Brain Injury 101 Brain Injury in the Criminal

Brain Injury 101 Brain Injury in the Criminal Justice System June 27, 2017 Lance E. Trexler, Ph. D, FACRM Rehabilitation Hospital of Indiana University School of Medicine

The Biological Basis of Our Identity, Consciousness, and Adaptability

Men ought to know that from nothing else but the brain come joys, delights, laughter and sports, and sorrows, griefs, despondency, and lamentations. And by this, in an especial manner, we acquire wisdom and knowledge, and see and hear and know what are foul and what are fair, what are bad and what are good, what are sweet and what are unsavory… And by the same organ we become mad and delirious, and fears and terrors assail us…All these things we endure from the brain when it is not healthy…In these ways I am of the opinion that the brain exercises the greatest power in man. -Hippocrates, On the Sacred Disease (Fourth century B. C. )

Incidence & Prevalence of Traumatic Brain Injury 1. 74 million/year requiring a physician visit Severity ranges from mild (80%) to moderate to severe (20%) 3. 32 -5. 3 million have long-term disability People with history of TBI are 66% more likely to receive welfare or disability payments Ma, VY, Chan, L, & Carruthers, KJ. (2014). Incidence, prevalence, costs, and impact on disability of common conditions requiring rehabilitation in the United States: Stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, osteoarthritis, rheumatoid arthritis, limb loss, and back pain. Archives of Physical Medicine and Rehabilitation, 95: 986 -995.

Costs Associated with Traumatic Brain Injury $13. 1 Billion in 2013 dollars are direct costs $64. 7 Billion in lost productivity $63. 4 -79. 1 Billion in medical costs Ma, VY, Chan, L, & Carruthers, KJ. (2014). Incidence, prevalence, costs, and impact on disability of common conditions requiring rehabilitation in the United States: Stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, osteoarthritis, rheumatoid arthritis, limb loss, and back pain. Archives of Physical Medicine and Rehabilitation, 95: 986 -995.

Indiana Prevalence of Traumatic Brain Injury 2, 472 Annual hospitalizations for just Traumatic Brain Injury 13, 282 (20%) are moderate to severe, and have chronic disability 66, 410 Hoosiers living with Traumatic Brain Injuries CDC has determined that moderate to severe brain injury is a lifelong condition Economic Impact of Resource Facilitation: Workforce Re-entry Following Traumatic Brain Injury, Srikant Devaraj, Ph. D, Michael Hicks, Ph. D, Brandon Patterson Graduate Research Assistant, Center for Business and Economic Research, Miller College of Business, Ball State University, February 21, 2017.

Epidemiology U. S. 2006 -2010 7 http: //www. cdc. gov/traumaticbraininjury/get_the_facts. html

Epidemiology Stroke is the leading cause of serious, long-term disability in the United States. Strokes can and do occur at ANY age. Nearly one fourth of strokes occur in people under the age of 65. 8 http: //www. strokecenter. org/patients/about-stroke/strokestatistics/

The “Umbrella” of Acquired Brain Injury A 9 cquired B I rain njury

ABI There are two categories of ABI, traumatic and nontraumatic. Traumatic Contusion Diffuse Axonal Injury (DAI) Non-traumatic 10 Stroke Anoxic / Hypoxic Brain Tumor Brain Surgery Infection Toxic / Metabolic Injury Electrocution / Struck by lightning
 “TBI occurs when an external mechanical force causes brain dysfunction.")
Traumatic Brain Injury (TBI) “TBI occurs when an external mechanical force causes brain dysfunction. ” (Mayo Clinic) “Traumatic brain injury (TBI) is a nondegenerative, noncongenital insult to the brain from an external mechanical force, possibly leading to permanent or temporary impairment of cognitive, physical, and psychosocial functions, with an associated diminished or altered state of consciousness. ” 11

Mechanisms of Traumatic Injuries Coup – Contrecoup injury 12 Diffuse Axonal Injury

