Breastfeeding Public Health 2009 Functions of Public Health

Breastfeeding & Public Health 2009

Functions of Public Health • Assessment • Policy Development • Assurance

Levels of Influence in the Social-Ecological Model Structures, Policies, Systems Local, state, federal policies and laws to regulate/support healthy actions Institutions Rules, regulations, policies & informal structures Community Social Networks, Norms, Standards Interpersonal Family, peers, social networks, associations Individual Knowledge, attitudes, beliefs

Objectives Students will be able to: • Identify advantages to increasing breastfeeding rates in the population • List 2010 Healthy People goals for breastfeeding • Access population-based breastfeeding data and describe patterns of breastfeeding in the US • Apply evidence-based approaches to improve breastfeeding rates • Use knowledge about the physiology of breastfeeding to advocate for policies that support breastfeeding

Benefits of Breastfeeding • Health outcomes – Infant – short term – Infant – long term – Maternal • Economic • Environmental

Breastfeeding and the Use of Human Milk American Academy of Pediatrics, 2005 • “Human milk is species-specific, and all substitute feeding preparations differ markedly from it, making human milk uniquely superior for infant feeding. ”

Health Benefits for Infant: AAP • Lowered risk of infectious diseases in both developed and developing countries: diarrhea, respiratory tract infection, otitis media, bacterial meningitis, botulism, UTI, necrotizing enterocolitis, bacteremia • Enhanced immune response to polio, tetanus, diptheria, haemophilus influenza immunization • Possible lowered risk of sudden infant death syndrome • Possible lowered risk of diabetes (type 1 & 2), leukemia, Hodgkin disease, lymphoma • Probable enhanced cognitive development • Provides analgesia to infants during painful procedures

Health Benefits for Mother: AAP • Possible reduction in hip fractures after menopause • Less postpartum bleeding & more rapid uterine involution • Reduced risk of breast and uterine cancer • Increased child spacing

Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries (Agency for Healthcare Research and Quality, 2007) • Systematic reviews/meta-analyses, randomized and non-randomized comparative trials, prospective cohort, and case-control studies on the effects of breastfeeding • English language • Studies must have a comparative arm of formula feeding or different durations of breastfeeding. Only studies conducted in developed countries were included in the updates of previous systematic reviews. • Studies graded for methodological quality.

Limitations of Breastfeeding Outcome Studies • Definitions of breastfeeding; misclassification • Lack of randomization; confounding & residual confounding • “Wide range in quality of evidence”

AHRQ: Positive Findings for Infants % less in BF Acute otitis media (exclusive BF 3 -6 mos. ) 50% Atopic dermatitis (exclusive BF 3 mos) 42% GI infection (infants breastfeeding) 64% Lower respiratory tract diseases Asthma (in young children) – no family hx, family hx Obesity Type I diabetes Type 2 diabetes Childhood leukemia Sudden Infant Death Syndrome Necrotizing enterocolitis 72% 27%, 40% 4, 7, 24% 19, 27% 39% 15, 19% 36% 4 -82%

AHRQ: Equivocal or insignificant infant outcomes • Cognitive development in term or preterm infants • CVD • Infant mortality in developed countries

AHRQ: Positive Maternal Outcomes % less in BF Maternal Type II Diabetes (reduction in risk per 4, 12% year of lactation) Postpartum depression Breast cancer (reduction per year of lactation) Ovarian cancer association 4. 3, 28% 21%

AHRQ: Equivocal or insignificant maternal outcomes • Effect of breastfeeding in mothers on return-to-pregnancy weight was negligible • Effect of breastfeeding on postpartum weight loss was unclear • Little or no evidence for association with osteoporosis

Breastfeeding and Obesity: Reviews & Meta-analysis • Owen et al. Pediatrics. 2005 – 61 studies – Odds ratio = 0. 87 (95% CI 0. 85 -0. 89) for reduced risk of later obesity associated with breastfeeding compared to formula • Arenz et al. Int J obes relat metab disord. 2004 – 9 studies met criteria – Odds Ratio = 0. 78, 95% CI (0. 71, 0. 85) protective effect of breastfeeding for obesity – Found dose response • Harder et al. Am J Epidemiol. 2005

Breastfeeding and risk of obesity Does Breastfeeding Reduce the Risk of Pediatric Overweight? CDC. 2007
 Length of Odds Ratio for")
Harder et al. Am J Epidemiol. 2005 (17 studies) Length of Odds Ratio for 95% CI Breastfeeding Risk of Obesity < 1 1. 00 0. 65, 1. 55 1 -3 0. 81 0. 74, 0. 88 4 -6 0. 76 0. 67, 0. 86 7 -9 0. 67 0. 55, 0. 82 Ø 9 0. 68 0. 50, 0. 91

