BURN Dr Yaseen Abdullah Plastic surgeon A burn

BURN Dr. Yaseen Abdullah Plastic surgeon

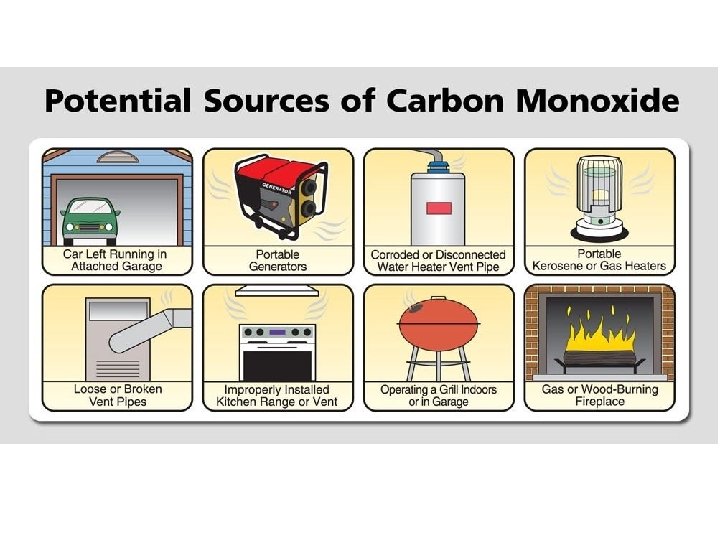
• A burn is a type of injury to skin , or other tissues , caused by – Heat (scald or fire) – Cold – Electricity – Chemicals – Radiation

The pathophysiology of burn

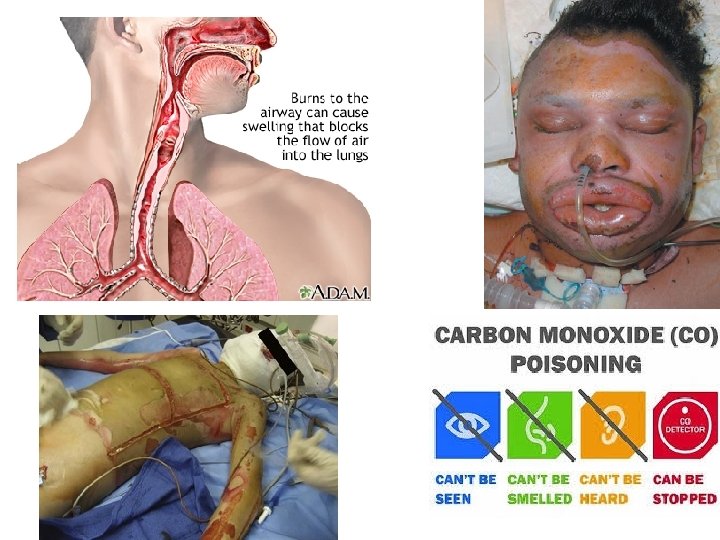
Airway and lungs

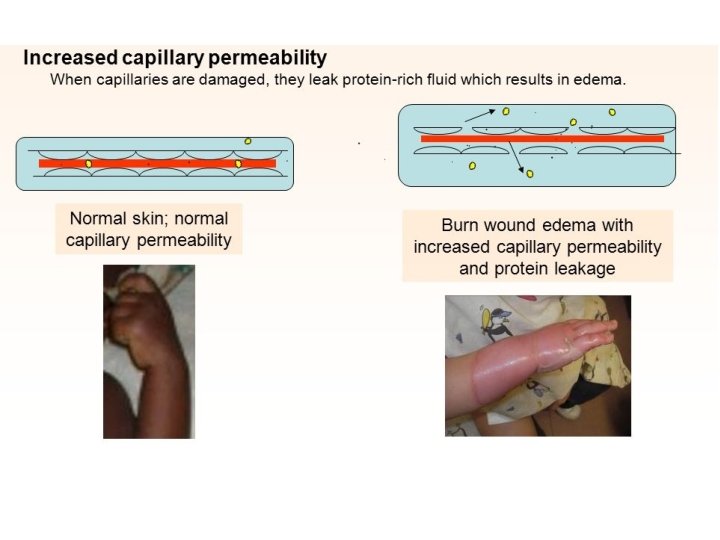
Inflammation and circulatory changes

Immediate care of the burn patient

Pre hospital care • • • Ensure rescuer safety Stop the burning process Check for other injuries Cool the burn wound Give O 2 Elevate


