar dialatation -oedema Extent of oedema depends on extent of blood flow in damaged tissues Oedema formn in small burns reaches max within 6 hrs of trauma In extensive burns it takes about 18 -24 hrs

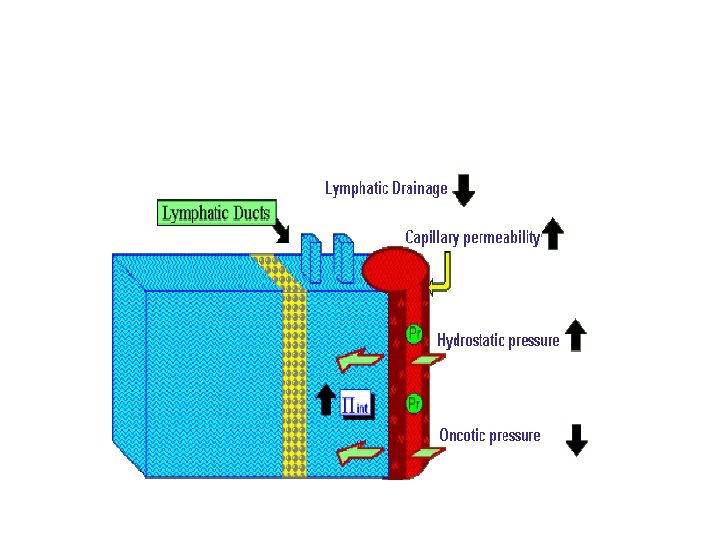
4 processes involved in oedema formn: n Increased capillary hydrostatic pressure n Decrease in plasma oncotic pressure , Increase in interstitial oncotic pressure n Increase in permeability of capillary wall n Decrease in lymphatic drainage Oedema decreases O 2 supply to cells-increases their damage If burn surface >30% TBSA –oedema spreads to unburned tissues n

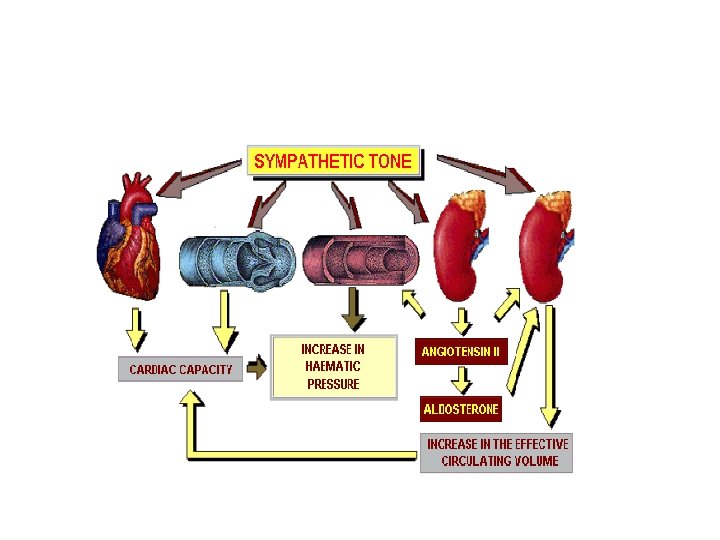
Early shock phase n Leakage of fluid from intra to extra vascular space n Decrease circulatory volume n Increase free water deficit n Compensatory hemodynamic changes n Decrease venous return n Decrease cardiac output n Decrease in mean arterial BP

n Stimulatn of barorecepters in carotid sinus and aortic arch n Decrease in arterial BP n Increased sympathetic activity n Tries to return BP to normal by direct action on heart n Increase myocardial contractility & HR n Increase circulatory volume

n Increase circulatory volume n Increase renal absorbn of water &Na n Increase vascular resistance n Increase VP Vasoconstriction in cutaneous & mesenteric circulation

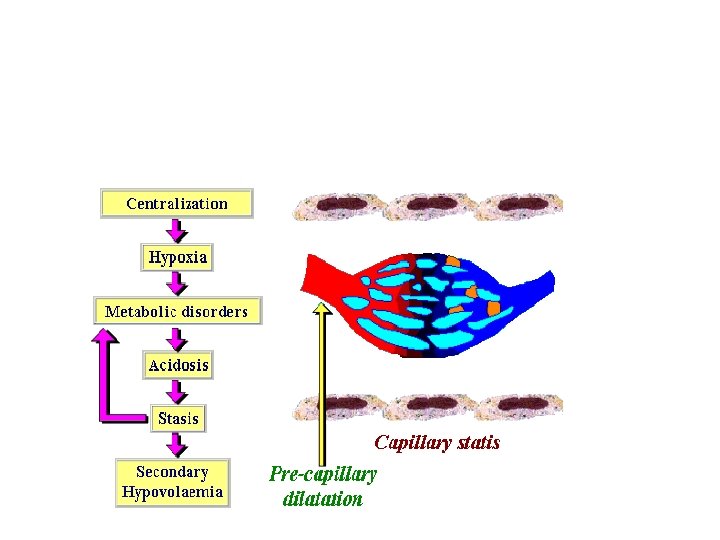
Clinical shock syndrome n Burn size >15% TBSA produce circulatory shock n Persistent vasoconstriction – hypoxia –a vicious cycle which aggravates shock n Hypoxia -increase local& systemic metabolic acidosis n Functional & organic damage n These occur when no treatment is taken

n Acidosis -decrease vascular tone in arterial part –capillary stasis –as postcapillary sphincter constricted –blood accumulates in capillary lumen –secondary hypovolemia