Breastfeeding & Obesity: Support for the Evidence • Secular trends – Trend for increased breastfeeding is opposite that for obesity • Dose Response – Some studies find, others do not • Plausible mechanisms – – Changes in leptin production and sensitivity Lower energy and protein intake in breastfed infants Insulin response to feeding; higher in formula fed infants Differences in the feeding relationship; self-regulation of energy intake – Changing composition of human milk during feedings

Dubois et al. Public Health Nutrition, 2003 • Social inequalities in infant feeding during the first year of life. The Longitudinal Study of Child Development in Quebec (LSCDQ 1998 -2002) • “Social disparities in diet during infancy could play a role in the development of social and health inequalities more broadly observed at the population level. ”
 • Families: ~$2, 000 for the")
Economic Costs of Formula Feeding (US Breastfeeding Committee) • Families: ~$2, 000 for the first year • Employers: loss of productivity, increased absence, more health claims • Health care: 3. 6 billion a year to treat infant illnesses, $331 -475 per child for one HMO • Food assistance: costs to support breastfeeding mothers in WIC are 55% the cost for providing formula
 • Human milk is a renewable")
Environmental Benefits of Breastfeeding (ADA Position Paper, 2005) • Human milk is a renewable natural resource. • Produced and delivered to the consumer directly • Formula requires manufacturing, packaging, shipping, disposing of containers – 550 million formula cans in landfills each year* – 110 billion BTUs of energy to process and transport* • Breastfeeding delays return of menses, increases birth spacing, limits population growth *USBC
 • Individual: Inadequate knowledge, embarrassment, social reticence,")
Barriers to Breastfeeding (ADA Position Paper 2005) • Individual: Inadequate knowledge, embarrassment, social reticence, negative perceptions • Interpersonal: Lack of support from partner and family, perceived threat to father-child bond • Institutional: Return to work or school, lack of workplace facilities, unsupportive health care environments • Community: discomfort about nursing in public • Policy: aggressive marketing by formula companies

2007 Health Styles Survey Neither Agree/Disa gree Question Agree Disagree Mothers who breastfeed should do so in private places only. 35. 8% 26. 0% 38. 2% I am comfortable when mothers breastfeed their babies near me in a public place, such as a shopping center, bus station, etc. 44. 1% 24. 6% 31. 3% I believe women should have the right to breastfeed in public places. 52. 0% 23. 8% 24. 2% Infant formula is as good as breast milk. 20. 2% 27. 2% 52. 6%

Moses Lake Breastfeeding Data
 Statements about the Community % Agree %")
Moses Lake Resident Survey (N = 254) Statements about the Community % Agree % Disagree Babies in our community are more likely to be bottle-fed first 6 months 55. 1% 28. 3% It is not customary to breastfeed a baby in public 61. 0% 26. 4% Brzezney A. Unpublished Data (2003)
 Statements about Worksites % Agree % Disagree")
Moses Lake Resident Survey (N = 254) Statements about Worksites % Agree % Disagree Workplaces in our community make it easier for mother to bottle-feed 61. 4% 21. 3% Workplaces in our community make it easier for mother to breastfeed 8. 7% 67. 3% (Barrier) Mothers don’t want to breastfeed…mothers must return to work 87. 8% 3. 5% Brzezney A. Unpublished Data (2003)
 Statements about Childcare % Agree % Disagree")
Moses Lake Resident Survey (N = 254) Statements about Childcare % Agree % Disagree (Barrier) Mothers don’t want to breastfeed…baby starts attending day care 71. 7% 14. 2% Brzezney A. Unpublished Data (2003)

Assessment Rates of Breastfeeding and Exclusive Breastfeeding

Percent of U. S. children who were breastfed, by birth year Breastfeeding Among U. S. Children Born 1999— 2006, CDC National Immunization Survey

Exclusive Breastfeeding

Percent of U. S. breastfed children who are supplemented with infant formula, by birth year 1

Percent of U. S. Breastfed infants who are supplemented with infant formula 2003 Before 2 days 2004 2005 2006 22. 3± 1. 6 23. 5± 1. 0 24. 9± 1. 1 25. 6± 1. 4 Before 3 months 38. 1± 2. 2 37. 4± 1. 3 38. 1± 1. 4 37. 9± 1. 7 Before 6 months 47. 4± 2. 6 45. 9± 1. 7 44. 7± 2. 0 44. 5± 1.