Severity of TBI Mild Moderate Severe Normal / Abnormal LOC 0 -30 minutes > 30 minutes < 24 hours > 24 hours AOC A moment up to 24 hours > 24 hours Severity based on other criteria PTA 0 -1 day > 1 and < 7 days > 7 days GCS 13 -15 9 -12 3 -8 Imaging Classification based on 2009 VA/Do. D Clinical Practice Guidelines for Management of Concussion/Mild Traumatic Brain Injury *LOC = loss of consciousness *AOC = alteration of consciousness / mental state *PTA = post-traumatic amnesia *GCS = Glasgow Coma Scale

Severity of TBI 14

Moderate to Severe TBI Basic cognitive skills may be disrupted: Sustaining attention Concentrating on tasks at hand Remembering newly learned material Processing of information Solving problems / making decisions Neurobehavioral changes are common: Decreased inhibition and impulsivity Difficulty with initiation Diminished awareness of weaknesses / limitations Social inappropriateness Possible emotional & social consequences: 15 Increased irritability / aggression Depression & anxiety Mood lability Social withdrawal *** Can also experience physical & other medical complications related to the TBI

TBI Consequence 16 Functional Impact on Behavior Attention deficit → Difficulty focusing on or responding to required tasks or directions on the job or in the classroom Memory deficit → Difficulty understanding or remembering new information or directions Irritability or Anger → Incidents with co-workers / supervisors Uninhibited or Impulsive Behavior → Poor Inhibition of emotions or desires (e. g. , making inappropriate jokes, drug use, rage) Executive Function deficit → Difficulty organizing behavior to execute stated intentions or goals (e. g. , don’t actually do what they wanted or said they would do)
 m. TBI and concussion are often thought of as interchangeable")
Mild TBI (m. TBI) m. TBI and concussion are often thought of as interchangeable terms Diagnostic Criteria for MTBI by the American Congress of Rehabilitation Medicine A traumatically induced physiological disruption of brain function, as manifested by at least one of the following: Any loss of consciousness Any loss of memory before or after injury Any alteration of mental state Focal neurological deficit that may or may not be transient Severity of Injury does not exceed the following: LOC ≤ 30 minutes After 30 minutes, an initial GCS score of 13 -15 PTA ≤ 24 hours 17

Common Consequences of m. TBI Acute Symptoms Behavioral Emotional Physical • • 18 Headache Nausea Vomiting Blurred or Double Vision Seeing Stars or lights Dizziness Sensitivity to light or noise Tinnitus • • • Drowsiness Fatigue/Lethargy Irritability Anxiety Depression Sleeping more than Usual • Difficulty Falling Asleep Cognitive • Feeling “Slowed Down” • Feeling “in a Fog” or “dazed” • Difficulty Concentratiing • Difficulty Remembering
 History of head trauma with LOC preceding symptom onset by a")
PCS Diagnosis (ICD-10) History of head trauma with LOC preceding symptom onset by a maximum of 4 weeks Symptoms in 3 or more of the following categories: Headache, dizziness, malaise, fatigue, noise intolerance Irritability, depression, anxiety, emotional lability Subjective concentration, memory or intellectual difficulties w/o neuropsychological evidence of marked impairment Insomnia Reduced alcohol tolerance Preoccupation with Sx’s, fear of brain damage with hypochondriacal concern and adoption of sick role 19
 Diagnosed concussion PCS is a “hot topic” and")
m. TBI and Post-concussive syndrome (PCS) Diagnosed concussion PCS is a “hot topic” and heavily debated Diagnostic criteria can vary Symptoms appearing within one week Symptoms of at least 3 months duration Symptoms typically resolve within 3 -6 months Roughly 10 -20% have continued symptoms Persistent Post-Concussive Syndrome (PPCS) Symptoms lasting longer than 3 or 6 months “Permanent” PCS? ? ? 20
 “Miserable Minority” Prevalence estimates vary: < 5% by 6 -12 months")
Persistent PCS (PPCS) “Miserable Minority” Prevalence estimates vary: < 5% by 6 -12 months (Iverson, 2005) 7 -15% have any symptoms one year postinjury (Hall et al. , 2005) 10 -20% of MTBI pts who have persistent symptoms at 6 -12 months and beyond (Millis and Putnam, 1996) Incidence of PPCS: ~ 27/100, 000 Equal to annual incidence of Parkinson’s Disease, Multiple Sclerosis, Guillain-Barre, motor neuron disease, myasthenia gravis combined (Satz, et al. , 1999) 21

