Brief Intervention and Referral to Treatment EMERGENCY MEDICINE

Brief Intervention and Referral to Treatment EMERGENCY MEDICINE

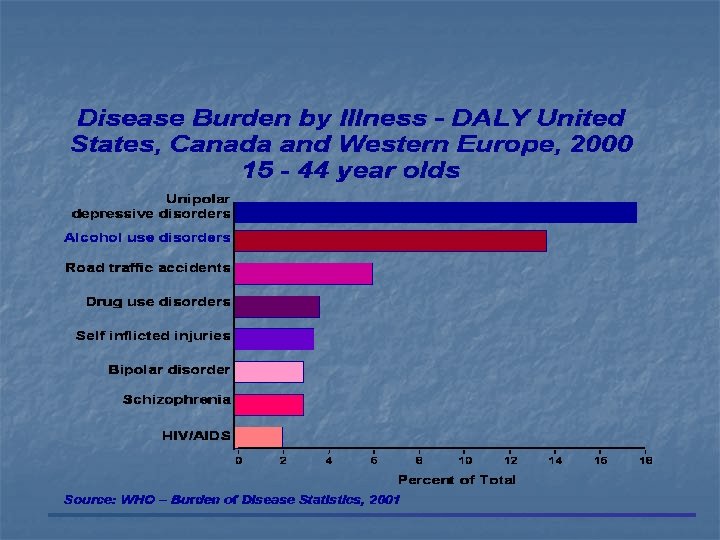
Morbidity and Mortality n >107, 000 alcohol related deaths each year n 1/3 of adult hospital admissions are alcohol related n Attributable risk factor for multiple illnesses n n Major risk factor for all categories of injury n Problem drinkers have 2 x injury events/yr and 4 x as many hospitalizations for injury n A single alcohol-related visit predicts continued problem drinking Social and family issues

Alcohol Related Injuries n n 150, 000 injury deaths in U. S. each year several hundred thousand disabling injuries per year 15 -34 years olds at highest risk alcohol use involved in large proportion of deaths and injuries

Alcohol Related Costs n n Medical treatment, insurance, unemployment, lack of productivity Families with an alcoholic member have twice the average monthly health care bill than other families

Alcohol Related Casualties n n n Under reported on death certificates Under reported on hospital discharge Selection and recording bias

Alcohol-Related Fatalities in MVCs Source: FARS

BAC Levels for Alcohol Positive Drivers Involved in Alcohol-Related Fatal Crashes. 16 = Median and Mode BAC Source: 2002 ARF FARS

Drinking Patterns in the U. S. Abstain 40% At Risk or Problem 20% Dependent 5% Low Risk 35% Source: National Longitudinal Alcohol Epidemiologic Survey, 1992
 MODERATE (20%) at risk drinkers SEVERE")
Prevention and Intervention ABSTAINERS & MILD DRINKERS (70%) MODERATE (20%) at risk drinkers SEVERE (10%) Specialized Treatment Brief Intervention Primary Prevention

Alcohol Terminology n Hazardous drinking - at-risk drinking n n Harmful drinking n n NIAAA definition Health consequences Binge drinking n 5 or more drinks per drinking episode

Alcohol Terminology n n Dependence - cluster of symptoms including impaired control over intake, withdrawal symptoms, tolerance, drinking despite problems Abuse - repetitive patterns of drinking in harmful situations with adverse consequences, including impaired ability to fulfill responsibilities or negative effects on social/interpersonal functioning and health

Issues related to lack of exploration of alcohol use n n n Lack of understanding of problem Failure to acknowledge responsibility for identification/intervention Biases - personal/professional Feeling that nothing can be done Not knowing what can be done Outside of what is thought to be the traditional realm of medical care providers

Issues Related to ED Provider Screening for Alcohol Use n n Alcohol screening not traditionally part of physician job Not comfortable with alcohol related issues Don’t know how to intervene Frustration over prior experiences with patients who abuse alcohol

Alcohol Use as Part of the Medical History n n n Alcohol use Quantity Frequency Type of alcohol used Problems related to alcohol use

Alcohol Screening - Issues n n Not seen as responsibility of physician in ED Included as part of “social” history Providers not educated concerning importance of alcohol screening as routine practice Providers not educated concerning how to ask the questions

Alcohol Interventions n n n Brief intervention Further evaluation and more extensive intervention for person with more significant problem Provider intervention may be more effective

Social Morays

A Standard Drink A standard drink is 12 grams of pure alcohol or: • • • One 12 -ounce bottle of beer or wine cooler One 5 -ounce glass of wine 1. 5 ounces of distilled spirits

Screen Positive Drinks per week Drinks per occasion Men > 14 >4 Women >7 >3 All Age >65 >7 >1

Drinking Patterns: Rates and Risks Binge Drinking The National Advisory Council on Alcohol Abuse and Alcoholism has recommended the following definition of “Binge Drinking”: n n A “binge” is a pattern of drinking alcohol that brings blood alcohol concentration (BAC) to 0. 08 gm% or above. For the typical adult, this pattern corresponds to consuming 5 or more drinks (male) or 4 or more drinks (female) in about 2 hours. Binge drinking is clearly dangerous for the drinker and for society
 n Single or repeated sessions")
Brief Intervention n Short counseling sessions (5 -45 minutes) n Single or repeated sessions n Performed by non-addiction specialists n Contain advice and/or motivational enhancement

Brief Intervention n n At risk/problem drinkers n Advise to cut down n Set goals n Provide Primary Care follow-up Dependence n Advise to abstain n Refer to treatment

Advise: What? n ABSTAIN n n n pregnant or considering medication that interacts dependence failed attempts to cut down contraindicated medical condition n CUT DOWN n n n drinking above low risk amounts no dependence no problems

Stages of Change Model Pre-Contemplation Mai Preparation ntenance Action Prochaska & Di. Clemente, 1986

General Principles for Negotiating Behavior Change n n n Respect for autonomy of patients and their choices Readiness to change must be taken into account Ambivalence is common Targets selected by the patient, not the expert Expert is the provider of the information Patient is the active decision-maker Rollnick, 1994
- Slides: 27