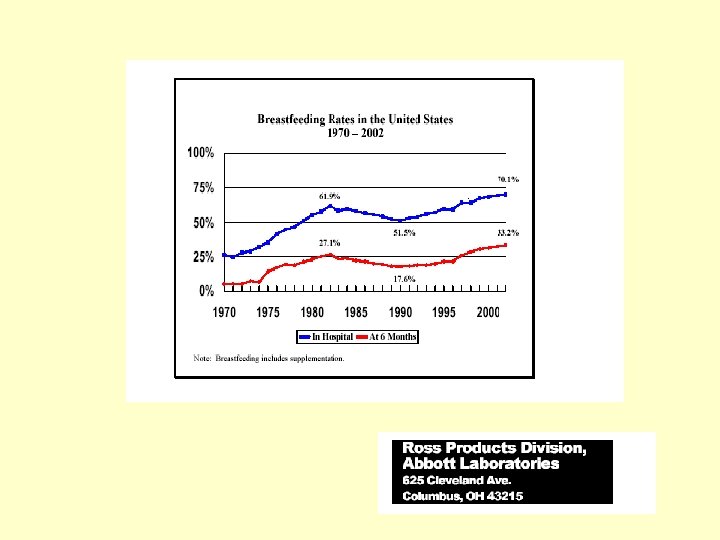
The resurgence of breastfeeding at the end of the second millennium (Wright and Schanler, J Nutr. 131, 2001) • Between 1971 and 1995 increase was for all groups. • Between 1984 and 1995 increase was in groups less likely to breastfeed (low income, low education, African American, WIC) • Early resurgence of breastfeeding concurrent to “natural childbirth” and women’s movement in white well educated families

More recent increases associated with: • Increased knowledge of the benefits of breastfeeding by professionals (AAP 1997) • Successful breastfeeding interventions - especially in WIC – 47% of US infants on WIC – early 90 s brought increased WIC & for breastfeeding promotion and increased maternal food package for BF

Healthy People Goals and Breastfeeding Data

National Immunization Survey • Random-digit--dialed telephone survey conducted annually by CDC • Nationally representative data • Breastfeeding questions first added in 2001 • Data organized by birth cohort, not year of data gathering • 2004 data from 17, 654 infants

Healthy People 2010: Increase the proportion of mothers who breastfeed their babies Goal Early postpartum At 6 months 75% US Baseline 64% US 2004 WA 2005 74% 88% 90% 50% 25% 42% 57% At one year 25% 16% 21% 32% 33%

Healthy People 2010: Increase the proportion of mothers who breastfeed their babies Goal Early post 75% -partum US Baseline 64% US 2004 WA 2005 WA 2006 74% 88% 90% 86% At 6 months 50% 25% 42% 57% 58% At one year 25% 16% 21% 32% 33% 35%

Does Breastfeeding Reduce the Risk of Pediatric Overweight? CDC. 2007
")
Demographics of Breastfeeding (NIS 2004)

2004 Percent of Children Ever Breastfed by State among Children Born 2005 2006

Percent of Children Breastfed at 6 Months of Age by State 2004 2006 National Immunization Survey, Centers for Disease Control and Prevention, Department of Health and Human Services

Percent of Children Breastfed at 12 Months of Age by State 2004 2006 National Immunization Survey, Centers for Disease Control and Prevention, Department of Health and Human Services

New 2010 Breastfeeding Objectives added in 2007 • To increase the proportion of mothers who exclusively breastfeed their infants through age 3 months to 60% • To increase the proportion of mothers who exclusively breastfeed their infants through age 6 months to 25%

Exclusive breastfeeding: definition • Exclusive breastfeeding is defined as an infant receiving only breast milk and no other liquids or solids except for drops or syrups consisting of vitamins, minerals, or medicines

Exclusive Breastfeeding Thro ugh 3 mont hs Thro ugh 6 mont hs US 2004 US 2005 US 2006 WA 2004 WA 2005 WA 2006 31 36 33 50 45 49 11 12 14 23 21 25
 Maternal Education Less than high")
Rates of Exclusive Breastfeeding at 3 months (NIS, 2004) Maternal Education Less than high school High school Some college College graduate Income/poverty ratio < 100 - 184 185 - 340 >350 % 24 23 33 42 24 29 34 39
 Education Hispanic White, non-Hispanic Black,")
Rates of Exclusive Breastfeeding at 3 months (NIS, 2004) Education Hispanic White, non-Hispanic Black, non-Hispanic Asian, non-Hispanic Other Mother’s age at birth of child < 20 20 -29 > 30 % 31 33 20 31 17 26 35

Percent of Children Exclusively Breastfed Through 3 Months of Age among Children born in 2004 National Immunization Survey, Centers for Disease Control and Prevention, Department of Health and Human Services