Hospital care

Criteria for acute admission to a burn unit: • Suspected inhalational or airway injury • Any burn likely to require fluid resuscitation(15%) • Any burn likely to require surgery(circumferential) • Face , hand , feet , major joint or perineum burn • Psychiatric patient • non accidental burn • Electrical • chemical burns • Extreme of age • Preexisting medical disorder

Airway and Inhalational injury
")
Airway(inhalational injury)

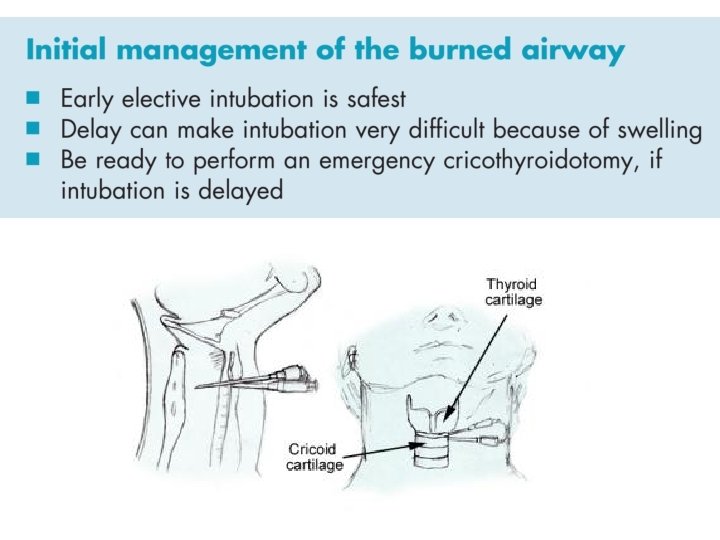
 • • Physiotherapy Nebulizer Warm humidified O 2 Escharotomy when needed")
Breathing(inhalational injury) • • Physiotherapy Nebulizer Warm humidified O 2 Escharotomy when needed

• If there is mechanical block to breathing from a circumferential chest eschar , then we have to do scoring cut through the burned skin to allow the chest to expand (escharotomy) • This is not painful (burned nerves)

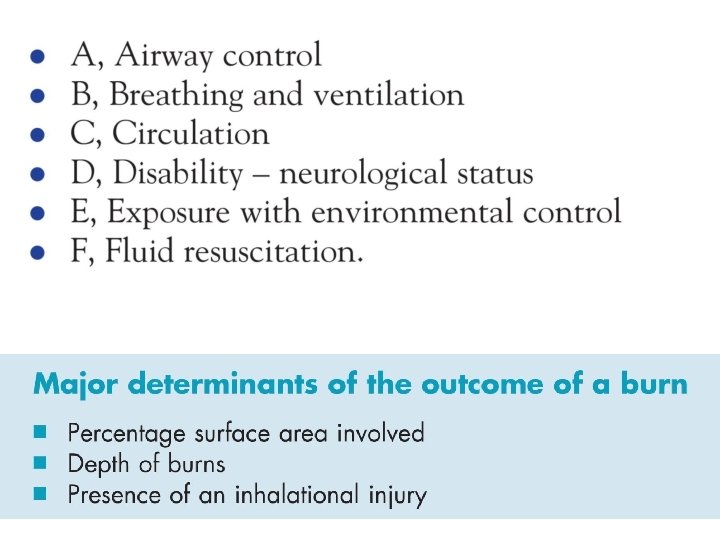
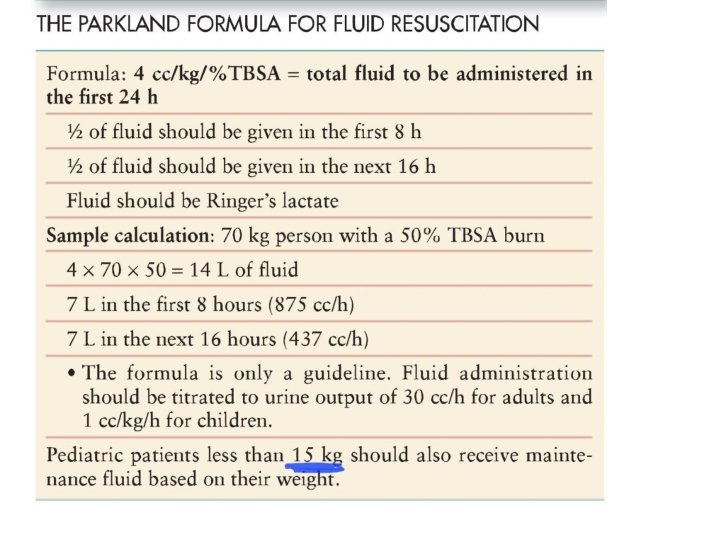
Circulation and fluid resuscitation • Partial and full thickness burn victim of more than 15 % of the total body surface area burned will have shock and require fluid resuscitation • TBSA = total body surface area
 ACCURATE")
Assessment of burn size (TBSA) ACCURATE

