Brain Aging Dementia management A Dean Sherzai MD
 Director of")
Brain Aging Dementia & management A. Dean Sherzai MD, MAS, Ph. D(c) Director of Loma Linda Memory and Aging Center Director of Loma Linda University Neurology Research Program

Normal Aging

CENTENARIANS 1900 – RARE 1982 – 32, 000 1998 – 61, 000 2050 – 600, 000

SUPER-CENTENARIANS
 > 90 Michelangelo sculpted at")
Active Aging Artists: Picasso > 90 T. Vecellio (Titian) > 90 Michelangelo sculpted at 89 Composers: Verdi wrote Falstaff at 84 Scientists: Galileo > 70 Linus Pauling > 80 Performers: Martha Graham danced till 75 choreographed @ 95 Artur Rubinstein last recital at 93 Writers: too numerous to mention. . .

Definitions • Normal Brain Aging • Mild Cognitive Impairment • Dementia

Aging, memory and intellect Don’t change Verbal IQ Vocabulary Store of information Comprehension Decrease • Speed of memory retrieval • Speed of processing • Multi-tasking ability • Memory-formation efficiency

Common Cognitive Complaints in Normal Adults Situation Percentage of elderly Names 83 % Where I put things 60 % Knowing I have told someone 49 % something Forgetting a task after starting 41 % Losing the thread of conversation 40 % From: Boller et al, Arch Neurol 1991

Brain Changes With Aging • Brain weight: – Decreases by about 0. 5% per year after age 30 • Neuron loss: – Region-specific – 10 -25% loss in cerebellum, cortex, hippocampus, substantia nigra, Frontal Lobe • Loss of synapses (connections between neurons) • Mild degree of Alzheimer-type pathology

Causes of Memory Changes in Aging • Normal aging * • Neurodegenerative diseases / Alzheimer’s disease • Medications • Alcohol • Depression • Anxiety • Head trauma

Variability of Aging depends on: • Heredity: – Presence of longevity genes – Absence of disease genes • Lifestyle: – Diet – Body weight – Exercise • Luck: – Avoiding disease and trauma

Normal Aging Alzheimer’s disease Mild Cognitive Impairment No change over time Other dementias

Mild Cognitive Impairment • Variable defintion • Originally defined as a memory only syndrome • Defined loosely -include memory and cognitive problems, yet normal ability to do ADLs • Conversion to AD at a rate of about 10 -15%/year • Normal elderly – 1 -2% per year • The non- memory types are those at risk for other types of dementia

Why is identifying at MCI stage important? • Study the conversion of MCI to AD – Intervene with drugs – Predict who is at the greatest risk for developing the disease • It appears that intervention at the MCI stage may be more effective

What is Dementia? Loss of memory and other intellectual abilities serious enough to interfere with daily life Alzheimer’s is most common form of dementia

TYPES OF DEMENTIA • Degenerative • Non degenerative ‣ Vascular Dementia ‣ Bacterial/Viral infections ‣ Syphilis, cryptococcus, Lyme Dz. , Whipple’s Dz. , ‣ ‣ ‣ ‣ HIV/AIDS, SSPE, PML, ect. Prion disease (e. g. , CJS) Neoplasia (brain tumors, carcinomatos meningitis, paraneoplastic synd. ) Vitamin deficiency (e. g. , Pellegra, B 12 deficiency) Endocrine deficiencies (e. g. , Thyroid dz. , Hashimoto’s encephalitis, Cushing’s) Cerebral trauma (SDH, Concussions) Toxins (Alcohol, drugs, heavy metals) Others: NPH, Hydrocephalus, MS, Dialysis, Depression, TBI
 Lewy Body Disease (20%) FTLD (2 -5%)")
Degenerative Diseases • • Alzheimer’s disease (>60%) Lewy Body Disease (20%) FTLD (2 -5%) Parkinson’s disease and Dementia (PDD) Huntington’s PSP Some others: CBGD, Kearns-Sayre, Hallervorden-Spatz, Wilson’s dz, etc.

What is AD? AD Statistics…. • Most common cause of dementia among people age 65 and older. • 5. 3 million people now have AD. • 1 out of 8 over 65; 1 out of • By 2050, 13. 2 million older 2 over 85 Americans are expected to have • For every 5 -year age group AD if the current numbers hold beyond 65, the percentage of people with AD doubles. and no preventive treatments become available.

Impact of AD Once considered a rare disorder, Alzheimer’s disease is now seen as a major public health problem that is seriously affecting millions of older Americans and their families.