Percent of Children Exclusively Breastfed Through 3 Months of Age among Children born in 2005 (Provisional)

Percent of Children Exclusively Breastfed Through 6 Months of Age among Children Born in 2004 National Immunization Survey, Centers for Disease Control and Prevention, Department of Health and Human Services

Percent of Children Exclusively Breastfed Through 6 Months of Age among Children Born in 2005

Healthy People 2010 Objectives # of States Meeting Objective, children born 2006 75% of mothers initiating breastfeeding 28 50% of mothers breastfeeding their infant at 6 months of age 13 25% of mothers breastfeeding their infant at 12 months of age 20 40% of mothers exclusively breastfeeding their infant through 3 months of age 13 17% of mothers exclusively breastfeeding their infant through 6 months of age 13

Assurance: Evidence-Based Interventions The CDC Guide to Breastfeeding Interventions, 2005

Six evidence-based interventions • Individual: – Educating mothers – Professional support • Intrapersonal: – Peer support/counseling programs • Institutional – Maternity care practices • Media and social marketing

Four Interventions: Effectiveness not established, encourage rigorous evaluation 1. Use contermarketing techniques to limit the negative impact of formula marketing 2. Improve the knowledge, skills and attitudes of health care providers re breastfeeding 3. Increase public acceptance of breastfeeding 4. Provide assistance to breastfeeding mothers through hotlines or other information sources

Policies to Support Breastfeeding Key policy documents Worksites Healthcare Legislation

Breastfeeding Policy Documents 1984 U. S. Surgeon General’s Workshop 1990 Innocenti Declaration, WHO and UNICEF 2000 Healthy People 2010: Objectives 2000 HHS Blueprint for Action on Breastfeeding 2001 US Breastfeeding Committee Strategic Plan 2003 WHO: Global Strategy for Infant and Young Child Feeding 2003 WA State Nutrition & Physical Activity Plan

Key Policy Documents: Worksites Global Strategy for Infant & Young Child Feeding Innocenti Declaration WHO/ UNICEF (1990) WHO/ UNICEF (2003) “Women in paid employment “…obstacles to breastfeeding can be helped to continue within the…workplace… breastfeeding by bring must be eliminated…” provided with minimal enabling conditions. paid maternity leave, part- time work arrangements, onsite crèches, facilities for expressing and storing breastmilk and breastfeeding breaks. ”

HHS Blueprint: Worksites 1. “Facilitate breastfeeding or breastmilk expression at the workplace by providing private rooms, commercial grade breastpumps, milk storage arrangements, adequate breaks during the day, flexible work schedules and onsite childcare facilities. ” 2. “Establish family and community programs that enable breastfeeding continuation when women return to work in all possible settings. ” 3. “Encourage childcare facilities to provide quality breastfeeding support. ”
 Agree Neither Disagree/ Disagree")
CDC Healthstyle Survey – 2006 (Nationally representative postal survey N~5000) Agree Neither Disagree/ Disagree I believe employers should provide flexible work schedules, such as additional break time, for breastfeeding mothers 51 32 18 I believe employers should provide extended maternity leave to make it easier for mothers to breastfeed. 49 31 19

Healthstyle Survey, cont. Agree Neither agree/ Disagree I believe employers should provide a private room for breastfeeding mothers to pump their milk at work. 47 29 24 I would support tax incentives for employers who make special accommodations to make it easier for mothers to breastfeed. 30 34 36

WA Healthy Worksite Survey • Content: Measures policies, & environments to support healthy nutrition, physical activity, breastfeeding and to discourage tobacco use. • Population: WA businesses with 50+ employees, selected from WA Department of Employment Security. • Sampling: Representative geographic sample across WA. 900 contacted, 540 responded. • Administration: Fall 2005. 15 minute phone survey of HR managers, conducted by Gilmore. Repeat in 2007. • Background: DOH STEPS/CDNPA/Tobacco collaboration

Of the 400 Businesses with Female Employees < age of 50: • 11% had a specific policy to support breastfeeding • 82% provided flexible scheduling to allow employees adequate break time to breastfeed or pump/express breast milk • 31% had a designated room or location (not counting bathroom stalls) for mothers to breastfeed or pump/express breast milk

Characteristics of Breastfeeding Rooms

Key Policy Documents: Childcare HHS Blueprint for Action WA State Nutrition & Physical Activity Plan (2000) (2003) • Safe storage • Follow mothers’ instructions • Provide quiet and comfortable place for mothers • “Assure that…child care facilities are breastfeeding friendly. ” • Follow guidelines of Breastfeeding coalition of Washington.