Secondary Post-traumatic Injury Initial injury sets in motion molecular and hormonal changes in the brain These chemical reactions can be destructive to the brain These changes can continue to occur for weeks to years post-traumatic injury 22

Non-traumatic Brain Injuries Stroke Anoxic / Hypoxic Brain Tumor Brain Surgery Infection Toxic / Metabolic Injury Electrocution / Struck by lightning Hydrocephalus 23

Stroke Ischemic Stroke Most common type of stroke DWI = Diffusion-weighted imaging 24 The Internet Stroke Center

Stroke Intracerebral Hemorrhage Subarachnoid Hemorrhage The Internet Stroke Center 25

Anoxic / Hypoxic Anoxic brain injury is a result of a lack of oxygen Hypoxia is the term used to describe low oxygen Brain cells without oxygen will begin to die in about 4 minutes 26

Anoxic / Hypoxic Causes Oxygen is carried to the brain in the blood. Anoxic brain damage may occur if: Blood flow to the brain is blocked or slowed. This can happen with: Blood clot or stroke Shock and heart problems, like heart attack The blood flow is normal but the blood is not carrying enough oxygen. This may happen if: The individual has lung disease There is a lack of oxygen in the air, which may occur at high altitudes The individual experiences prolonged exposure to certain poisons or other toxins, such as carbon monoxide The individual experiences an event that stops them from breathing normally, such as drowning, choking, or suffocation Icahn School of Medicine at Mount Sinai 2015 27

Brain Tumor Classified into 2 categories Primary Originates within brain tissue Astrocytoma Oligodendrogliomas Ependymomas Meningiomas Others 28 Secondary Caused from cancer that originates in another part of the body Metastasis to the brain from: lung, melanoma, kidney, breast, bladder, others

Infection CNS can become vulnerable to infection most commonly by bacteria and viruses, but also parasites, fungi, and other organisms (more rarely) Infection Inflammation Depending on the location of the infection, different names are given to the diseases Meningitis Encephalitis Abscess 29

Encephalitis 30 The Encephalitis Society

Toxic / Metabolic Injury ~ 1, 000 substances identified as possibly neurotoxic Categories of substances: Metals – e. g. , lead, mercury, manganese Pesticides – many types Solvents & Fuels – e. g. , glues, paints, thinners Carbon Monoxide 31

Electrocution / Struck by Lightening High voltage electric shock or lightening strike can cause damage to the CNS, including the brain Immediate effects are usually obvious E. g. , burns, cardiac arrhythmias, paresthesias, seizures, sensory and motor deficits Sometimes there is a delayed onset of symptoms Due to progressive cellular damage and death Can occur days to years post-injury Long-term effects might be more subtle, pervasive, and less well-defined Wesner & Hickie, 2013 32

Hydrocephalus A result of excessive accumulation of fluid in the brain A. K. A. – “water on the brain” “Water” = Cerebrospinal fluid (CSF) Most commonly treated by inserting a shunt system 33

