Briefly describe a recent frustrating or difficult case

Briefly describe a recent frustrating or difficult case

Patient-Centered Care Plans: How Reframing the Complicated to the Complex Creates a Key Patient-Centered Tool

Dan Eubank MD Lora Council MD Bill Gunn Ph. D NH-Dartmouth Family Medicine Residency Concord Hospital Family Health Centers Concord Hospital May 1, 2008

Complicated to Complex: Rethinking our Clinical Paradigm

What do we mean by complex instead of complicated? Recipes Rockets Children Formula Essential Critical Limited Prediction High Some Expertise Helps Essential Contributes Reproduce Results Outcome Certainty Standard High Unique High Always remains uncertain

Degree of Engagement Low Complex Chaotic Scan for patterns Good enough planning-minimum specifications, simple rules Multiple actions Experiment and tune system Listen to the shadow system Use intuition, muddle through Chunking Plan and Control Metaphors Regulate Wicked questions Mechanical High (Simple, Complicated) High Low Degree of certainty

Characteristics of Complexity • • Agents acting based on internal rules Uncertainty & unpredictability Interrelationships key Purposeful and adaptive – agents & system Emerging novel behavior via interactions Porous boundaries – nested, agents come & go Self organize with discernable patterns, attractors, & local rules • Tension & paradox natural

Recognizing a complex situation: How do you know you are in a complex situation? – Too many elements to understand by direct observation- requires multiple perspectives – An issue that technique can’t analyze adequately – No direct solution – requires multiple interventions and time to see how they do – So multifaceted that any action has unanticipated consequences – Conflicting assumptions or values

Recognizing a complex situation: When the dynamics of a patient’s problems begin to feel: - neglected - “dissected” into multiple discrete problems (ignoring important interrelationships) - the issues are addressed, but laboriously and inefficiently

Recognizing a complex situation: • You’re fighting back feelings of: – Frustration – Anger – Fear – Failure – Rejection – Hopelessness – Blame

What makes generalism complex? • • • Person centered Need for change and growth Involves relationships Delivered in Organizations Context – conflicting cultural values Chronic illness
 ACUTE / 2) STRAIGHTFORWARD 2)")
The Quadrant Model-Plus STRAIGHTFORWARD COMPLICATED A C U 1) ACUTE / 2) STRAIGHTFORWARD 2) ACUTE / COMPLICATED 3) CHRONIC / STRAIGHTFORWARD 4) CHRONIC / COMPLICATED T E C H R O N I C

What does complexity imply? • New paradigm – Hero/expert/mechanical- Learner/coach/ complexity • New interventions – Muddling, chunking, teaching, experiment, minimum specification, metaphors, provocative questions, remove barriers • New problems – Motivation, resilience, integration, learning, meaning

What does complexity imply? • New processes – Teams, care management, education, organization development, integration • New skills – Coaching, creating holding relationships, influence, conflict management, narrative analysis, self awareness and reflection, collaboration

How does complexity play a part in care of chronic illness? • • Role Process Ideal Care Plans

Generalist’s Role • Committed to acquiring the best knowledge available and applying it to the benefit of individual persons in their care rather than to the aims of science or technology. – Prevent and alleviate suffering – Help people understand their vulnerabilities – Help them change what they can – Help them transcend what they can’t change
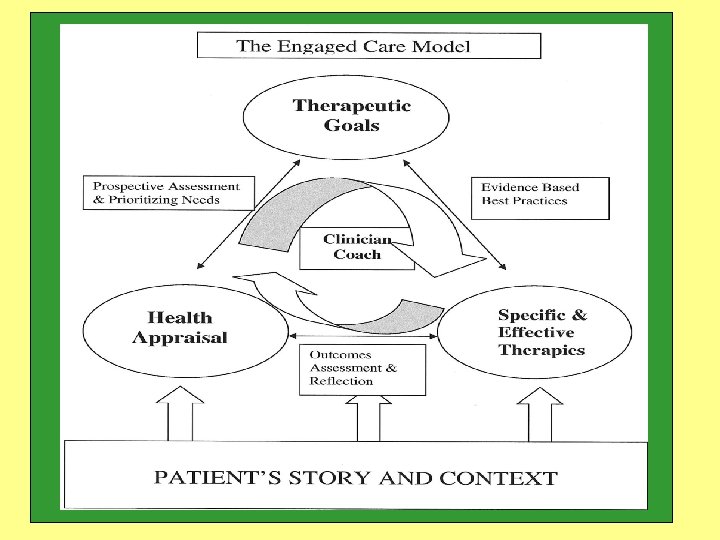

