Brachial artery injury Supparerk Prichayudh M D Anatomy

Brachial artery injury Supparerk Prichayudh, M. D.

Anatomy • Course – – Teres major m. Medial bicipital sulcus Cubital fossa Bifurcation (opposite to radial head) • Branches – Deep brachial a. – Ulnar collateral a. (superior and inferior)

Ligation of brachial a. proximal to Deep brachial a. should not be performed due to poor collateral circulations in this area.

the anastomosis around the elbow-joint.

• Medial bicipital sulcus – Coracobrachialis m. , Biceps m. – Triceps m. • Cubital fossa – Artery lies medial to biceps tendon, coverd by bicipital aponeurosis. Median n. Ulnar n.

Venous system • Deep – Accompanied by a pair of venae comitantes • Superficial – Basilic v. – Cephalic v. – Median cubital v. • All drain into the axillary v.

• Basilic v. – Medial – Arm level • Accompanied by 2 medial antebrachial cutaneous n. • Upper 2/3 underneath the fascia, medial to Brachial a. • Cephalic v – Lateral – Runs superficially – Deltopectoral groove underneath the fascia

Incidence and Mechanism • Vascular Trauma – 50% neck, torso – 50% extremities • Brachial artery most common in UEVI (30 -50%) • Penetrating most common (70 -80%), Urban • Blunt Rural
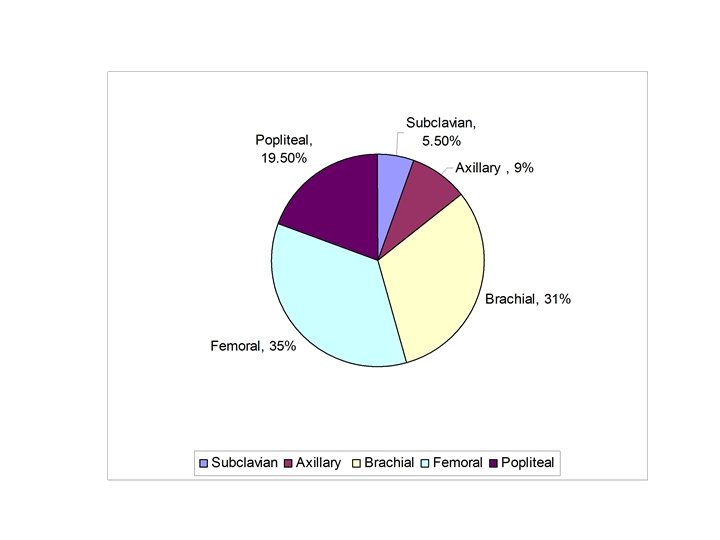

43. 5% 42. 5% 7% 1% 3% 3%
 • 52 patients with UEVIs, Blunt 25 (48%), Penetrating 27")
Incidence in Thailand (20022007) • 52 patients with UEVIs, Blunt 25 (48%), Penetrating 27 (52%) • The mean ischemia time was 10. 07 h. • The mean ISS was 17. 52. • subclavian artery 12 (23%), axillary artery 3 (5. 76%) , brachial artery 18 (34. 61%), radial artery and/or ulnar artery 19 (36. 54%) Management of upper extremity vascular injury: outcome related to the Mangled Extremity Severity Score. Prichayudh S, Verananvattna A, Sriussadaporn S, Kritayakirana K, Pak-art R, Capin A, Pereira B, Tsunoyama T, Pena D. World J Surg. 2009 Apr; 33(4): 857 -63.

Diagnosis • PE • Arterial Pressure Index – Injured limb SBP/ Uninjured limb SBP – < 0. 9 specificity 97%, sensitivity 95% – > 0. 9 NPV 99% • Doppler US – sensitivity 50% • CTA • Angiography gold standard
")
Hard vs. Soft signs of Vascular injury Hard signs Soft signs Active arterial (pulsatile) Minor bleeding Pulseless/ ischemia Injury in proximity to major vessel Expanding pulsatile hematoma Bruit or thrill Small to moderate size hematoma Associated nerve injury API < 0. 9 Operation Mandatory Further W/U
 Doppler velocity waveform – rapid antegrade flow reaching a")
Doppler signal • normal (“triphasic”) Doppler velocity waveform – rapid antegrade flow reaching a peak during systole – transient reversal of flow during early diastole – slow antegrade flow during late diastole.