The patient’s palm Not the doctor’s palm

Rule of nines Not accurate but adequate for first approximation in adult only Each upper limb is 9% Each lower limb is 18% The torso is 18% each side The head and neck is 9% Genitalia is 1%

Lund browder chart Is accurate method ﻏﻴﺮ ﻣﻄﻠﻮﺏ ﻓﻘﻂ ﺍﻻﺳﻢ

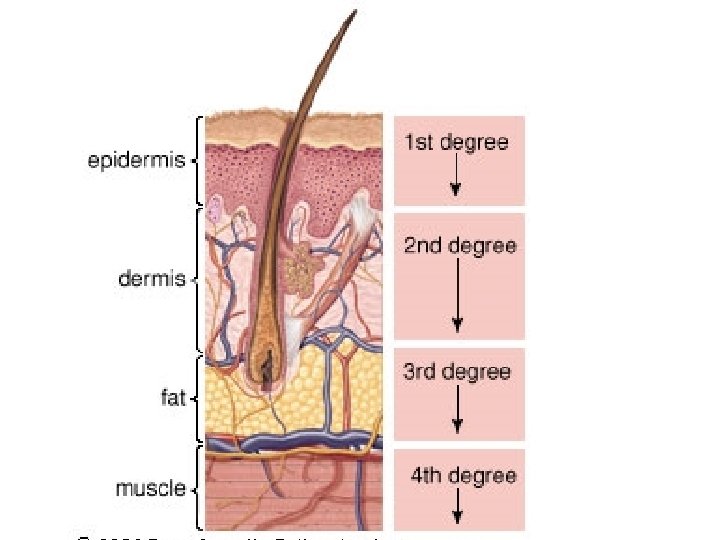
Assessment of burn depth
 • • Eg. Sun burn epidermis Dry, red , painful Treated")
First degree(superficial burn) • • Eg. Sun burn epidermis Dry, red , painful Treated with moisturizing cream for 5 days
 • Can be superficial or deep")
Second degree (partial thickness) • Can be superficial or deep

Superficial partial thickness • Papillary dermis • Moist, pink , painful , capillary refill, blister • Treated with moisturizing or antibiotic ointment for two weeks with no residual scarring

burn")
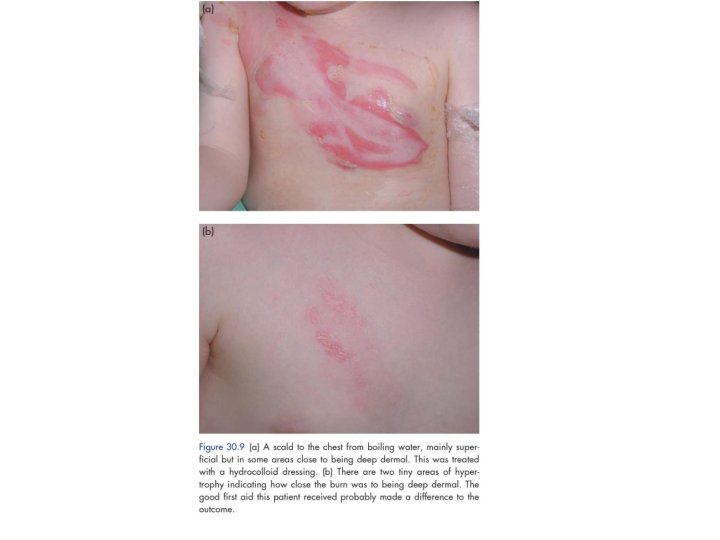
The blister of superficial partial thickness(2 nd degree)burn