Aligning the Care Team to Address Complexity • Patient clearly articulates goals • Goals help focus a coherent dialogue with patients and team • Goals help manage the complexity of practice • Care in a longitudinal, goal-directed experience engages patients and creates learning for resilience

The Medical Home • A care team • A place of coming together for people who care for each other • A place where we as people are understood, a place that can garner the resources to address the challenges of life. • A home base to work from in a dynamic world • A place of respite when things are difficult and confusing • A place to grow and learn

Care Plans • Become central, but need to: – Reflect complexity – Integrate relationships – Be patient driven – Reflect the learning process – Communicate the individual – Be current

Characteristics of Complexity • • Agents acting based on internal rules Uncertainty & unpredictability Interrelationships key Purposeful and adaptive – agents & system Emerging novel behavior via interactions Porous boundaries – nested, agents come & go Self organize with discernable patterns, attractors, & local rules • Tension & paradox natural

What interventions help deal with complexity? Image from http: //www. cs. iastate. edu/~honavar/ELEGANT. GIF

Complicated systems use “tools”
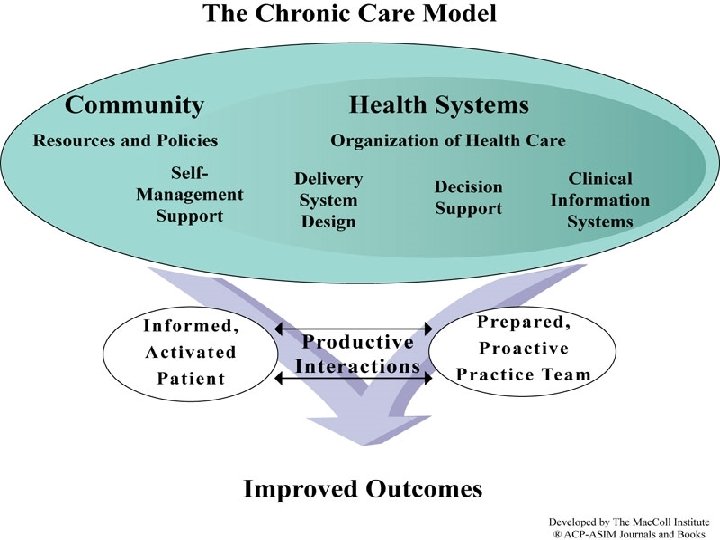

“If we educate clinic teams and train them in the chronic care model in clinics, we will see implementation of the chronic care model resulting in appropriate treatment for patients with high blood pressure. ” http: //cdc. gov/DHDSP/state_program/evaluation_guides/logic_model. htm, accessed 4/15/08

The Patient Centered Medical Home is Complex Patient centered care address patients’ Needs Wants Values are Complex Values change and can conflict Values are influenced by relationships Values guide choices and actions that may not be predictable or logical

The Patient Centered Medical Home is Complex • The medical home is a system of care allowing: – Continuity – Comprehensiveness – Teamwork – Whole person orientation – Coordinated care

If the Patient Centered Medical Home is complex, then – CANNOT be ‘installed’ using a set of tools. – CAN be adapted for patients by reframing the care system to address needs, wants and values in the context of the medical home principles.

Care Plans Help Address Complexity Values Relationships Team Goal-based

Care Plans need to: – Reflect complexity – Integrate relationships – Be patient driven – Reflect the learning process – Communicate the individual – Be current

Care Plans help with Complexity • Traditional care plans tend to be Disease-based Mechanistic Protocol driven Multi-disciplinary • Care plan that address complexity Situation-based Adaptive Values driven Interdisciplinary

Nickname Physical Address Can we leave Messages? Contacts PERSONAL Written Releas COORDINATED Do they have Appointment? Who is on the team? TEAM

PERSONAL Snapshot WHOLE PERSON APPROACH PATIENT CENTERED COMPREHENSIVE Priorities

Situation Motivational Interviewing Goals Measure Importance &

s s e i it l i ib s on p es p e t S R Ti f e m ra

Problem Plan

Joan’s Story

Care Plan Improvement Team Medical Assistant Clinical Nurse Team Leader Health Center Nurse Manager Geriatric Nurse Pediatric Nurse Care Manager Behavioral Health Coordinator Community Resource Coordinator Pediatrician Faculty Family Medicine Faculty Behavioral Health Faculty Family Medicine Resident Preventive Medicine Resident Patient Registrar