Indication for angiography • Hemodynamic stability • Uncertain diagnosis – Soft signs – PVD • Unclear location (location determine operative approach) – Multiple wounds, fractures – GSW parallel to an artery – Thoracic outlet wound

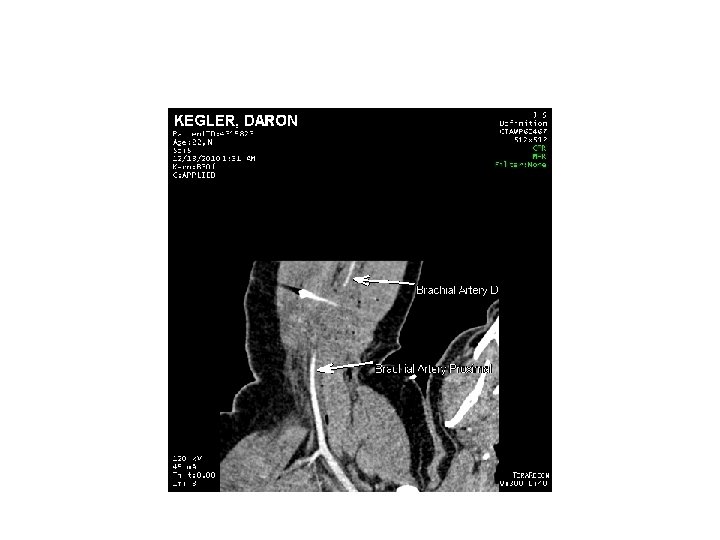
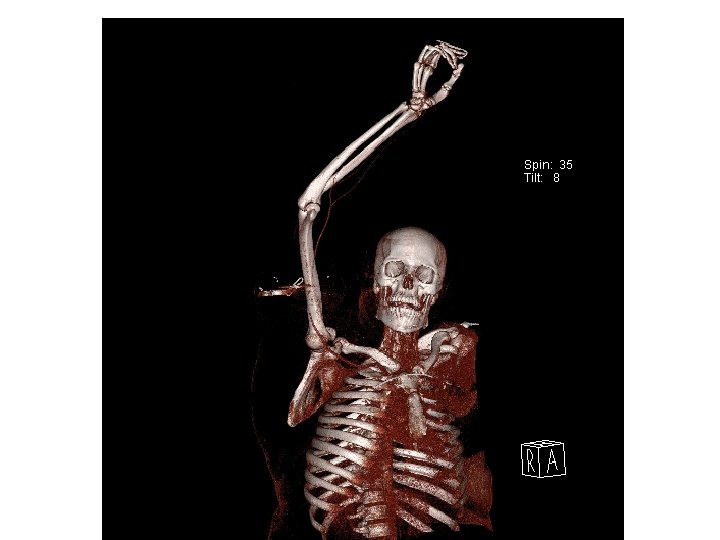
CTA

General Principle of management • ABCs – Temporary bleeding control digital pressure, Tourniquet • Active bleeding, limb threatening ischemia OR • Stable, good limb viability may investigate • Non-operative management non-occlusive lesion in asymptomatic patient • Pre-operative management – Prophylactic antibiotic – Single dose heparin iv if no C/I
 - Tourniquet - Intraoperative angiogram •")
Surgical treatment • Prepare for - leg (SVG) - Tourniquet - Intraoperative angiogram • Incision & exposure • Proximal & distal control • Identify injury and resect the injured segment • Thrombectomy with a Fogarty catheter obtain good inflow and back-bleeding before the repair.