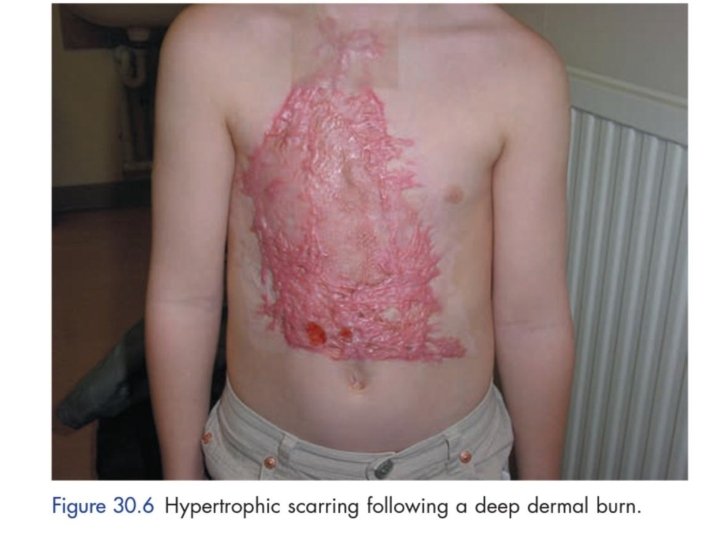
Deep partial thickness • Reticular dermis • Not moist , not blanch with pressure , decreased sensation • Treated with excision and grafting • Lead to hypertrophic scar

Deep dermal burn , tangential excision Taking skin graft Skin graft over excised burn
 • All the dermis is destroyed(reach to fatty layer) • Hard")
Third degree(full thickness) • All the dermis is destroyed(reach to fatty layer) • Hard , leathery feel , variable color (normal to black) , no capillary refill , no sensation(painless) • Treated with excision and grafting • Hypertrophic scarring

Forth degree • Eg. Electrical burn • Same as 3 rd degree with exposed tendon, bone or muscle • May require amputation

")
Circulation and fluid resuscitation (0. 5 -1 ml/kg/hour)


Treating the burn wound

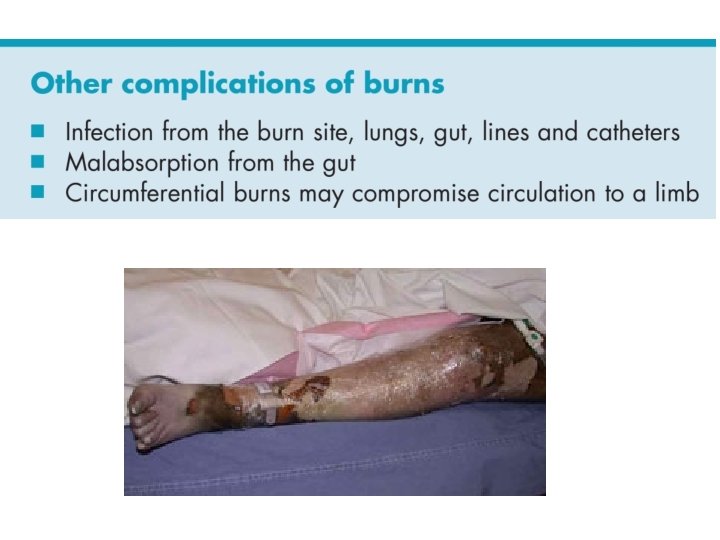
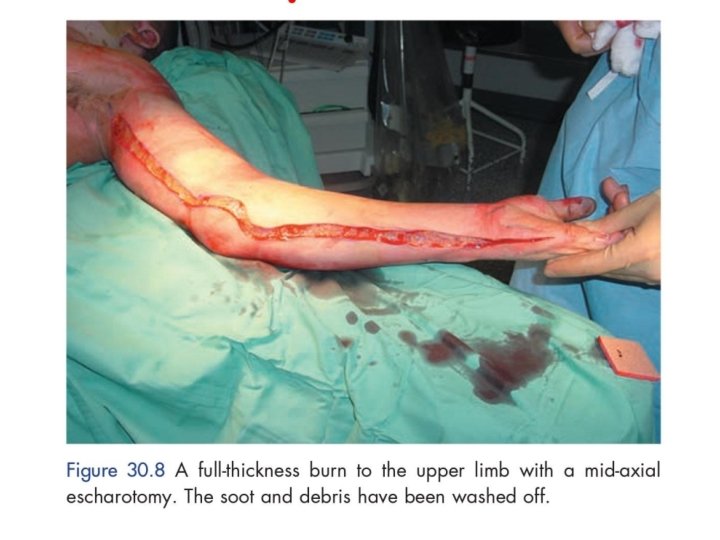
escharotomy • Circumferential full thickness burn to the limb require emergency surgery. • The tourniquet effect of this injury is easily treated by incising the whole length of full thickness burn (escharotomy).

