BURNS Dr Neil DSouza Overview Epidemiology Definition Assessment

BURNS Dr. Neil D’Souza

Overview • • Epidemiology Definition Assessment Management • Immediate • Definite • Complications • Special considerations

Epidemiology • More then 6 million people are burned in India every year • Most are minor burns and treated in outpatient • About 5% require hospitalization for appropriate treatment

• Death in burns is a typical bimodal distribution • Immediately after injury • Weeks later as a result of multi-organ failure • 2/3 rd of burns occur at home involving children less then 15 yrs or elderly more than 60 yrs

Definition of a Burn “Tissue injury caused by thermal, radiation, chemical, or electrical contact resulting in protein denaturation, burn wound edema, and loss of intravascular fluid volume due to increased vascular permeability. ”

Approach to a Patient with Burns • Cause of the burns • Assessment of burn • Depth • Extent • Immediate casualty treatment

• Definitive treatment • • • Fluid resuscitation Nutrition Treatment of wound Infection Surgical intervention • Prevention of complications and their treatment

Types of Burns • Thermal burns • Scald • Flame • Flash • Contact • Electrical burns • Chemical burns • Cold injury • Radiation

• Effects of burns influenced by • Intensity • Duration of exposure • Type of tissue

Classification of burns • Depending on thickness of skin involved • Depending on percentage of burns

• Depending on thickness of skin involved

Classification • First degree • Second degree • Third degree • Fourth degree
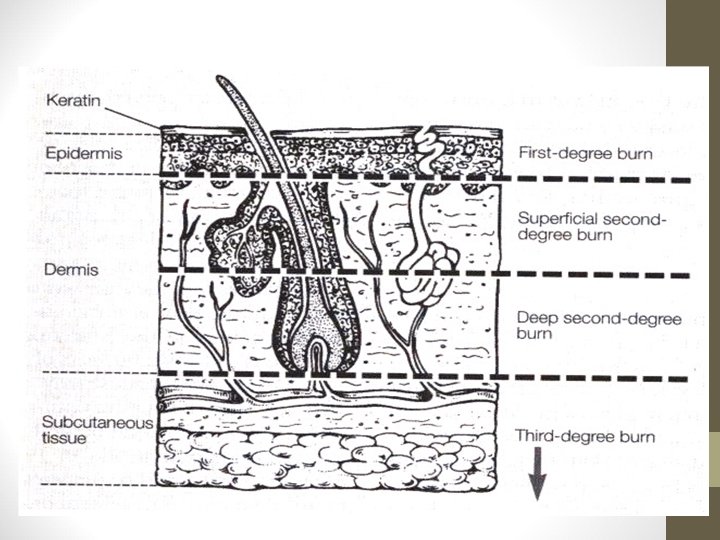

First-Degree Burns • Does not go below basal layer of the epidermis • Dry and painful • Appears red due to increased blood flow • Heals in a few days


Second-Degree Burns • Extends below basal layer, but not completely through dermis • Superficial • Blister, very painful, contains skin parts (adnexa) which assist in epithelialization • Deep Partial-thickness • Deeper in dermis, fewer adnexa, longer healing time, less painful



Third-Degree Burns • Extends completely through dermis • Adnexa destroyed so can’t heal by epithelialization • Dermal plexus of nerves destroyed-less painful • Burns can be yellow, red, black, brown


Fourth-degree burns • Full-thickness destruction of skin/subcutaneous tissue • Involves underlying fascia, muscle, bone or other structures • Prolonged disability

• Depending on percentage of burns

• Mild • Partial thickness < 15% in adult or <10% in children • Full thickness < 2% • Treated as outpatient

• Moderate – Partial thickness 15 -20% – Full thickness 2 -10% • Severe – – Partial thickness > 25% Full thickness > 10% Involving eyes, ears, feet, hands, perineum Burns with trauma

Zones of Burn Injury • Zone of Coagulation • Inner Zone • Area of cellular death (necrosis) • Zone of Stasis • Area surrounding zone of coagulation • Cellular injury: decreased blood flow & inflammation • Potentially salvable; susceptible to additional injury • Zone of Hyperemia • Peripheral area of burn • Area of least cellular injury & increased blood flow • Complete recovery of this tissue likely.

