Burn Care Tammy Henderson BSN RN Objectives Discuss

Burn Care Tammy Henderson, BSN, RN

Objectives ¡ Discuss incidence of burn in U. S. ¡ Describe factors affecting severity of burns ¡ Classify burn depth ¡ Describe initial assessment and Rule of Nines for TBSA% ¡ Describe local and systemic effects of burn injury ¡ Identify priorities of care and potential complications ¡ Calculate fluid requirements for resuscitation ¡ Discuss nurse’s role in managing burns in acute phase ¡ Use nursing process as framework to care for burn patient ¡ Describe psychological challenges for burn patients and strategies for intervention ¡ Define terms associated with burn patients

Goals related to burns • Prevention • Institution of lifesaving measures for the severely burned person • Prevention of disability and disfigurement through early specialized and individualized care • Rehabilitation through reconstructive surgery and rehabilitation programs (Wolters Kluwer Health/ Lippincott Williams & Wilkins, 2014)

Incidence: 486, 000 total 40, 000 hospitalizations ¡Over 60% of the estimated U. S. acute hospitalizations related to burn injury were admitted to 128 burn centers. ¡Such centers now average over 200 annual admissions for burn injury and skin disorders requiring similar treatment. ¡ 1/3 of the patients are pediatric

American Burn Association 2014 Repository ¡ Survival Rate: 96. 7% ¡ Gender: 69% Male, 31% Female ¡ Ethnicity: 59% Caucasian, 20% African-American, 14% Hispanic, 7% Other ¡ Admission Cause: 43% Fire/Flame, 34% Scald, 9% Contact, 4% Electrical, 3% Chemical, 7% Other ¡ Place of Occurrence: 73% Home, 8% Occupational, 5% Street/Highway, 5% Recreational/Sport, 9% Other ¡ Young children and older adults are more susceptible

Functions of the Skin ¡IInfection and injury protection ¡ Maintenance of body fluid composition ¡ Body temperature regulation ¡ Sensory contact with environment (heat, cold, pain) on and injury protection Body Sensory contact with environment

Anatomy of the Skin n Epidermis - outer thinner layer n Dermis - deeper thicker layer – contains hair follicles, sweat glands, sensory fibers n Hypodermis; Subcutaneous tissue n Largest organ in the body n Collagen-protein found in skin
- epidermis only ¡red, hypersensitive ¡Second degree (partial thickness")
Determining Burn Severity ¡First degree (superficial)- epidermis only ¡red, hypersensitive ¡Second degree (partial thickness or deep partial) epidermis, part of dermis ¡red, blistered, edematous, painful ¡Third degree (full thickness)- epidermis and dermis ¡white, loss of sensation

Superficial or 1 st degree n. Cause: Exposure to sunlight n Color: Red n Surface: Dry or small blisters n Sensation: Painful n Healing: 3 -6 days

Partial or Deep Partial Burns “ 2 nd degree” n Cause: Exposure to hot liquid, flash, flame, or chemical agent n Color: Pink or mottled n Surface: Bullae, moist weeping surface n Sensation: Painful, +/- loss of sensation (pressure intact, loss of pinprick) n Healing: superficial - 10 to 21 days deep - > 21 days, +/- graft

Partial Thickness Scald Burn

Nikolsky’s Sign

Partial Thickness “Deep”

Full Thickness or “Third Degree” ¡Cause: Prolonged exposure to flame, hot object, or chemical agent Contact with high-voltage ¡ Color: White, charred, thick ¡ Sensation: Insensate ¡ Healing: Requires grafting

Full Thickness Burn

Full Thickness Burn

Factors to Consider with Extent of Burn Injury • How the injury occurred • Causative agent • Temperature of agent • Duration of contact with the agent • Thickness of the skin
 instant")
Temperature and Duration are the KEY! n 70 o C (160 o. F) instant full-thickness n 65 o C (149 o. F) instant partial-thickness n 60 o C (140 o F) 2. 0 seconds n 55 o C (131 o F) 7. 5 seconds n 50 o C (122 o F) 1. 5 minutes

Pediatric Skin Thickness Child Adult Almost instantaneous Full Thickness Burn 1600 F Tissue Destruction: 5 Sec. 1400 F Almost instantaneous Full Thickness Burn Severe Damage: 10 Sec. 1300 FSevere Damage: 30 Sec. Tolerated for Time 1110 F Tolerated for Time

Initial Assessment. Pre-hospital n. Stop the burning process Ø Remove clothing from involved areas Ø Flush areas in contact with chemical Ø Remove contact with electrical injury n Universal Precautions n Prevent Hypothermia - Clean Dry Sheet n Infuse warm fluids

Limited Role for Cold Water Soaks ¡ Use only for burns less than 25% TBSA ¡ May reduce pain of second degree ¡ If applied within 10 minutes of burn, may tissue damage ¡ Hypothermia must be avoided ¡ Clean Dry Sheet following cooling decrease
 ¡ Breathing (breath sounds,")
Initial Management ¡ Airway (jaw lift, chin thrust, oral airway) ¡ Breathing (breath sounds, 15 liters oxygen) ¡ Circulation (pulses, perfusion) ¡ C-spine (stabilize as necessary) ¡ Cardiac (electrical injuries) ¡ Disability (AVPU) ¡ Expose and Examine ¡ Fluid Resuscitation (IV access, burn OK)

