BUGANDO MEDICAL CENTER CONTINUOUS MEDICAL EDUCATIONCME REHABILITATION TO
 REHABILITATION TO PATIENTS WITH STROKE 28 -SEPTEMBER-2017")
BUGANDO MEDICAL CENTER CONTINUOUS MEDICAL EDUCATION(CME) REHABILITATION TO PATIENTS WITH STROKE 28 -SEPTEMBER-2017

PRESENTATION OVERVIEW �Introduction �Definition �Epidemiology/Etiology �Clinical classification �Risk factors �Signs and symptoms �Management -Physiotherapy -Occupational therapy -Prosthetic and Orthotic

DEFINITION Stroke – Sudden neurological deficit of a vascular origin lasting for 24 hours or longer with focal or global disturbance to cerebral function. TIA – Neurological deficit resolves in less than 24 hours. – Most TIAs last <1 h

EPIDEMIOLOGY/ETIOLOGY �According to WHO, -15 million people suffer stroke worldwide each year. -5 million die -5 million are left permanently disabled. �The 2010 Global Burden of Disease Study suggested Stroke is -the second leading cause of death globally -the third leading cause of premature death and disability -kills more than 49, 000 people each year in the UK, nearly 1 in 10.

EPIDEMIOLOGY/ETIOLOGY - the fourth largest cause of death in the UK after cancer, heart disease and respiratory disease. �The lowest incidence and mortality rates in 2010 were in High Income North America, Australasia, and Western Europe, whereas the highest rates were in Central Asia, Southeast Asia, and sub-Saharan Africa

BMC PHYSIO STATISTICS 2015 “INPATIETS”-NEW Months Jan Feb March Apr May June July Aug Sept Oct Nov Dec TOTAL F 6 1 1 8 10 4 2 7 3 3 1 50 M 3 2 6 6 10 7 6 5 GRAND TOTAL 4 5 100 50

OUTPATIENTS 2016 SEX F M Number 110 114 GRAND TOTAL 224

CLINICALLY RELEVANT ANATOMY
 �Hemorrhagic (15%) �Atria fibrillation 17% �Aneurismal 4% �Carotid disease")
CLINICAL CLASSIFICATION-SUMMARY �Ischemic stroke/TIA (85%) �Hemorrhagic (15%) �Atria fibrillation 17% �Aneurismal 4% �Carotid disease 4% �Hypertensive 7% �Others 64% �Others 4%
 �Occlusive: �Thrombosis �Embolism Anterior Circulation �Occlusion")
CLASSIFICATION OF STROKE Ischemic Stroke (85% “Brain Infarct”) �Occlusive: �Thrombosis �Embolism Anterior Circulation �Occlusion of carotid artery involve cerebral hemispheres Posterior Circulation �Vertebro-basilar artery distribution involve brainstem or cerebellum
 �Arteriovenous malformation �Intracerebral �Hypertension (most")
CLASSIFICATION OF STROKE Hemorrhagic Stroke �Subarachnoid �Aneurysm (most common) �Arteriovenous malformation �Intracerebral �Hypertension (most common) �Amyloid angiopathy in elderly

STROKE – RISK FACTORS • • Modifiable Hypertension Tobacco use Hx of TIA’s Heart Disease Diabetes Mellitus Hypercoagulopathy � Pregnancy, cancer etc. Sickle Cell and increased RBC Hx of carotid Bruit None modifiable �Age �Gender �Race �Previous CVA �Heredity
 �Numbness (opposite side) �Language")
SIGNS AND SYMPTOMS �Ischemic �Carotid Circulation �Unilateral paralysis (opposite side) �Numbness (opposite side) �Language disturbance �Aphasia – difficult comprehension, difficult reading/writing �Dysarthria – slurred speech, abnormal pronunciation. �Visual disturbance (opposite side) �Monocular blindness (same side)

STROKE – SIGNS AND SYMPTOMS Ischemic �Vertebrobasilar Circulation �Vertigo �Visual disturbance �Diplopia �Ocular palsy – inability to move to one side �Dysconjugate gaze – asynchronous movement �Paralysis �Numbness �Dysarthria �Ataxia

STROKE – SIGNS AND SYMPTOMS �Hemorrhagic Subarachnoid hemorrhage �Sudden severe HA �Transient LOC �Nausea/Vomiting �Neck pain �Intolerance of noise/light Intracerebral hemorrhage � LOC, N/V

MANAGEMENT �Acute medical care �rehabilitation

ACUTE MEDICAL CARE �Diagnosis: �CT SCAN to differentiate ischemic from hemorrhagic �BP control �If diastolic is > 140 �Elevated levels of diastolic > 110 can be treated on the second day Oral CCB, ß-blockers, ACEi. �BP is always elevated in the acute phase as a compensation made by the body. � There is auto-regulation of the cerebral circulation so the actual cerebral blood flow is usually satisfactory. � BP will return to normal over a week in most cases �Cardiac stabilization �Convulsions control �Swallowing assessment

REHABILITATION v. Physiotherapy v. Occupational therapy v. Speech therapy v. PNO

PHYSIOTHERAPY �Primary goals: ØPrevent complications ØMinimize impairments ØMaximize function

PHYSIOTHERAPY Involves Two Phases, ØAcute Phase ØRehabilitation Phase should be involved early Ø-make own assessment Ø-complete work up Øearly mobilization is associated with better outcomes

Acute phase: Assessment: Ø observation e. g. mouth deviation, bed sores, NGT, Cannula etc. Ø vital signs e. g. BP, PR, Temp. , SO 2 Ø functional e. g. ADL’S Ø neurological e. g. GCS, muscle tone, reflexes , sensation, proprioception