ASSESSMENT OF BURNS Rule of Nines

Burn Assessment Lund & Browder Chart

• Indications for admission – – – Moderate or severe burns (2 nd or 3 rd degree) Airway burns Burns in extremes of age Electrical or deep chemical burns Burns with significant co-morbid conditions Burns in pts who require special emotional, social intervention

Presentation • • H/o Burn Pain Anxious state Blisters Tachycardia Tachypnea In severe cases, shock

Pathophysiology

Fluid shift • § Vessels adjacent to burn injury dilate → ↑ capillary hydrostatic pressure and ↑ capillary permeability Continuous leak of plasma from intravascular space into interstitial space § Associated imbalances of fluids, electrolytes and acid-base occur § Hemoconcentration § Lasts 24 -36 hours

• After 36 hrs, fluid leak ceases • Fluid shifts back into circulation • Restores fluid balance and renal perfusion

• Inflammatory reaction is localised in small burns • After 10 -15% TBSA burns, inflammatory reaction (fluid loss) can lead to shock • Volume of fluid lost is directly proportional to area of the burn

Effects of burns • • Shock Renal failure Respiratory distress Infections Erosive gastritis Electrolyte imbalance Immunosuppression
 • Resuscitation (hours 0 -48) •")
Phases of Burn Care • Emergency care (ABCs) • Resuscitation (hours 0 -48) • Definitive care (day 3 until wounds are closed) • Rehabilitation

First Aid • Keep the patient away from the source • Clothing to be removed • Clean the part • Cool the area with tap water • Cover the part
 A = Airway (with cervical")
ABCs of Emergency Burn Care (Advanced Burn Life Support) A = Airway (with cervical spine assessment) B = Breathing C = Circulation D = Disability E = Exposure and Environmental Control F = Fluid Resuscitation based on Burn Size and Weight Measurement • Secondary Survey • • •

Definitive Treatment • Fluid resuscitation • Local management

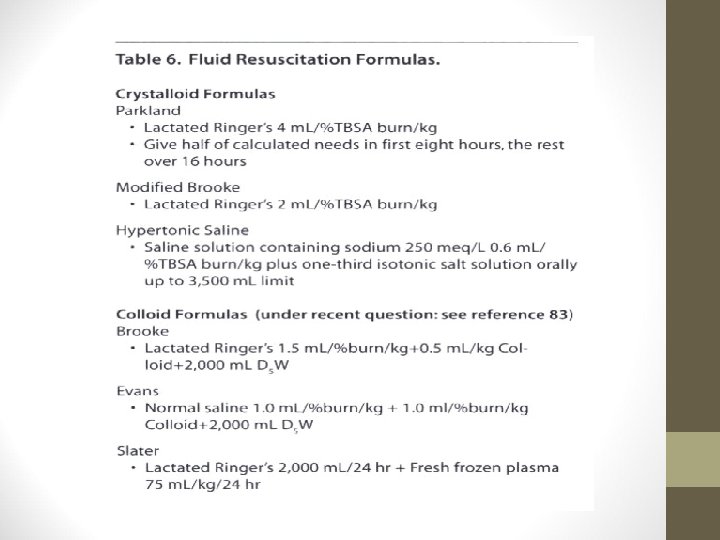
Fluid Resuscitation • 1 or 2 large bore IV lines • Fluid replacement based on: size/depth of burn, age of pt. • Palmar Method • Rule of Nines • Lund-Browder Method • Formula’s for replacement: Parkland formula and Brooke formula

Nutrition • Burns patients need more calories • Early enteral feeding in pts > 20 TBSA burns

Local management • 1 st degree burns • Regular dressings is mainstay • Topical ointments like neosporin , povidone iodine will suffice