Rule of Nines

Extent of Burn Injury ¡Rule of Nines” ¡ Include second and third degree only ¡From time of burn injury ¡ increase initial volume if delay in resuscitation ¡ Usually only needed for burns > 15% TBSA ¡ Modification for children ¡ Limited extent burns (palm = 1%)
 x")
Fluid Resuscitation=Priority ¡ Consensus Fluid Formula 2 -4 cc LR x Weight (kg) x % TBSA burn ¡ Give half over first 8 hours ¡ Give remainder over next 16 hours ¡Titrate volume resuscitation to urine output and blood pressure

Massive Fluid Requirements ¡ Example: 70 kg man with 50% TBSA 4 cc x 70 kg x 50% TBSA = 14, 000 cc ¡ First 8 hrs: 7000 cc or 875 cc/hr ¡ Next 16 hrs: 7000 cc or 437 cc/hr Titrate volume resuscitation to urine output

Special Fluid Requirements ¡ Increased Fluid Requirements ¡ ¡ Electrical Injury Inhalational Injury Delayed Resuscitation Prior Dehydration (diuretics, alcohol) ¡ Volume Sensitive Patients ¡ Pre-existing cardiopulmonary disease ¡ Extremes of age

High Voltage Injury

Zones of Cellular Injury= Local Response to Burn Injury Zone of Coagulation Zone of Stasis Zone of Hyperemia


Conversion of Partial Thickness to Full Thickness

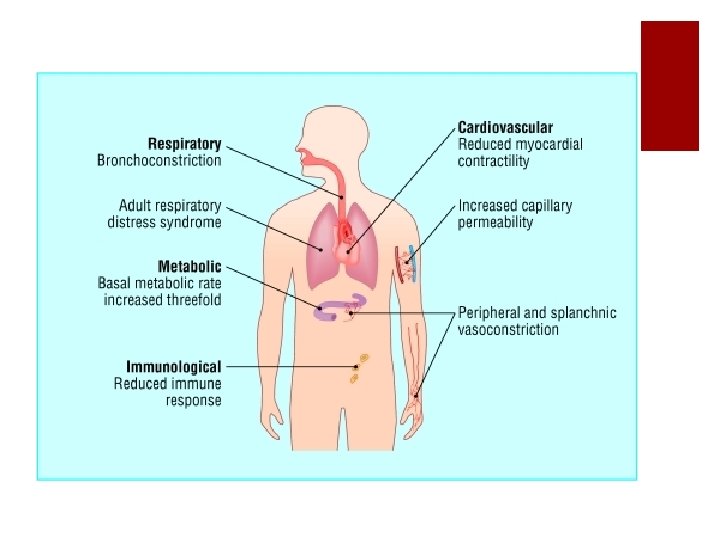
Systemic Response to Burn Injury The release of cytokines and inflammatory mediators Fluid and electrolyte shifts-shock and “third spacing” Cardiovascular changes Respiratory changes Metabolic changes. Immunological changes Inadequate thermoregulation

Phases of Burn Injury ¡Refer to Table 62 -3 ¡Emergent or resuscitative phase ¡ Onset of injury to completion of fluid resuscitation ¡Acute or intermediate phase ¡ From beginning of diuresis to wound closure ¡Rehabilitation phase ¡ From wound closure to return to optimal physical and psychosocial adjustment

Emergent or Resuscitative Phase ¡Patient is transported to emergency department ¡Determine TBSA and begin fluid resuscitation ¡Foley catheter ¡Full set of labs including carboxyhemoglobin ¡Patient with burns exceeding 20% to 25% should have an Ng tube inserted and placed to suction ¡Patients with electrical burns should have ECG ¡Address pain, pulses, ventilatory support, circumferential burns ¡Psychosocial consideration and emotional support

Carbon Monoxide Poisoning ¡ Cause of most fatalities at scene ¡ Carbon monoxide binds to hemoglobin with 200 x higher affinity than oxygen ¡ 100% oxygen decreases half-life by 5 x ¡ Carboxyhemoglobin levels: ¡ 40 -60 obtundation, LOC 15 -40 CNS dysfunction 5 - 15 smokers <5 normal

Escharotomy ¡ Bedside procedure ¡ Incision made through eschar to relieve circulatory or respiratory compromise ¡ ¡ Chest Extremities Fingers Neck (rare)

Escharotomy Eschar: the tough leathery tissue remaining after a full thickness burn

Fasciotomy

Standard Excision and Grafting

Donor Site

Mesh Expansion of Skin Graft

Contractures

Use of the Nursing Process in the Care of the Patient in the Emergent Phase of Burn Care—Diagnoses ¡Impaired gas exchange ¡Ineffective airway clearance ¡Fluid volume deficit ¡Hypothermia ¡Acute pain ¡Anxiety

Potential Complications • Inhalation injury-pneumonia, ARDS, respiratory failure • Under resuscitated-organ failure, renal failure, shock • Over resuscitated- cardiopulmonary edema • Circumferential burn-Compartment Syndrome • Infection- sepsis, UTI, cellulitis, bacteremia • Death

Rehabilitation Phase ¡Rehabilitation is begun as early as possible in the emergent phase and extends for a long period after the injury. ¡Focus is on wound healing, psychosocial support, self-image, lifestyle, and restoring maximal functional abilities so the patient can have the best quality life, both personally and socially. ¡The patient may need reconstructive surgery to improve function and appearance. ¡Vocational counseling and support groups may assist the patient.

Psychological Challenges

New Technology ¡Face transplant ¡ https: //www. facebook. com/techinsider/videos/434597 810071914/

Questions?
- Slides: 49