Recovery Post-Brain Injury Myth or Fact? 1. Acute severity can accurately predict post-acute MYTH 2. The amount of time the person with a brain injury FACT 3. Knowing which parts of the brain have been injured MYTH severity. remains in a coma is one of the factors that affects recovery. will tell you the specific challenges to expect. 4. Most recoveries for brain injury show steady improvement up until 2 years when recovery is complete. 5. With support, many people can change their behavior after a brain injury. MYTH FACT
")
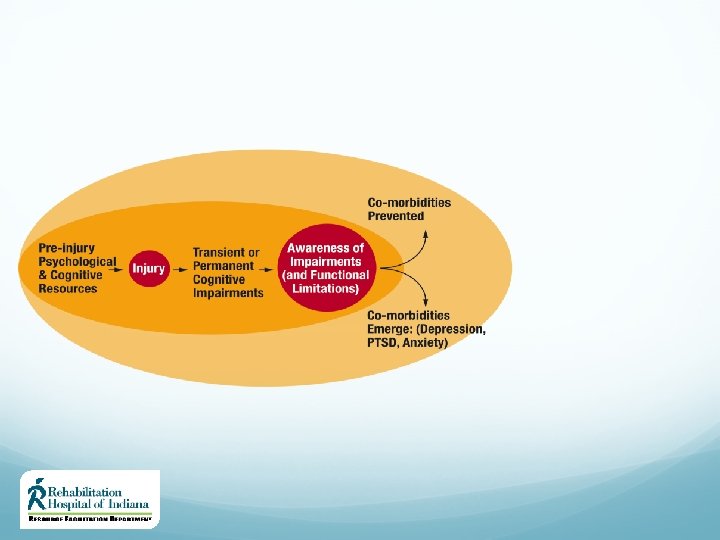
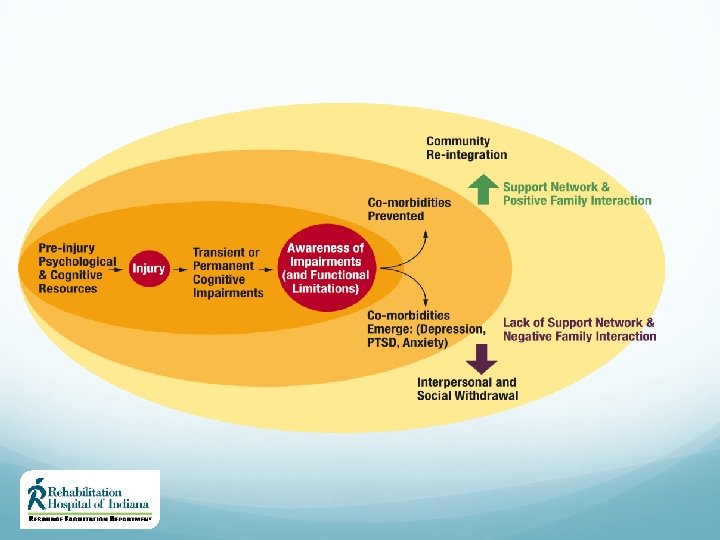
“Recovery” after TBI (Brooks, 1984)

Determinants of Recovery Factors Affecting Initial Response to TBI Environmental Factors Personal Factors Medical Care Factors 36 Factors Affecting Recovery from TBI Mechanism of Injury Multiple TBIs Polytrauma Severity of injury Social support Family functioning Transportation access Age Cognitive reserve Genetics Premorbid mental health Neurobehavioral issues Comorbid conditions Pain Sleep disturbance Access to acute care Quality of care Access to post-acute care Quality of care

Determinants of Recovery Factors affecting cognitive and functional recovery from TBI: Premorbid Conditions Comorbidities Contextual Factors https: //www. nap. edu/read/13220/chapter/6 37

Determinants of Recovery Premorbid Conditions ADHD, learning disabilities, developmental disabilities, syndrome on the Autism spectrum Pre-injury psychiatric conditions including personality and substance use disorders Lack of social support systems Low socioeconomic status Uninsured / Underinsured Low educational status Low IQ 38 https: //www. nap. edu/read/13220/chapter/6

Determinants of Recovery Comorbidities Can include behavioral, psychiatric, physical, or cognitive disorders – mostly causal associations E. g. Depression and anxiety related to the effects of the injury Post-traumatic seizure disorder Neurobehavioral syndromes Vision impairment Fatigue Headache / pain Sleep disturbance Co-occurring injuries may include multi-trauma such as broken bones 39