2 nd degree burns • Regular dressings with antibiotic ointments • Silver sulfadiazine • Mafenide acetate • Silver nitrate • Or temporary coverage using biological/artifical synthetic coverings • If 2 nd degree burns don’t heal within 2 weeks, skin grafting is indicated
 • Isograft •")
Biological/artifical coverings • Biological • Autograft • Homograft • Heterograft (xenograft) • Isograft • Amniotic membrane • Cultured skin

• Artificial skin • Two layered which creates an artificial dermis • Synthetic dressing • Solid silicone and plastic dressing • Can see through to monitor wound status
 • 3 rd")
Collagen dressing • Indications • Deep 2 nd degree (non infected) • 3 rd degree burns as temporary covering after surgery • Advantages • Adheres to raw surfaces • Peels off as wound heals and epithelisation occurs • Promotes healthy granulation tissue in deep wounds


Artificial skin • Complex of collagen and condroiton sulphuric acid with silicon membrane

Systemic antibiotic therapy • Usually not recomended in the first 48 hrs • After 48 hrs, broad spectrum antibiotics started • Re-evaluation with C&S should be done every 5 days • Resistance and superinfection is common
 • Early excision")
Deep burns ( deep 2 nd degree and 3 rd degree) • Early excision • Tangential • Sequential • Followed by • SSG • Full thickness graft

EXCISION • Done in any burns that does not heal within 3 weeks • Specifically indicated in deep 2 nd degree and 3 rd degree burns • Done in 2 nd -5 th post burn day

Tangential excision • Done in deep dermal burns • Dead dermis is removed layer by layer until fresh bleeding occurs • Later skin grafting is done
 • Done in 2 nd and 3 rd")
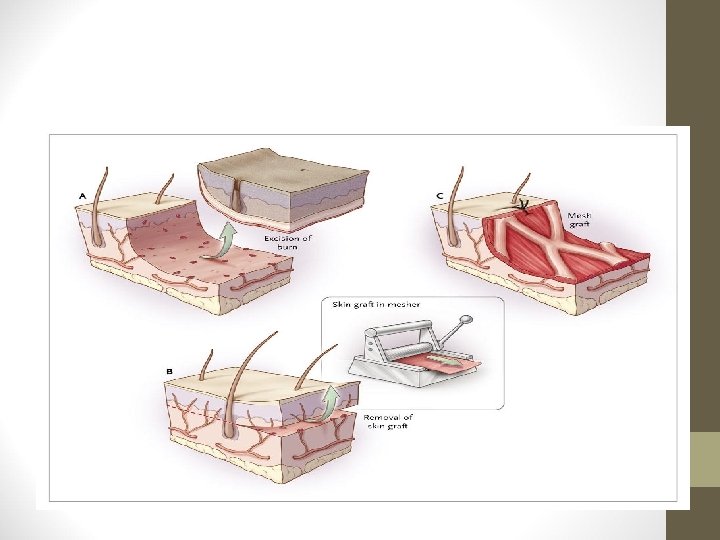
GRAFTING • Split thickness graft (SSG) • Done in 2 nd and 3 rd degree burns • Meshed graft used for large surface area • Thicker SSG more cosmetically accepted • Full thickness grafts • Used in small areas of cosmetic importance like face, hands


Eschar • Eschar- charred, denatured, full thickness, deep burns with contracted dermis • Insensitive, with thrombosed superficial veins • Can cause venous compression, arterial compression leading to ischaemia and gangrene

Escharectomy • Done usually in 2 -5 th post burn day or 3 rd post burn week • Non viable tissue removed with little pain • Grafting done at a later date