Topical antibiotic • In non infected burn , only topical antibiotic should be used (not systemic , because of poor circulation) • Silver sulphadiazine cream 1%: broad spectrum • Silver nitrate solution 0. 5% : need to be changed frequently , cause black staining • Mafenide acetate : painful , may cause acidosis • Cerium nitrate


Additional aspect in treating burned patient • • • Analgesia Nutrition Infection control Nursing care Physiotherapy Psychological support


Post burn contractures Can be prevented by early physiotherapy and splinting
")
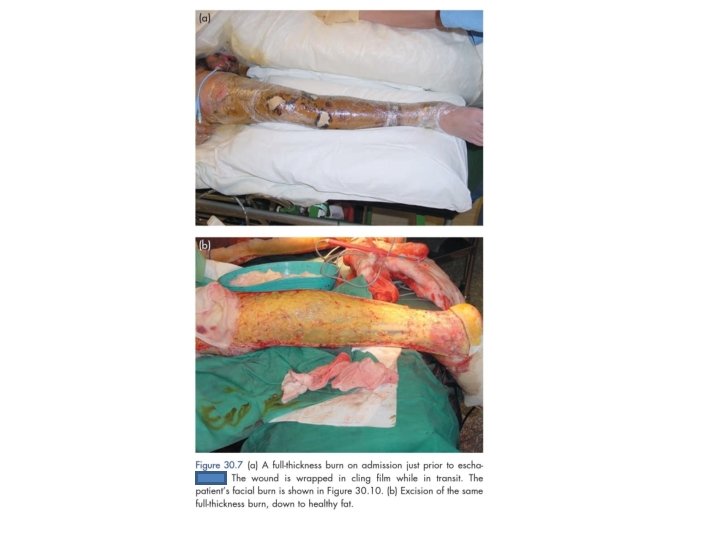
Surgery for the acute burn (excision and graft)
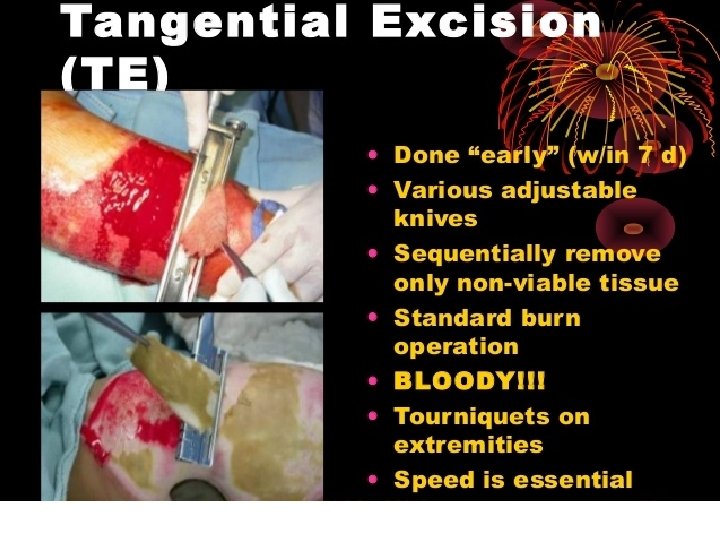
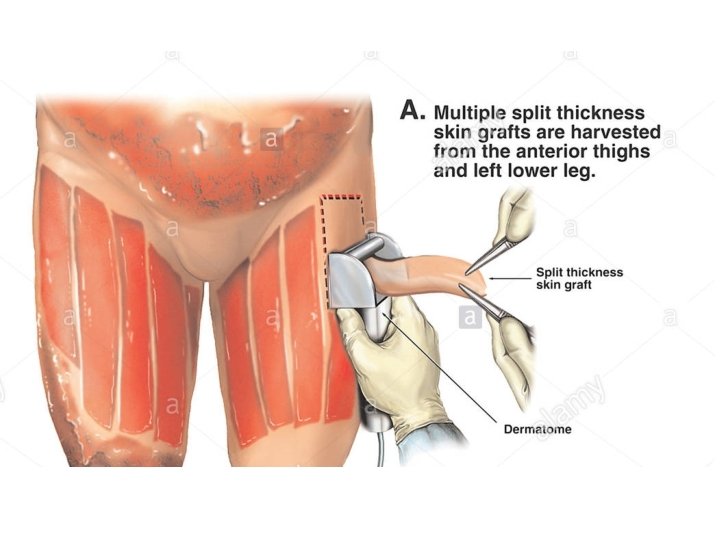

