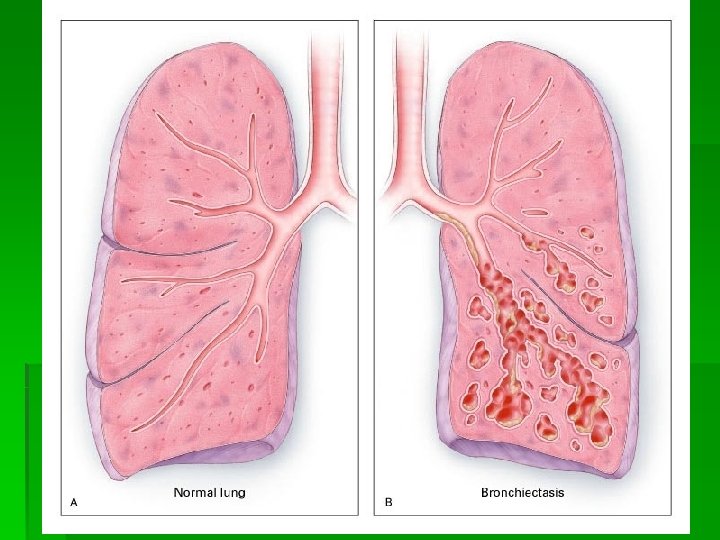
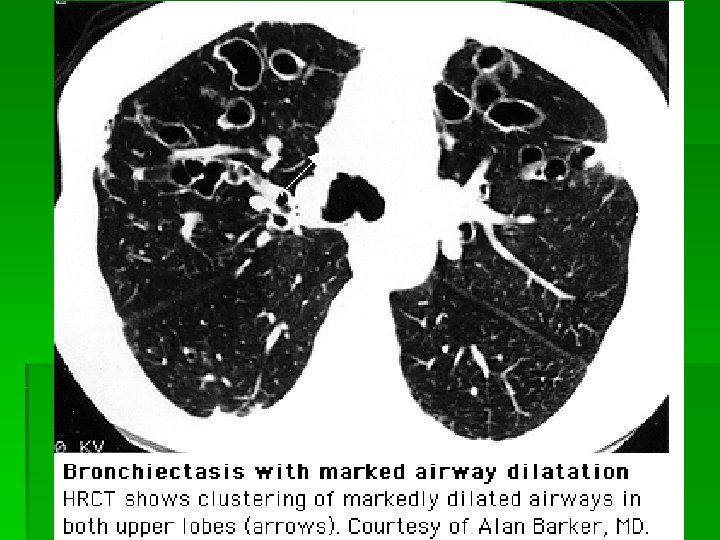
Bronchiectasis Dilated airways with frequently thickened walls Bronchiectasis

Bronchiectasis Dilated airways with frequently thickened walls

Bronchiectasis: Clinical Note: Bronchiectasis may happen 2/2 COPD or may be a separate process with very similar symptoms Clinical: § Cough (90 %) § Daily sputum production (76%) § Dyspnea (72%) § Hemoptysis (56%) § Recurrent pleurisy

Pathophysiology 2 Prerequisites: § Infectious insult § Impairment of drainage, airway obstruction, and/or a defect in host defense.

Pathophys Continued § Infection: Bacterial, mycobacterial, esp. ABPA central airway bronchiectasis § Airway obstruction: intraluminal tumor, foreign body, lymph nodes, COPD § Immunodeficiency: ciliary dyskinesia, HIV, hypogammaglobulinemia, cystic fibrosis (obstruction and immunodef. )

Note: this table compares primary bronchiectasis with COPD
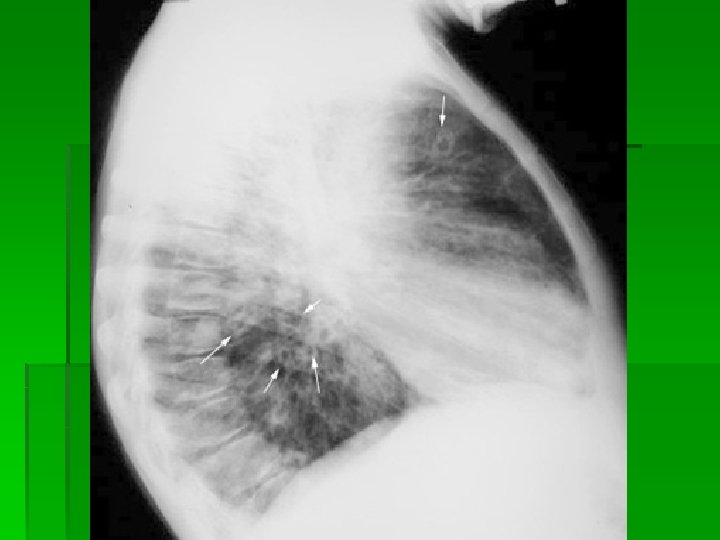

Characteristic central bronchiectasis 2/2 ABPA

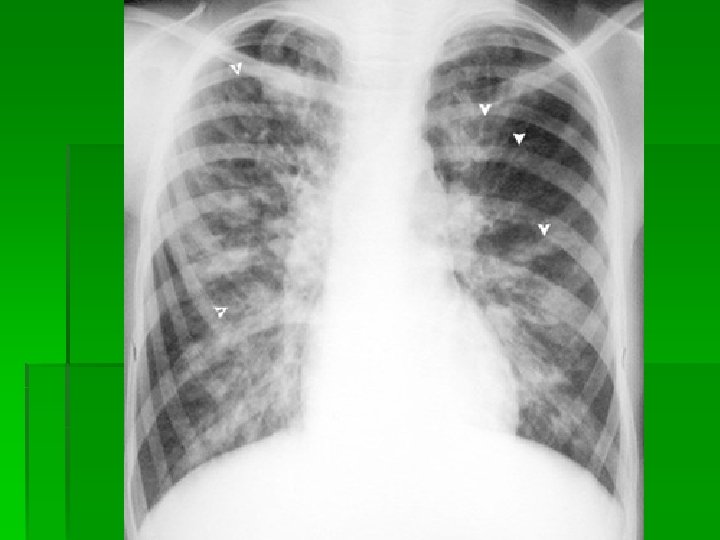
Note characteristic location in the upper lobes and superior segments of lower lobes

Exacerbation

Exacerbation: Etiology +Rx Colonization/infection: § Hemophilus § Pseudomonas § MAI § Aspergillus Very difficult to distinguish colonization from acute infection with these bugs. Psuedomonas colonized more bronchiectasis on CT; increased number of hospitalizations vs H. flu colonization Effect of sputum bacteriology on the quality of life of patients with bronchiectasis. Wilson CB; Jones PW; O'Leary CJ; Hansell DM; Cole PJ; Wilson R Eur Respir J 1997 Aug; 10(8): 1754 -60. Treatment: fluoroquinolone

Prevention § Antibiotics-Controversial: Consider Macrolide TIW Cipro qd X 7 -14 D/ month § Bronchial Hygiene, physiotherapy, pulmonary rehab § ? bronchodilators, and steroids § Surgery

Citations All material from Uptodate. com unless otherwise noted
- Slides: 16