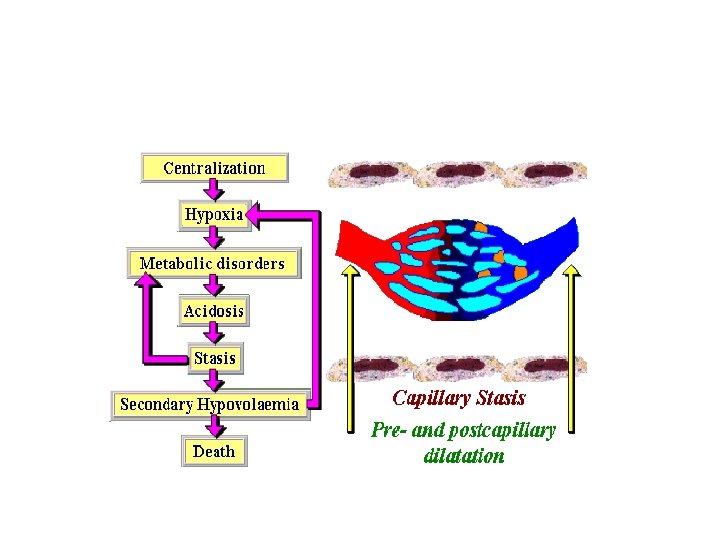
Late shock phase n Phase of vasoparalysis n increase dilatation in post capillary system n fluid resuscitation wont improve tissue perfusion n Collapse of entire circulation n death

Changes in other systems: respiratory system n n Inflammatory mediators cause bronchoconstriction, and in severe burns adult respiratory distress syndrome can occur. In circumferential burns of thorax- eschar and underlying oedema restrict ventilation Initial hypovolemia-rapid shallow respiration After resuscitation-hyperventilation –mild respiratory alkalosis


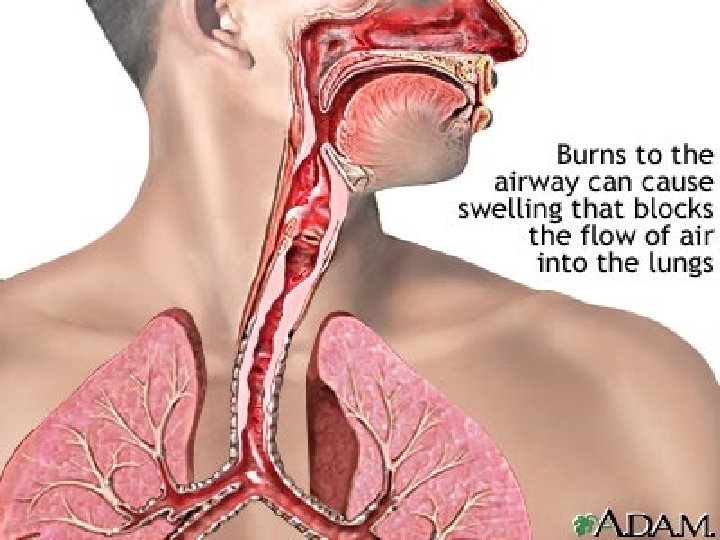
n n n INHALATIONAL INJURY: Upper airway Thermal / chemical injury leading to edema Lower airway Thermal injury unlikely beyond major bronchi [except steam ] Injury secondary to inhalation of chemically injurious substances [ HCl, SO 2, NH 3] pneumonitis and / or pulmonary edema

n Systemic toxicity n In civilian setting only CO or occasionally cyanide CO binds 240 times as strongly as O 2 to Hb Cyanide is a metabolic poison at mitochondrial level

n HEMATOLOGIC CHANGES: -Loss of plasma -RBC destruction -biphasic alteration of coagulation system

Changes in other systems n Metabolic changes-The basal metabolic rate increases up to three times its original rate. This, coupled with splanchnic hypoperfusion, necessitates early and aggressive enteral feeding to decrease catabolism and maintain gut integrity. n Immunological changes-Non-specific down regulation of the immune response occurs, affecting both cell mediated and humoral pathways

GIT Changes n Ileus in patients with burns>25% TBSA n Gastric & duodenal mucosal damage n Sometimes frank ulcerations n Gastroduodenal Stress ulcers – Curling’s ulcer

GIT Changes n Scarring n Perforation Failure of enteral feeding in extensive burns Translocation of gut bacteria – main source of infection Abdominal compartment syndrome – due to gut mucosal swelling

Endocrine changes n Glucagon , cortisol , catecholamines increase n Insulin & triiodothyronine decrease

complications n n n n n Early Hypovolemia Fluid overload Renal dysfunction Hemoglobinuria Stress gastroduodenal ulcers Pulmonary dysfunction Burn encephalopathy Local / systemic sepsis

n Late sequelae n Scarring –hypertrophic, keloid n Contractures – limbs, neck n Hypo / hyperpigmentation n Disfigurement n Functional disability n Post-traumatic stress

n Features associated with inhalational burns – History of fire in an enclosed space – History of unconsciousness – Cough + / - bronchorrhea – Sooty sputum – Facial burns – Singed nasal hairs – Auscultatory signs in the chest

n Features of respiratory failure – Inability to speak due to dyspnoea – Sweating – Apparent exhaustion - Tachycardia - Tachypnoea[RR>40/min in adults] - PCO 2>5. 5 k. Pa - PO 2 < 8 k. Pa despite O 2 therapy

THANK YOU
- Slides: 55