AD and the Brain The Changing Brain in Alzheimer’s Disease No one knows what causes AD to begin, but we do know a lot about what happens in the brain once AD takes hold. Pet Scan of Normal Brain Pet Scan of Alzheimer’s Disease Brain

Medial Temporal Lobe

AD and the Brain Plaques and Tangles: The Hallmarks of AD The brains of people with AD have an abundance of two abnormal structures: • beta-amyloid plaques, which are dense deposits of protein and cellular material that accumulate outside and around nerve cells • neurofibrillary tangles, which are twisted fibers that build up inside the nerve cell An actual AD plaque An actual AD tangle
 is the precursor")
AD and the Brain Beta-amyloid Plaques 1. Amyloid precursor protein (APP) is the precursor to amyloid plaque. 1. APP sticks through the neuron membrane. 2. 3. 2. Enzymes cut the APP into fragments of protein, including beta-amyloid. 3. Beta-amyloid fragments come together in clumps to form plaques. In AD, many of these clumps form, disrupting the work of neurons. This affects the hippocampus and other areas of the cerebral cortex.
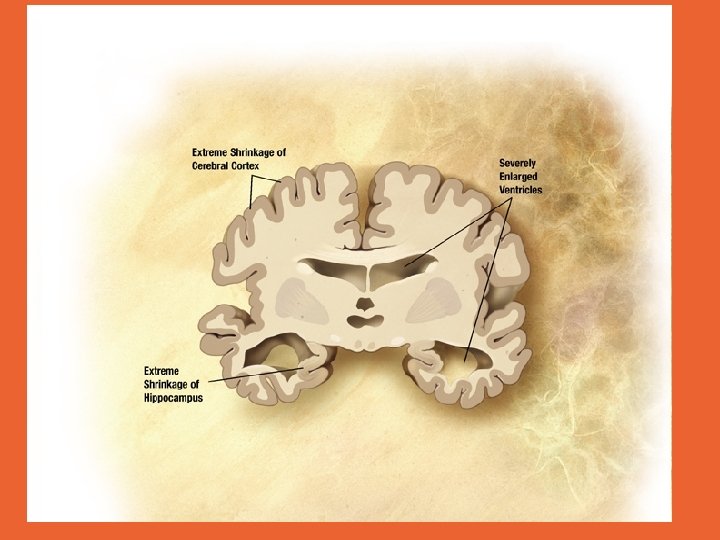

Ultimately the brain Shrinks

Risk factors for AD • Major Risks • Age • Family history • Genes (Apo E 4, others) • Minor Risks • Head trauma • Low education • Female sex • • • ? Protective factors NSAID use Estrogen use Statins Anti-oxidants Exercise Diet Mental activity Psychosocial factors
 – Apo. E 4: stratifies")
Genetics of AD • Genetic component (present in <10%) – Apo. E 4: stratifies risk of development, no guarantee – Presenilin 1 (most common) and 2 – Amyloid Precursor protein (chr. 21) – Alpha 2 macroglobulin – all generally increase risk for early onset AD – More genes are being discovered

Warning Signs • Memory changes that disrupt daily life • Challenges in planning or solving problems • Difficult completing familiar tasks • Confusion with time or place • Trouble understanding visual images and spatial relationships
 • New problems with words • Misplacing things and losing")
Warning Signs (cont. ) • New problems with words • Misplacing things and losing ability to retrace steps • Decreased or poor judgement • Withdrawal from work or social activities • Changes in mood and personality
 & other Neuropsycholgical testing • Imaging •")
Evaluation • Informant history • MMSE (Folstein) & other Neuropsycholgical testing • Imaging • Activities of daily living (ADLs) • Medical history – Medication – Comorbidities

AD Research: Diagnosing AD Experienced physicians in specialized AD centers can now diagnose AD with > 90% accuracy. Early diagnosis has advantages: • Doctors can rule out other conditions that may cause dementia. • If it is AD, families have more time to plan for the future. • Treatments can start earlier, when they may be more effective. • It helps scientists learn more about the causes and development of AD.

Imaging • • • SPECT Structural MRI / Volumetrics Functional MRI PET PIB

Structural imaging MRI

Functional MRI

PET Scan

Positive PIB PET MCI Negitive PIB PET MCI Non-progressor
")
CSF and Peripheral Biomarkers • • A Beta 42 (A beta Amyloid 1 -42) T-tau (total Tau) P-Tau (phosphorylated tau) Others to be validated
 (5 mg, 10 mg, 23")
Treatments for Alzheimer’s Disease Cholesterase Inhibitors • Donepezil (Aricept) (5 mg, 10 mg, 23 mg) • Rivastigmine (Exelon) (1. 5 mg x 2, 3. 0 mg x 2, 4. 5 mg x 2, 6 mg x 2) • Rivastigmine Patch (Exelon patch) (4. 6 mg x 2, 9. 5 mg x 2) • Galantamine (Razadyne) (4 mg x 2, 8 mg x 2, 12 mg x 2) NMDA Receptor Antagonist • Mentantine (Namenda) (10 mg x 2)