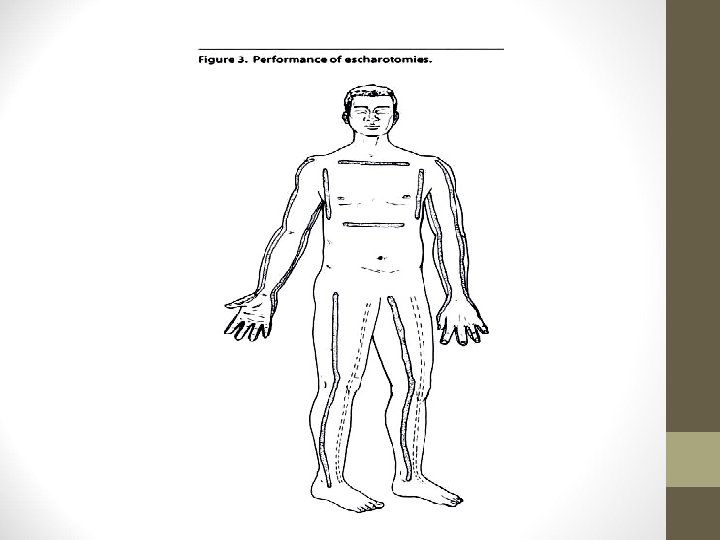
Escharotomy • Cut the burned skin to relieve the underlying pressure • Cut along the inside or outside of the limb • Knife or cautery is used

• Indications • Circulation of the limb is in danger due to swelling • Progressive loss of sensation/ motion • Progressive loss of pulses by palpation or doppler • In circumferential chest burns, patient might not be able to expand the chest and thus might need escharotomy


SPECIAL CONSIDERATIONS

ELECTRICAL BURNS • Extent of injury depends upon • • Type of current Amount of current Path of current Duration of current • Injury from electrical burns results from coagulation necrosis that is caused by intense heat generated from an electric current

Electrical injury can cause • Fractures of long bones and vertebra • Cardiac arrest or arrhythmias--can be delayed 24 -48 hours after injury • Severe metabolic acidosis--can develop in minutes • Massive muscle damage --- myoglobinuria --- mechanical block to renal tubules --- acute renal tubular necrosis

• Cardiac arrhythmias are the most serious immediate injury that occurs with electrical contact • V-Fib • V-Tach

ELECTRICAL BURNS
")
Treatment of electrical burns • Fluids- RL or other fluids • Osmotic diuretic (Mannitol) • To maintain urine output • Local management

CHEMICAL BURNS • Acids - can be neutralized • Alkalis - adhere to tissue, causing protein hydrolysis and liquefaction • Inorganic compounds • Organic compounds

• Acids • Immediate coagulation necrosis creating an eschar though self-limiting injury • Coagulation of protein results in necrosis • Affected tissues are converted into a dry, dull, homogeneous eosinophilic mass without nuclei
 • Liquefactive necrosis with continued penetration into deeper tissue resulting")
• Bases (Alkali) • Liquefactive necrosis with continued penetration into deeper tissue resulting in extensive injury • Characterized by dull, opaque, partly or completely fluid remains of tissue

CHEMICAL BURN COURTESY ROY ALSON, M. D.

• Injure the skin • May be absorbed into the body and damage internal organs • May be inhaled into the lungs and cause lung tissue damage • May have minimal skin injury and yet cause severe systemic injury

FACTORS CAUSING TISSUE DAMAGE IN CHEMICAL BURNS • Type of chemical • Concentration of chemical • Amount of chemical • Duration of contact • Manner of contact • Mechanism of action ACID BURN

TREATMENT OF CHEMICAL EXPOSURE • Remove all contaminated clothing • Brush off dry chemical • Flush with copious amounts of water or any drinkable liquid • Wipe or scrape any retained chemical and irrigate again

INHALATION INJURIES • Carbon monoxide poisoning • Toxic gas inhalation • Smoke inhalation • Heat inhalation • Steam inhalation • Asphyxiation

Inhalation injuries • Carbon monoxide poisoning • CO poisoning and asphyxiation account for majority of deaths • Treatment • • • Ventilator support for several weeks Hyperbaric oxygen Antibiotics Bronchoscopy, at regular intervals to remove bronchial casts Tracheostomy whenever required