Deep dermal burn , tangential excision Taking skin graft Skin graft over excised burn
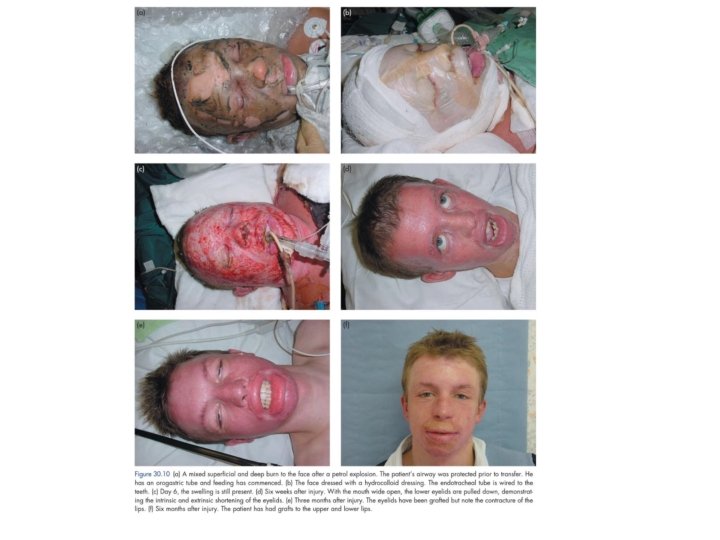
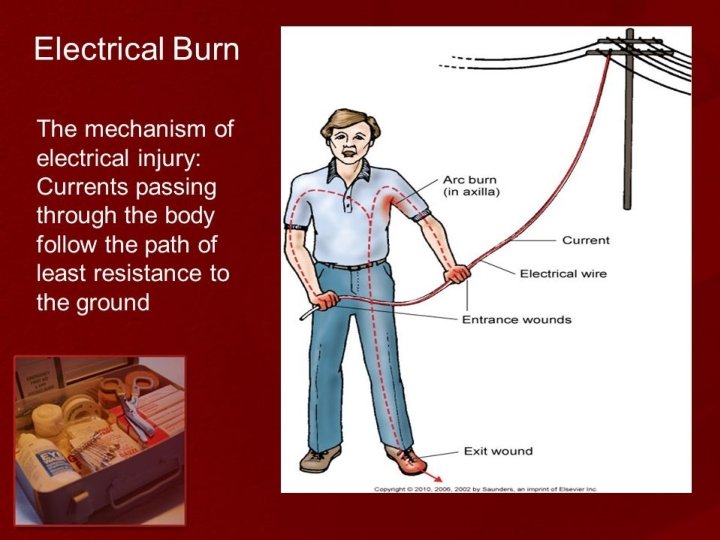

Complication of electrical injury • Cardiac arrest and myocardial damage • Compartment syndrome , amputation • Crush syndrome , myoglobinuria , acidosis and renal failure

- Slides: 63