BRONCHIECTASIS DEFINITION Bronchiectasis is defined as permanent abnormal

BRONCHIECTASIS
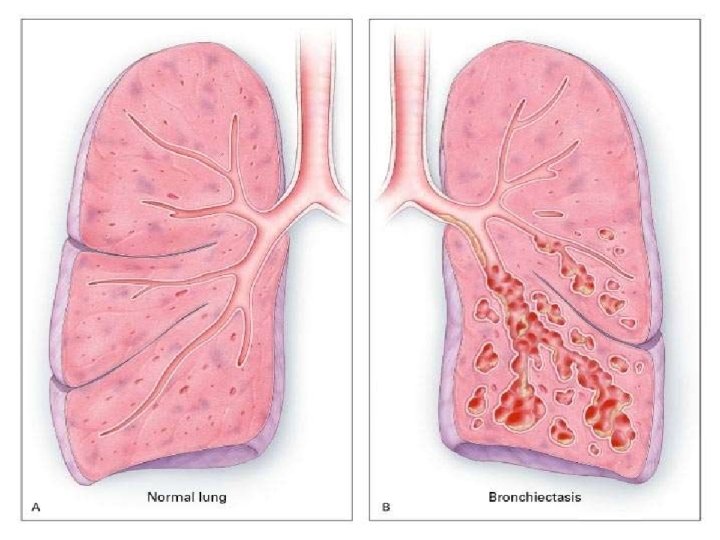

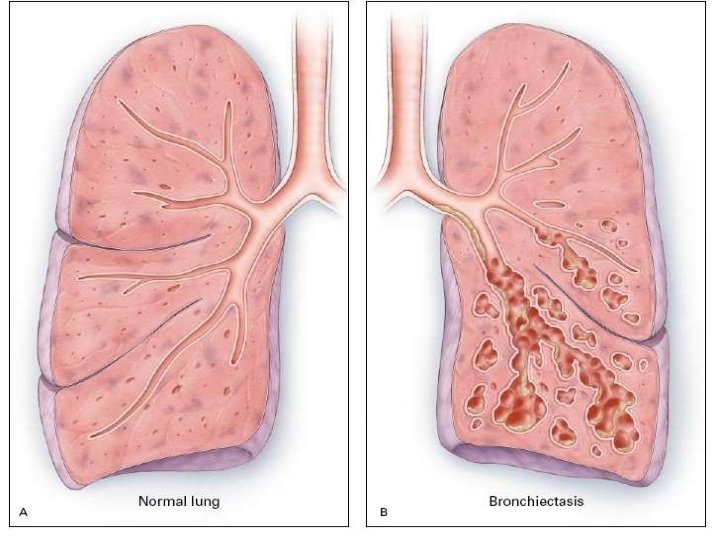
DEFINITION: �Bronchiectasis is defined as permanent, abnormal dilatation of one or more large bronchi.

DEFINITION: Bronchiectasis is defined as abnormal and irreversible dilatation of the bronchi and bronchioles (greater than 2 mm in diameter) developing secondary to inflammatory weakening of bronchial walls.

THE YELLOWISH DISCOLORATION OF LUNG PARENCHYMA REFLECTS OBSTRUCTIVE PNEUMONIA.

CAUSES �Tuberculosis, �pneumonia, �inhaled foreign bodies, �Allergic and bronchiol tumours.

INFECTIVE CAUSES ASSOCIATED WITH BRONCHIECTASIS INCLUDE �infections caused by the Staphylococcus, Klebsiella, or Bordetella pertussis, the causative agent of whooping cough.
,")
ASPIRATION OF AMMONIA AND OTHER TOXIC GASES, �pulmonary aspiration, �alcoholism, �various heroin (drug use), allergies all appear to be linked to the development of Bronchiectasis
, which predisposes patients to a variety of pulmonary")
�Childhood Acquired Immune Deficiency Syndrome (AIDS), which predisposes patients to a variety of pulmonary ailments, such as pneumonia and other opportunistic infections. �Inflammatory bowel disease, especially ulcerative colitis.

CONGENITAL CAUSES �Patients with alpha 1 -antitrypsin deficiency have been found to be particularly susceptible to bronchiectasis,

MORPHOLOGICAL TYPES �Cylindrical or tubular bronchiectasis �Varicose �saccular or cystic bronchiectasis