Key Policy Documents: Health Care Global Strategy for Infant & Young Child Feeding WA State Nutrition & Physical Activity Plan WHO/ UNICEF (2003) “Virtually all mothers can • Support King County breastfeed provided they have model breastfeeding accurate information, and standards. support within their families and communities and from the health care system. They should also have access to skilled practical help from, for example, trained health workers, lay and peer counselors, and certified lactation consultants…”

Key Policy Documents: Health Care International Code of Marketing of Breastmilk Substitutes Innocenti Declaration WHO/ UNICEF(1990) WHO (1981) “No facility of a health care system should be used for the purpose of promoting infant formula or other products…” “…obstacles to breastfeeding within the…health system…must be eliminated…” “Health workers should encourage and protect breastfeeding…” “…every facility providing maternity services fully practices all ten of the Ten Steps to Successful Breastfeeding…”

HHS Blueprint: Health Care System 1. Train health care providers who provide maternal and child care on the basics of lactation, breastfeeding counseling and lactation management during coursework, clinical and in-service training and continuing education. ” 2. Ensure that breastfeeding mothers have access to comprehensive, up-to-date, and culturally tailored lactation services provided by trained physicians, nurses, lactation consultants and nutritionists/dietitians.

Health Care System, cont. 3. Establish hospital and maternity center practices that promote breastfeeding, such as the “Ten Steps to Successful Breastfeeding. ” 4. Develop breastfeeding education for women, their partners, and other significant family members during the prenatal and postnatal visits.
 •")
National Survey of Maternity Care Practices in Infant Nutrition and Care (m. PINC) • 2, 546 hospitals, 121 birth centers in the 50 states, DC, Puerto Rico • 35 questions; 7 categories – – – labor and delivery, breastfeeding assistance, mother-newborn contact, newborn feeding practices, breastfeeding support after discharge, nurse/birth attendant breastfeeding training and education, – structural and organizational factors related to breastfeeding MMWR. June 13, 2008 / 57(23); 621 -625

http: //www. cdc. gov/mmwr/preview/mmwrhtml/mm 5723 a 1. htm#fig

m. PINC: Key Findings • 70% of facilities reported providing discharge packs containing infant formula samples to breastfeeding mothers • 88% of facilities taught the majority of mothers techniques related to breastfeeding • 24% of facilities reported giving supplements (and not breast milk exclusively) as a general practice with more than half of all healthy, fullterm breastfeeding newborns MMWR. June 13, 2008 / 57(23); 621 -625

State Breastfeeding Legislation • Breastfeeding in public: 23 states give the right to breastfeed in any place it is legal to be • Jury duty: 7 states exempt breastfeeding mothers from jury duty • Family law: three states require breastfeeding status to be considered in divorce or custody decisions.

WA Breastfeeding Legislation 1. Amendment to indecent exposure law – “A person is guilty of indecent exposure if he or she intentionally makes any open and obscene exposure of his or her person or the person of another knowing that such conduce is likely to cause reasonable affront or alarm. The act of breastfeeding or expressing breast milk is not indecent exposure. ”

WA breastfeeding legislation • “Am employer may use the designation “ infant friendly” on its promotional materials if the employer has an approved workplace breastfeeding policy addressing at least the following: – Flexible work schedule, place to nurse/express with handwashing facilities and refrigerator • DOH to approve employers, but no funds to do this, so no worksites have been designated

HB 1596 - 2009 • An act relating to protecting a woman’s right to breastfeed in a place of public resort, accommodation, assemblage, or amusement; amending RCW 49. 60. 030 and 49. 60. 215. • Adds breastfeeding to rights protecting discrimination because or race, creed, color, national origin, sex, honorably discharged veteran, sexual orientation or the presence of…. disability. .

CDC Breastfeeding Report Card 2009 – Process Indicators US WA Percent of live births occurring at facilities designated as Baby Friendly (BFHI) 2. 87 6. 85 Number of IBCLCs ** per 1000 live births 2. 20 4. 16 80 1. 4 Number of state health dept FTEs dedicated to breastfeeding

CDC Report Card, cont. US WA State legislation about breastfeeding in public places 46 yes State legislation mandating employer support 15 no Presence of an active statewide breastfeeding coalition 41 yes

Levels of Influence in the Social-Ecological Model Structures, Policies, Systems Local, state, federal policies and laws to regulate/support healthy actions Institutions Rules, regulations, policies & informal structures Community Social Networks, Norms, Standards Interpersonal Family, peers, social networks, associations Individual Knowledge, attitudes, beliefs
- Slides: 81