Determinants of Recovery Contextual Factors Family and social support play a key role in recovery post-TBI The dynamic of family functioning (poor and good) can directly affect one’s potential for optimal recovery Access to appropriate rehabilitation resources may be limited due to geographical restrictions and/or limited funding 40

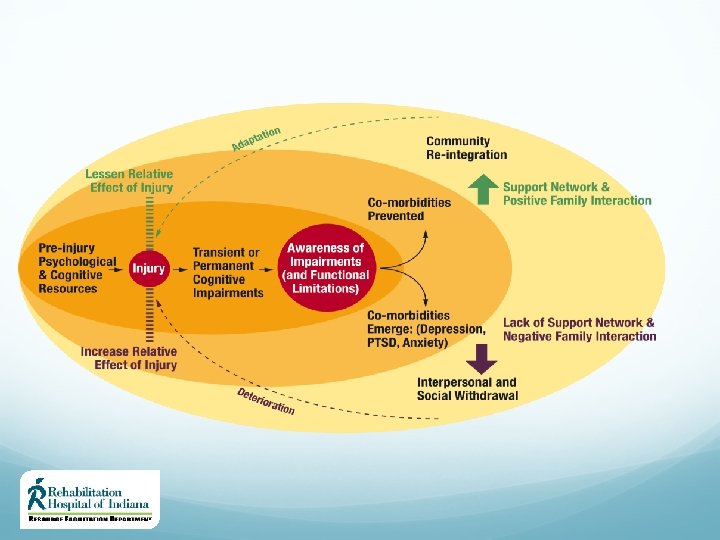

Chronic Condition ≠ Stable Condition TBI Model System National Data & Statistical Center % 2 categ. Declined 100% 80% 60% % 1 categ. Declined 8, 8% 11, 5% 48, 2% % no change 12, 9% 0% % 2 categ. Improved 20, 7% 23, 7% 13, 3% 8, 2% 14, 2% 44, 8% 40% 20% % 1 categ. Improved 41, 8% 39, 2% 19, 0% 17, 3% 12, 5% 10, 8% 8, 7% 10, 3% Year 2 vs. Year 1 (N=4, 986) Year 5 vs. Year 2 (N=2, 867) Year 10 vs. Year 5 (N=796) Year 15 vs. Year 10 (N=194) 15, 5% Change in GOS 18, 6%

Indiana Public Health Implications 18% return to work 50% return to hospital at least once 33% rely on others for help with everyday activities 29% are not satisfied with life 29% use illicit drugs or misuse alcohol 22% reside in nursing homes Moderate to severe traumatic brain injury is a lifelong condition. Center for Disease Control and Prevention. https: //www. cdc. gov/traumaticbraininjury/pdf/moderate_to_severe_tbi_lifelong-a. pdf

CDC Recommendations Recognize brain injury as a chronic health condition Screen for brain injury in state-funded health and social services Train health and social service professionals on brain injury Develop proactive lifelong disease (condition) management strategies Moderate to severe traumatic brain injury is a lifelong condition. Center for Disease Control and Prevention. https: //www. cdc. gov/traumaticbraininjury/pdf/moderate_to_severe_tbi_lifelong-a. pdf

Brain Injury Affects All State Agencies Brain Injury is a risk factor for incarceration Brain Injury is a significant risk factor for substance/ETOH abuse 40 -60% of brain injury patients develop psychiatric co-morbidity (e. g. , depression) Neurobehavioral impairments not well managed which result in out-of-state placements Brain injury is typically unrecognized and misdiagnosed in the mental health system (especially bi-polar disorder) Patients with brain injury don’t benefit from typical mental health and substance abuse treatment secondary to cognitive impairments (e. g. , memory) Return to work rate of 18% = significant societal cost and family burden
- Slides: 51