CYLINDRICAL OR TUBULAR BRONCHIECTASIS

4. Diagnosis – Chest CT Varicose bronchiectasis

CYSTIC BRONCHIECTASIS

Cystis / saccular bronchiectasis


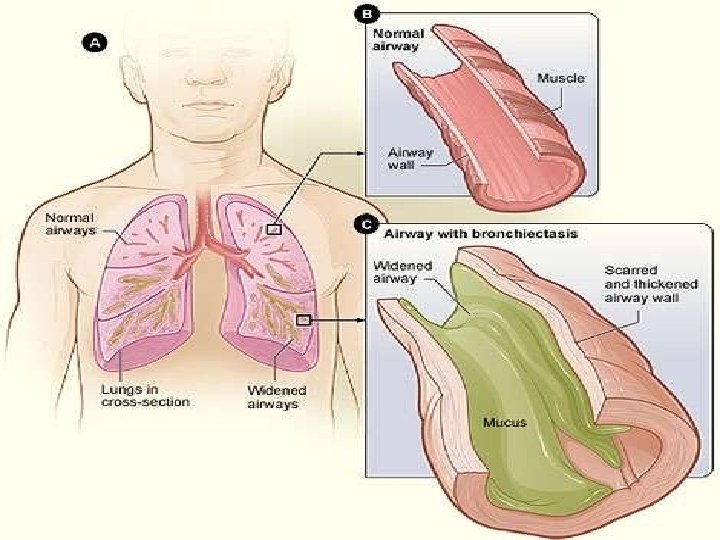
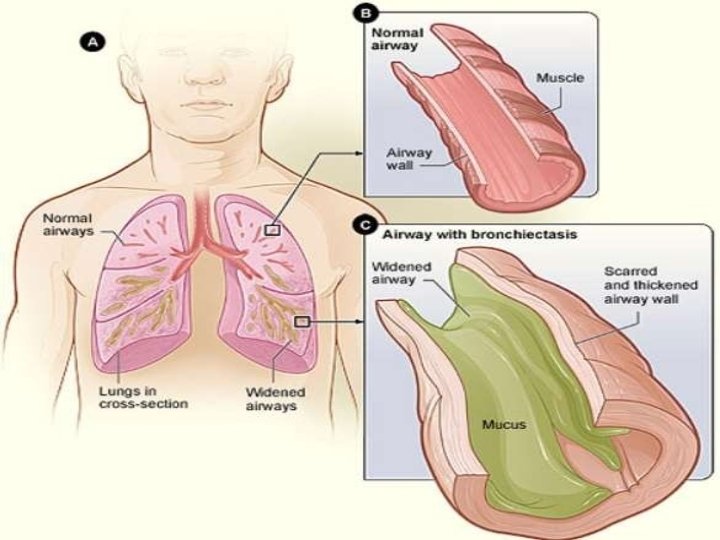
Due to etiological factor Inflammation of bronchial wall causing Loss of supporting structure Result in Thick sputum that obstruct the bronchi The bronchial wall become permanently dialated

PATHOPHYSIOLOGY � Dilation and distortion of the bronchi � Damage of airway epithelium � Dilation and hyperplasia of blood capillary

CLINICAL MANIFESTATION 1. The production of large quantities of purulent and often foul-smelling sputum. The volume of sputum can be used for estimating the severity of the disease � Mild < 10 m. L � Moderate 10~150 m. L � Severe >150 m. L

2. Chronic cough 3. Hemoptysis: � Frequent �More commonly in dry variety �Usually mild (blood streaking of purulent sputum) �Massive hemoptysis is usually from dilated bronchial arteries or bronchialpulmonary anastomoses under systemic pressure

SIGNS AND SYMPTOMS �Chronic cough with foul smelling sputum production, �Some people with bronchiectasis may produce frequent green/yellow sputum (up to 240 ml daily). �Bronchiectasis may also present with hemoptysis �Pneumonia � Bad breath indicative of active infection. �Frequent bronchial infections and breathlessness are two possible indicators of
 scan �Blood tests")
DIAGNOSTIC EVALUATION: �History and physical examination �Chest x-ray �CT (computerised tomography) scan �Blood tests �Testing of the mucus to identify any bacteria present �Checking oxygen levels in the blood �Lung function tests (spirometry).

Dilated bronchus BRONCHIECTASIS

COMPLICATIONS �Haemoptysis, major pulmonary haemorrhage. �COPD, �emphysema, � chronic respiratory insufficiency

COMPLICATION Local complication �Recurrent pneumonia �Lung abcess �Empyema �Hemoptysis �Pulmonary hypertension

TREATMENT � Treatment of bronchiectasis includes � controlling infections and bronchial secretions, � relieving airway obstructions, � removal of affected portions of lung by surgical removal or artery embolization � preventing complications.
Treatment of infection, particularly during acute exacerbations (2)")
TREATMENT Therapy has several major goals: (1)Treatment of infection, particularly during acute exacerbations (2) Improved clearance of tracheobronchial secretions (3) Reduction of inflammation (4) Treatment of an identifiable underlying problem
 Expectorant (Mucinex) 2)")
TREATMENT � Medical management 1. Improving the drainage of airway 1) Expectorant (Mucinex) 2) Bronchodilators (Salbutamol, theophilline, Derriphyl lin) 3) postural drainage

2. Antibiotic �The choice of antibiotics should be accurately by the results of sputum culture and drug sensitivity test. � Empirical therapy --- antipseudomonal antibiotics.

ANTIBIOTICSARETHECORNERSTONEOF BRONCHIECTASIS MANAGEMENT � Antibiotics are used only during acute episodes � Choice of an antibiotic should be guided by gram's stain and culture of sputum � Empiric coverage (amoxicillin, cotrimoxazole, levofloxacin) is often given initially

BRONCHODILATER � Bronchodilators to improve obstruction and aid clearance of secretions are useful in patients with airway hyperreactivity and reversible airflow obstruction

� Surgical management is indicated 1. Recurrent and refractory clinical symptoms are due to a focal area of disease involvement. 2. Massive hemoptysis � Management of hemoptysis

� Surgical resection Bronchialarterialembozil ato in �� �� Althoughresectionmaybesuccessfulif disease is localized, embolizationis preferablewith widespreaddisease

NURSING MANAGEMENT: �History �Obtain and physical examination history regarding amount and characteristics of sputum produced, including haemoptysis. �Auscultate lungs for diffuse rhonchi and crackles.

NURSING DIAGNOSIS �Ineffective Airway Clearance related to tenacious and copious secretions
- Slides: 38