Treatment Benefits • Individuals performed better on tests of memory and thinking • May delay or slow worsening of symptoms for about 6 – 12 months • People with moderate to severe AD may benefit slightly from taking memantine too

Issues in subjects with Dementia • Behavioral issues • Hallucinations • Sleep problems • Diminished appetite • Difficulty swallowing

Behavioral Problems • Very Common & Recurrent • Different manifestations – Active vs. Passive – Severity – Situational vs. Pervasive • Many sources and causes • Often related to Communication issues • Adverse consequences

Consequences of Untreated behavioral problems • Excess disability / disproportional presentation • Elevated caregiver depression & burder • Increased service utilization • Increased risk of institutionalization • Lower quality of life • Risk of harm to person or others
 • Environmental issues –")
Underlying causes • Unmet needs, and frustrations (emotional & physical) • Environmental issues – cold/ warm – noise • Biological issues – other disease process – degenerative process

ABC model • Antecedents -Behaviors-Consequences • first describe the behavior well • Identify the antecedents and triggers • specify consequences / outcome responses • develop an action plan according to the person and environment

Treatment • What should not be done – Argue and or convince – Negative emotions from care giver • What is useful – Redirecting – Distracting • Drug Treatment
 • Family psychoeducation • Caregiver")
Primay Approach to Behavioral problesm • Proactive assessment (NPI) • Family psychoeducation • Caregiver support & referral (e. g. AA) • ABC approach – behavioral 1 st then Pharmaceutical • Develop & document plan and goals • follow up and change plan regularly

AD Research: the Search for Causes Epidemiologic Studies Scientists examine characteristics, lifestyles, and disease rates of groups of people to gather clues about possible causes of AD. The NIA is currently funding epidemiologic studies in a variety of different groups. Two of the studies focus on religious communities. Researchers conduct yearly exams of physical and mental status, and studies of donated brains at autopsy. Some early results indicate: • Mentally stimulating activity protects the brain in some ways. • In early life, higher skills in grammar and density of ideas are associated with protection against AD in late life.

AD Research: Clinical Trials Clinical trials are the primary way that researchers find out if a promising treatment is safe and effective. • Trials examine approved drugs to see if they can be used for other purposes, or look at experimental drugs. • Participating in a trial means regular contact with the study team, who can provide state-ofthe-art AD care.

AD Research: the Search for New Treatments Researchers also are looking at other treatments, including: • vaccine against AD. • • cholesterol-lowering drugs called statins anti-oxidants (vitamins) and folic acid anti-inflammatory drugs substances that prevent formation of beta-amyloid plaques • nerve growth factor to keep neurons healthy

Research at Loma Linda University • Looking at the influence of Diet and lifestyle on development of neurodegenerative diseases (Dementia, PD, etc), and Stroke • Community based approach to aging research and aging support • Novel Imaging approaches to early detection of Dementia • Clinical trials

Why early diagnosis & follow-up is important • Major cause for mortality and morbidity is late treatment of behavioral disorder • Early identification means – Behavioral and enviromental measures work – Can start with milder drugs – Can control the progression and treatment – Not forced into high doses of strong medications – Not forced into early irreversible decisions

National Support for Caregivers Alzheimer’s Association • Local chapters provide referrals to area resources and services, and sponsor the Safe Return Program, support groups, and educational programs: 1 -800 -272 -3900 www. alz. org Eldercare Locator • Nationwide service of the Federal Government helps caregivers locate local support and resources: 1 -800 -677 -1116 www. eldercare. gov Slide 40

For more information on Alzheimer’s disease and a list of the NIA-funded Alzheimer’s Disease Centers, contact the Alzheimer’s Disease Education and Referral (ADEAR) Center at: 1 -800 -4380 www. alzheimers. org The ADEAR Center is a service of: National Institute on Aging, part of the National Institutes of Health (NIH), part of the Department of Health and Human Services This Power. Point slideshow is based on the publication Alzheimer’s Disease: Unraveling the Mystery. Contact the ADEAR Center for free copies. Slide 41

USE IT OR LOSE IT! • Don’t be a couch potato – Socially active, verbally active • Keep healthy habits – Good nutrition, mild exercise, take your medicines and don’t sweat the small stuff! • Life-long learning = long-life living – Mentally active- “Use it or lose it!” – (e. g. Keep going to educational lectures)

Loma Linda University Memory Disorders Clinic • Focus – Accurate and early diagnosis – Treatment – Potential Prevention – Research • Outreach to patients, their families, and community • QOL programs
 LOMA LINDA UNIVERSITY Faculty Medical")
MEMORY DISORDERS CLINIC Loma. Linda. Memory. org (under construction) LOMA LINDA UNIVERSITY Faculty Medical Offices 11370 Anderson ave B 100 Appointments: 909 -558 -2880 Messages: 909 -558 -2233 Fax: 909 -558 -2237

Thank you! Questions?
- Slides: 57