• Inhalation injury above the glottis • Caused by inhaling hot air, steam, or smoke - thermally produced • Mechanical obstruction can occur quickly • Watch for facial burns, signed nasal hair, hoarseness, painful swallowing, and darkened oral or nasal membranes

• Inhalation injury below glottis • Below glottis-it is usually chemically produced. • Amount of damage is related to length of exposure to smoke or toxic fumes • Can appear 12 -24 hours after burn

Features of upper airway burns • Burns of the face • Singed eyebrows or nasal hairs • Burns in the mouth • Sooty sputum • History of being burned while confined to an enclosed space COURTESY ROY ALSON, M. D. LIP BURNS & SOOT IN MOUTH

Management • Airway, Oxygenation and Ventilation • Assess for airway edema early and often • Early intubation • When in doubt, oxygenate and ventilate • High flow oxygen • Bronchodilators may be considered if bronchospasm present

• Circulation • Treat shock • IV Access • Large bore, multiple IV cannulas • RL/NS • Titrate fluids to maintain systolic BP and perfusion

CHRONIC PROBLEMS • Post- burns contracture • Wound shortening • Can be intrinsic by loss of tissue or extrinsic by pull during healing phase • Hypertrophic scar • Seen in 2 nd and 3 rd degree burns allowed to heal by primary intention or delayed excision • Initial pressure therapy followed excision and grafting

• Marjolins ulcer • Chronic ulceration of old burns scar • Associated with SCC • Wide excision with potential amputation


Post- burns contracture • Prevention • • Head and neck- extended with no piillow Eyelids- ointments 3 times daily Lips- moisturizing agents Axilla- abducted Hand- elevation and apply splint in functional position Knee- extended Foot - dorsiflexed with support • THE POSITION OF COMFORT IS THE POSITION OF CONTRACTURE


• Joint exercise in full range during recovery • Pressure garments • Topical silicone sheeting • Saline expanders for scars

Treatment of contractures • Non surgical • Constant pressure dressings with splints (difficult and time consuming) • Surgical techniques • Contracture release • Z plasty with pressure dressings, splinting and exercise

SKIN GRAFTING
 to the required defective")
• Transfer of skin from one area (donor area) to the required defective area (recipient area) • It is an autograft
 • Full thickness graft")
Types • Partial thickness graft (split-thickness skin graft—SSG) • Full thickness graft

PARTIAL THICKNESS GRAFT • Also called as Thiersch graft • Is removal of full epidermis + part of the dermis from the donor area • It may be • Thin SSG • Intermediate SSG, • Thick SSG • Depends on the amount of thickness of dermis taken

Prerequisite • Healthy granulation area • β-haemolytic streptococci load less than 10 to the power of 5 per gram of tissue, otherwise graft failure will occur

Indications • Well granulated ulcer • Clean wound or defect which can not be apposed • After surgery to cover and close the defect created • For example: • After wide excision in malignancy • After mastectomy