Changing a Culture • • Representation from all stakeholders Develop a Common Aim Clear leadership – organized meetings Flexibility of leadership to adapt to the group Creativity gains buy in of the clinic Look for early adopters – providing reinforcement Persistence, Persistence

Complex Continuity Clinic • Method for promoting care plans – furthering culture change • Third year residents – working with their team – multidisciplinary preceptors • Longer medical visits – goal-oriented focus • Patients selected by resident or team – individualized plans for patient – individualized themes for residents

Skill Areas • • Self-Reflection Patient Centered Interviewing Goal Oriented Interviews Care plan development Influence Skills Negotiation Skills Team Based Skills of delegation and collaboration
. \"Improving primary care for")
References Bodenheimer, T. , E. H. Wagner, et al. (2002). "Improving primary care for patients with chronic illness. " Jama 288(14): 1775 -9. Bodenheimer, T. , E. H. Wagner, et al. (2002). "Improving primary care for patients with chronic illness: the chronic care model, Part 2. " Jama 288(15): 1909 -14. Delbanco, T. (2006). "Sharing everything we write with our patients: will fully transparent electronic medical records make or break the future? " Med. Gen. Med 8(2): 1. Flocke, S. A. , W. L. Miller, et al. (2002). "Relationships between physician practice style, patient satisfaction, and attributes of primary care. " J Fam Pract 51(10): 835 -40. Fraser, S. W. and T. Greenhalgh (2001). "Coping with complexity: educating for capability. " Bmj 323(7316): 799803. Greenhalgh, T. , A. Collard, et al. (2005). "Sharing stories: complex intervention for diabetes education in minority ethnic groups who do not speak English. " Bmj 330(7492): 628. Greenhalgh, T. , G. Robert, et al. (2004). "Diffusion of innovations in service organizations: systematic review and recommendations. " Milbank Q 82(4): 581 -629. Hettema, J. Steele, et al. (2005). "Motivational interviewing. " Annu Rev Clin Psychol 1: 91 -111. Matlow, A. G. , J. G. Wright, et al. (2006). "How can the principles of complexity science be applied to improve the coordination of care for complex pediatric patients? " Qual Saf Health Care 15(2): 85 -8. Miller, C. E. and J. L. Johnson (2001). "Motivational interviewing. " Can Nurse 97(7): 32 -3. Miller, W. L. and B. F. Crabtree (2005). "Healing landscapes: patients, relationships, and creating optimal healing places. " J Altern Complement Med 11 Suppl 1: S 41 -9. Miller, W. L. , B. F. Crabtree, et al. (1998). "Understanding change in primary care practice using complexity theory. " J Fam Pract 46(5): 369 -76. Miller, W. L. , R. R. Mc. Daniel, Jr. , et al. (2001). "Practice jazz: understanding variation in family practices using complexity science. " J Fam Pract 50(10): 872 -8.
. \"New knowledge for")
References Miller, W. L. , W. R. Phillips, et al. (2005). "New knowledge for and about primary care: a view through the looking glass of the Annals of Family Medicine. " Ann Fam Med 3(3): 197. Plsek, P. E. and T. Greenhalgh (2001). "Complexity science: The challenge of complexity in health care. " Bmj 323(7313): 625 -8. Sia, C. , T. F. Tonniges, et al. (2004). "History of the medical home concept. " Pediatrics 113(5 Suppl): 1473 -8. Starfield, B. (2001). "New paradigms for quality in primary care. " Br J Gen Pract 51(465): 303 -9. Stroebel, C. K. , R. R. Mc. Daniel, Jr. , et al. (2005). "How complexity science can inform a reflective process for improvement in primary care practices. " Jt Comm J Qual Patient Saf 31(8): 438 -46. Sussman, A. L. , R. L. Williams, et al. (2006). "The art and complexity of primary care clinicians' preventive counseling decisions: obesity as a case study. " Ann Fam Med 4(4): 327 -33. Tallia, A. F. , K. C. Stange, et al. (2003). "Understanding organizational designs of primary care practices. " J Healthc Manag 48(1): 45 -59; discussion 60 -1. Wagner, E. H. , R. E. Glasgow, et al. (2001). "Quality improvement in chronic illness care: a collaborative approach. " Jt Comm J Qual Improv 27(2): 63 -80. Wilson, T. Holt, et al. (2001). "Complexity science: complexity and clinical care. " Bmj 323(7314): 685 -8. Zimmerman, B. (1999). "Complexity science: a route through hard times and uncertainty. " Health Forum J 42(2): 42 -6, 69.
- Slides: 44