Burn ulcer Burn edema Reduction in RBC mass


• • • *Burn ulcer * Burn edema * Reduction in RBC mass * Burn immunology * Hormonal changes * Inhalation injury

First Degree • *Epiderm is injured • * Derm and its appendages are intact

SECOND DEGREE • *Some thickness of derm is injured • * There is injury to the dermal appendages • * But some thickness of derm and many of dermal appendages are spared

THIRD DEGREE • *Full thickness of derm is injured • * Heeling is only by contraction





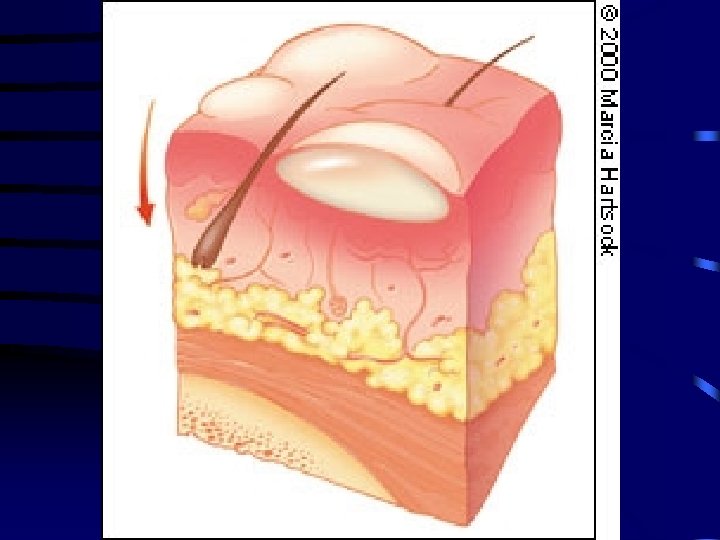

FORTH DEGREE • *Soft tissue and bone is injurred

EDEMA IN BURN PATIENT

PROBLEMES WITH EDEMA • • *Reduction in tissue oxygenation * Reduction in tissue perfusion * Increase the risk of infection * Increase the work of breathing leading to pulmonary failure

TWO KIND OF EDEMA • *FIRST Edema in burn area that is non preventable • * SECOND Edema in non burn area that is preventable

• • • * In burn area first vasoconstriction and then vasodilatation due to ischemia * Increase in gaps between cells in microvasculature for some days to some weeks * Vasoactive substances like LTs PGs oxygen radicals and histamin * Increase in intrestitial osmolarity in burned area * Probability of a systemic mediator * Hypoproteinemia

REDUCTION IN RBC MASS

40%DAMAGE OF RBC MASS • • *8% - 15% From direct injury • * 25% Due to reduced RBC

IMMUNOLOGY • • *Burn by itself * Systemic drugs * Topical drugs * General anesthesia

BURN BY ITSELF • • *Increase phagocytosis * reduced intracellular killing * reduced opsonins * reduced serum Ig level 2 days after Bu mostly Ig. M • * Reduced serum compleman • * Reduced cellmediated immunity • * Increased skin allograft survival

DRUGS • • • *Tetracyclin * Chloramphenicol * Streptomycin * Gentamicin * Kanamycin All reduce cell mediated immunity

TOPICAL DRUGS • *Acetate mafenide and silver sulfadiazin both inhibit PMN chemotaxis

General anesthesia • *Halotan Ether and N 2 Reduce mitogenic activity of lymphocyts Band T • * Phenobarbital reduce Ab production by spleen

HORMONAL CHANGES • • • *Increase in Catecholamines * “ “ GH * “ “ Cortizole * Decrease in T 3 and T 4 * “ “ serum Insuline * Serum TSH is normal

METABULISM • *Hypermetabolism 2 -4 times normal • * Most of extra blood flow is for B. ulcer • * Up reset of body thermostat is due to B receptor stimulation • * Brain deed patient have not hypermet. • * > 10% W. loss cause abnormal W. H • * > 30% W. loss is lethal • * Increase int. cellular Na due to Na and K pomp derangement

INHALATION INJURY • *20 -80% mortality is due to I. Inj • * 30 - 40% increase in mortality if I. Inj is present

PATHOGENESIS OF I. INJ. • *CO intoxication • * Direct thermal effect • * Products of combustion inhalation

CO INTOXICATION • *Competition with O 2 for Hb • * 210 times affinity for Hb • * Cytocorom system derangement in cytoplasm • * CNS derangement • * A. B. G : Lactic acidosis with low PO 2 Pa. O 2 is normal Oxy Hb saturation is low

DIRECT THERMAL INJ. • *Lower air ways are spared except for steam • * Upper air ways are more affected • * Most of edema is in first 18 -24 h • that increase breathing work or makes obstruction

PRODUCTS OF COMBUSTION • *The most common and most important part of inhalation inj. • * Aldeids Ketons and Organic materials • * Symptoms are like gastric acid aspiration Bronchoconstriction Silia paralysis Increase vessel permeability and ARDS Decrease in surfactant Prone to infection due to mucosa dam.

RESOSCITATION • COLLOID Evans N/S 1 ML/KG/% Brook R/L 1. 5 ml/kg/% Slater R/L 2 L/24 h • CRYSTALLOID Parkland Modified brook CO 1 ml/kg/% D/W 2000 cc CO 0. 5 ml/kg/% D/W 2000 cc FFP 75 ml/kg/24 R/L 4 ml/kg/% 2 ml/kg/% • HYPERTONIC SALIN Modif Monafo 180 meq Na/L (R/L+ 50 ml Na. HCo 3) /8 h then R/l after 8 h ---until 24 h • DEXTRAN FORMULA 30 ml/h DEX 40 insalin then after 8 h FFP 0. 5 ml/kg/h for 18 h U 30 -50 ml/h 2 ml/kg/h for 8 h + R/L for U

- Slides: 33