Contraindications • SSG can not be done over • • Bone, Tendon, Cartilage, Joint

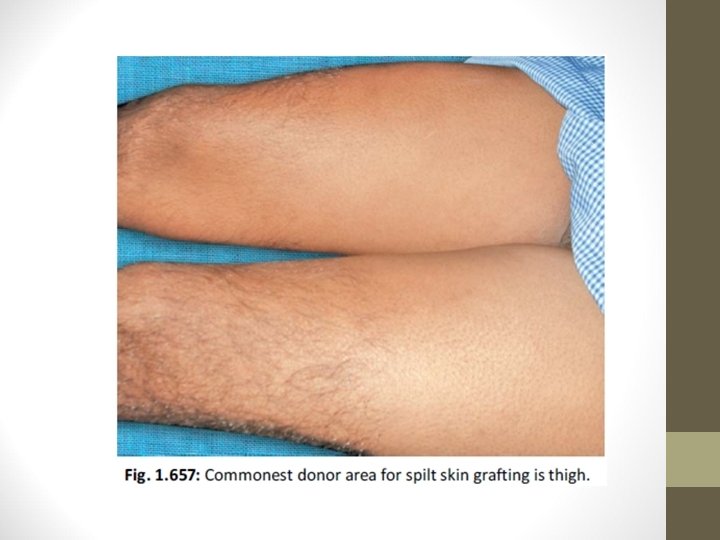
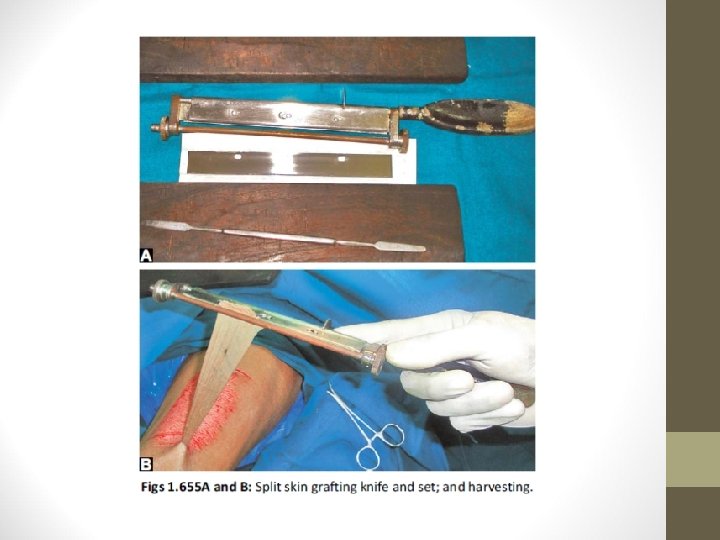
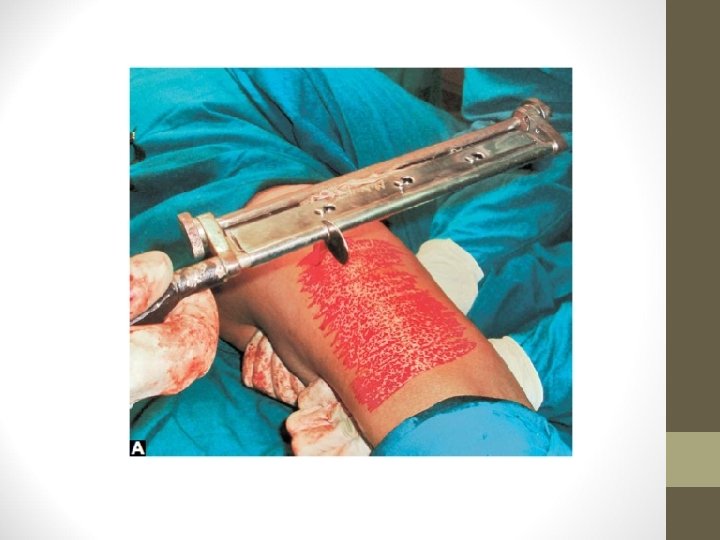
Technique • Donor sites: Thigh, arm, leg, forearm • Blade is Eschmann blade, Down’s blade • Using Humby’s knife graft is harvested • Punctate bleeding is observed which says that proper graft has been obtained