Acute Phase: ØUse of standardized evaluations and validated assessment tools e. g. -Motricity Index - trunk control test -Barthel Index

Acute Phase: �Motricity Index

Acute Phase: �Barthel Index

Acute Phase: �What we do, Øpassive mobilization ØBed mobility - turning Øsitting balance training Øsit-to-stand training Østanding balance training Ø balance training during various activities Øbody-weight supported training
 ØBilateral arm training ØTrunk stability")
Acute Phase: ØWhat we do, ØSupportive techniques (Subluxed shoulder) ØBilateral arm training ØTrunk stability training Ø-Devices (P&O Unit)
 gait and mobility-related functions and activities")
ØRehabilitation Phase: � can be divided into: (1) gait and mobility-related functions and activities -circuit class training -caregiver-mediated exercises (2) interventions related to arm-hand activities (3) interventions related to activities of daily living (4) strengthening exercises (5) neurological treatment approaches, e. g. (PNF).

ØRehabilitation Phase: �Can also be specific in the following areas: vmuscle and movement functions e. g. -muscle power functions -control of voluntary movement functions -muscle tone functions

ØRehabilitation Phase: vjoint and bone functions e. g. mobility of joints vsensory functions e. g. -proprioceptive -touch -sensory functions related to temperature and other stimuli

ØRehabilitation Phase: vgait pattern functions e. g. -gait speed -gait stance abnormality vcardiovascular and respiratory systems e. g. -exercise tolerance functions

ØRehabilitation phase: vbalance and coordination e. g. -changing basic body position -maintaining a body position vwalking e. g. -distance - independence - falls varm-hand activities e. g. -fine hand use -hand arm use

OCCUPATIONAL THERAPY.

OCCUPATIONAL THERAPY MANAGEMENT �Occupational therapist focuses on v. Independence and Function v. Individualized goal setting. v. Specific skills , task adaptation and environmental modification. v. Facilitation of occupational balance between work, rest and play/leisure activities
 �Re –education of sensory")
OT management at acute stage �Emphasis on posturing (handling techniques) �Re –education of sensory loss �Cognitive skills re training �Bed mobility �Oral therapy

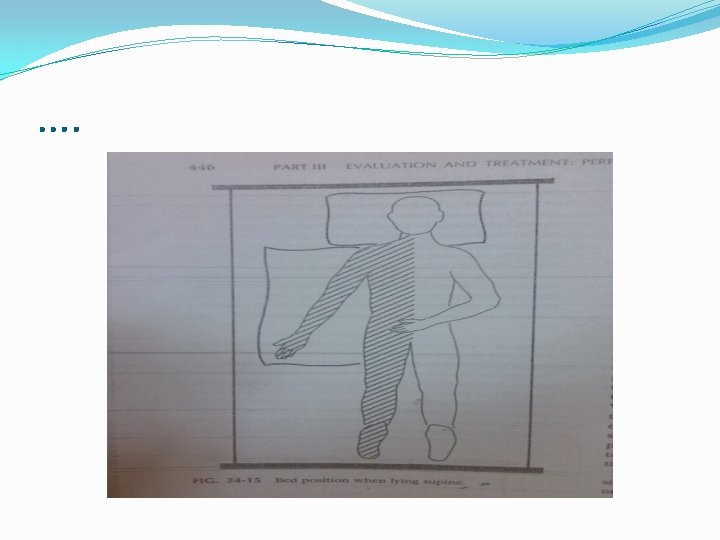
BED POSITION ACUTE STAGE

ASSESSMENT & INTERVENTION �The Occupational Therapy assessment begins by history taking to identify ability and deficit to establish base line for OT program. �Performance Areas v Self -care v Productivity v Leisure

SELF CARE PRODUCTIVITY

LEISURE

Performance Components v. ROM, Ms tone, Ms strength v. Gross motor coodination v. Hand function ( fine motor co-ordination, manipulation and dexterity) v. Coordination v Sensation

Cont… v Perception-Visual perception v Memory v. Endurance and work tolerance v Psychosocial skills v. Psychological skills v. Balance and postural control v. Cognition skills and Perception v. Communication and language skills
 v. Social (Roles in the")
Performance context v. Physical (Home assessment , working area) v. Social (Roles in the family and community) v. Culture

ASSESSMENT AND TREATMENT Standardized Assessment Tools e. g. Modified Barthel Index Assessment of Motor and Processing skills Different treatment approaches e. g. Rehabilitation Applied Frame of reference. Neurodevelopment Applied frame of reference.

General aims for OT treatment � Family and patient education (about condition, prognosis, coping strategies) � Improve physical function: to reinforce normal patterns of movement during activity and to avoid abnormal movement during activity � Establish optimal independence in ADL � Alleviate communication problems � Alleviate perceptual problems � Assist in resettlement

Orthotic management of stroke

Introduction �A comprehensive review of the orthotic management of stroke was undertaken by ISPO in 2003 as part of a multidisciplinary consensus conference. Definitions � orthotic is the science deals with orthoses

Defn cont… �ORTHOSES are an externally applied devices used to modify the structural and function characteristics of the neuromuscular and skeletal system � Example of post stroke deformities: wrist drop , foot drop(equinus), knee instability (genu recuvatum, valgum, varus etc.

Why orthoses on stroke pt �Controls gait deviations �Correct & prevents further deformities �Compensation Types of orthoses and designs are prescribed based on biomechanical functions

Wrist drop

Foot drop

Knee instability

�Good and early orthotic intervention can enhance and optimize the effect of other services such as physiotherapy and potentially minimize the need for long term care by preventing secondary complications.

THANK YOU
- Slides: 53