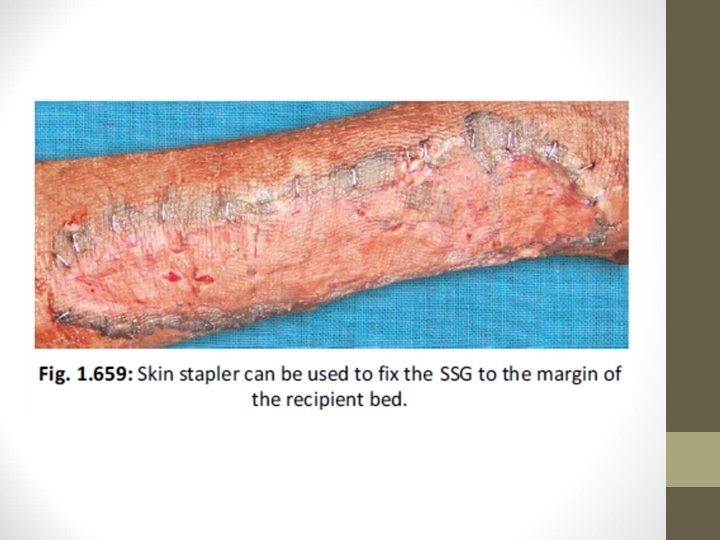

• Donor area is dressed and dressing is opened after 10 days • Window cuts in the graft are made to prevent the development of seroma • Recipient area is scraped well and the graft is placed & fixed • On 5 th day, dressing is opened and observed for graft take up • Mercurochrome is applied over the recipient margin to promote epithelialisation

Stages of Graft Intake • 1. Stage of plasmatic imbibition: Thin, uniform, layer of plasma forms between recipient bed and graft. • 2. Stage of inoculation: Linking of host and graft which is temporary • 3. Stage of neovascularisation: New capillaries proliferate into the graft from the recipient bed which attains circulation

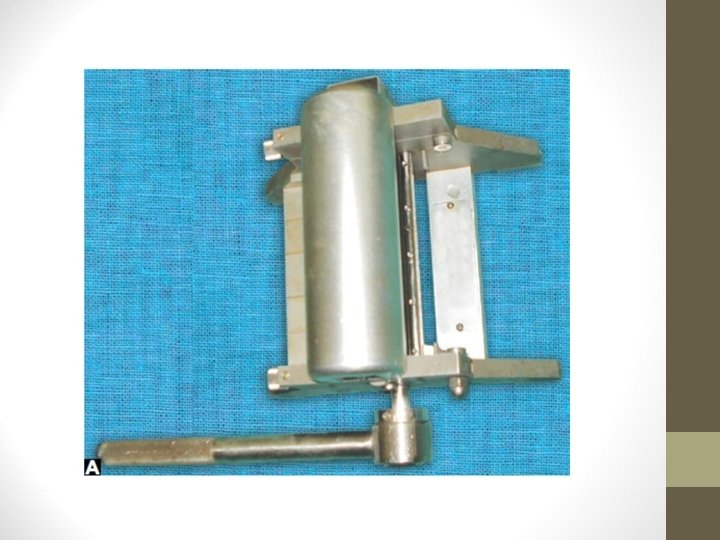
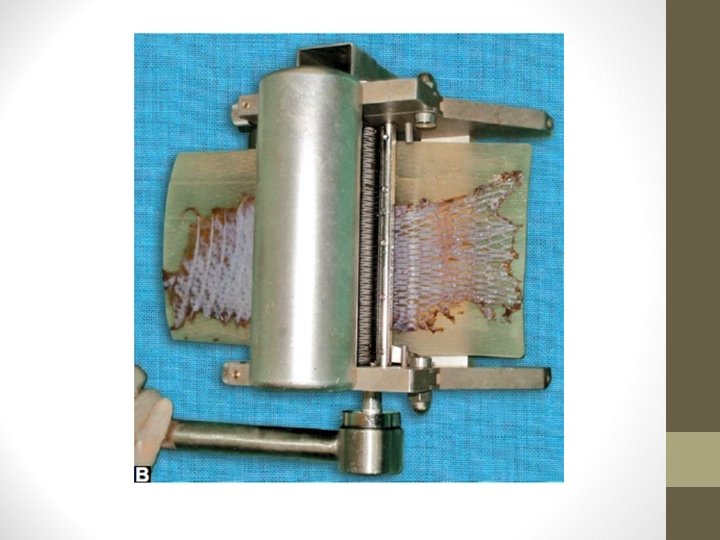
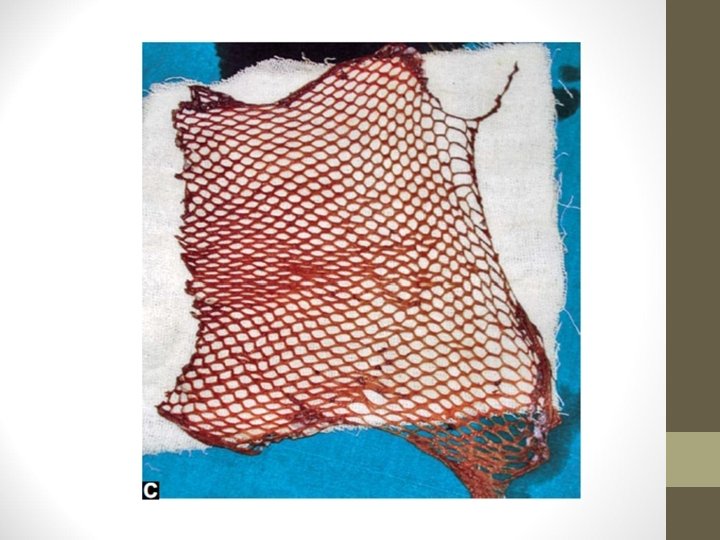
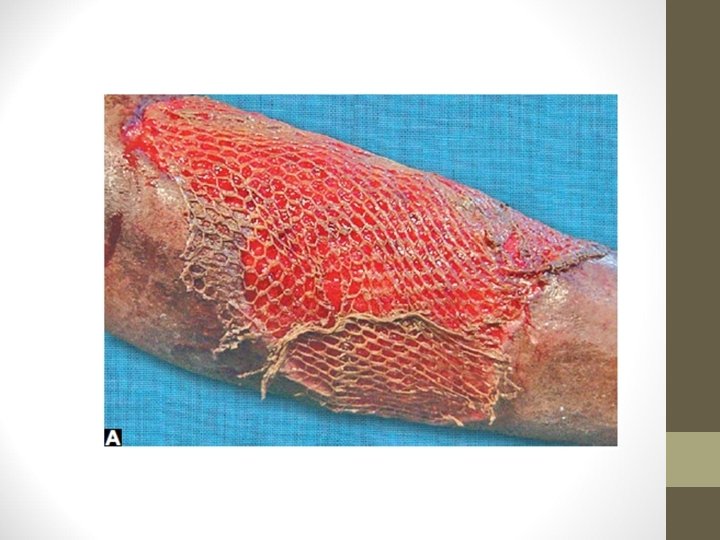
Advantages • Technically easier • Wide area of recipient can be covered • To cover large area like burns wound, graft size is increased by passing the graft through a Mesher which gives multiple openings to the graft, which can be stretched on the wider area like a net. It can cause expansion upto 6 times • Graft take up is better • Donor area heals on its own


Disadvantages of SSG • Contracture of graft. Two types: • A. Primary contracture means SSG contracts significantly once graft is taken from donor area (20 -30%). Thicker the graft more the primary contracture • B. Secondary contracture occurs after graft has taken upto recipient bed during healing period, due to fibrosis. Thinner the graft more the secondary contracture • Seroma and haematoma formation will prevent graft take up

• Infection • Loss of hair growth, blunting of sensation • Dry, scaling of skin due to nonfunctioning of sebaceous • glands. So after healing, oil (coconut oil) should be applied over the area • Graft failure

FULL THICKNESS GRAFT • Wolfe Graft • It includes both epidermis + full dermis. • It is used over the face, eyelid, hands, fingers and over the joints

Technique • It is removed using scalpel blade • Underlying fat should be cleared off properly • Deeper raw donor area is closed by primary suturing • If large area of graft is taken, then that donor area has to be covered with SSG

• Common sites of donor area • Post-auricular area • Supraclavicular area • Groin crease area

Advantages • Colour match is good, especially for face • No contracture (unlike in SSG) • Sensation, functions of sebaceous glands, hair follicles are retained better compared to SSG • Functional and cosmetic results are better

Disadvantages • It can be used only for small areas • Wider donor area has to be covered with SSG to close the defect • Can not be used to cover ulcers

THANK YOU
- Slides: 120