Extensile exposure

Arm incision along bicipital sulcus

Cubital fossa S shape incision
 • Graft")
Repair options • Primary repair defect < 1 -2 cm (33 -67%) • Graft – Reverse SVG (31 -59%) – PTFE (6 -12%) • Combined vascular- orthopedic injury – Bone alignment 1 st – Limb threatening ischemia shunt • Damage control – Ligation (0 -1%) – Shunt (0 -2%) Risk factors for compartment syndrome in traumatic brachial artery injuries: an institutional experience in 139 patients. Kim JY, Buck DW 2 nd, Forte AJ, et al. J Trauma. 2009 Dec; 67(6): 1339 -44. Management of traumatic brachial artery injuries: a report on 49 patients. Ekim H, Tuncer M. Ann Saudi Med. 2009 Mar-Apr; 29(2): 105 -9.

Temporary shunts • In complex extremity vascular injury, Damage control • Heparin-bonded shunts – Argyle – Sundt • Self-constructed shunt - Inahara

Indications for Fasciotomy • • S & S of compartment syndrome compartment pressure > 30 - 35 mm. Hg ∆P (DBP-CP) < 30 mm. Hg Prophylactic – any combined arterial and venous injury – prolonged extremity ischemia > 4 -6 h – vascular injury associated with shock; crush injuries; combined skeletal and vascular extremity trauma; and the ligation of a major extremity vein or artery.

Risk Factors for Compartment Syndrome in Traumatic Brachial Artery Injuries • 139 patients – 29 (20. 9%) CS – 110 (79. 1%) No CS • GSW 67, Sharp LW 64, Blunt 7 • 1 Amputation in CS group Risk factors for compartment syndrome in traumatic brachial artery injuries: an institutional experience in 139 patients. Kim JY, Buck DW 2 nd, Forte AJ, et al. J Trauma. 2009 Dec; 67(6): 1339 -44.

Arm Compartments Anterior Posterior

Fasciotomy of the Anterior and Posterior Compartments of the Arm
 Dorsal")
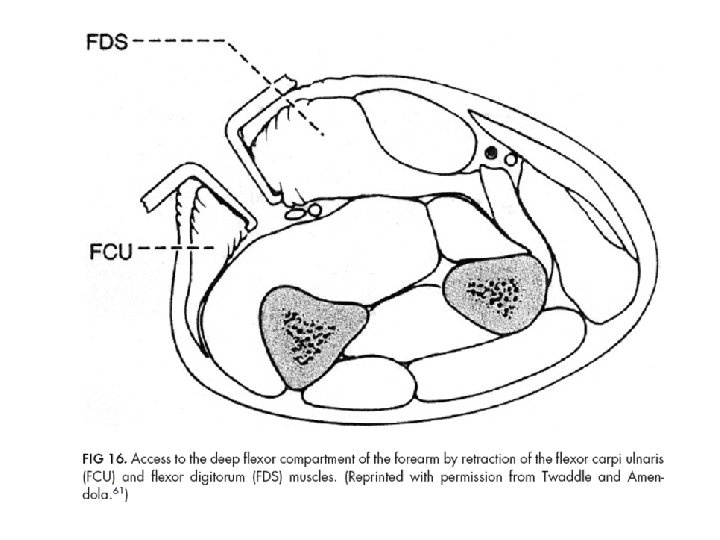
Forearm compartments Volar Lateral (Mobile WAD) Dorsal

Fasciotomy of the Forearm

Amputation: when? Non-viable or non-salvable limb Irreversible limb ischemia Extremely mangled limbs Severe necrotizing infection Safe life before limbs!!! Amputation can be life saving in life threatening extremity bleeding or infection. Functional outcome consideration

Clinical signs of irreversible limb ischemia • mottled, nonblanching skin • dark, tense, noncontracting muscles • Do not reperfuse the dead limb Reperfusion injury!!!!
 1 -14 Skeletal / soft-tissue injury Low energy (stab;")
Mangled Extremity Severity Score (MESS) 1 -14 Skeletal / soft-tissue injury Low energy (stab; simple fracture; pistol gunshot wound): 1 Medium energy (open or multiple fractures, dislocation): 2 High energy (high speed MVA or rifle GSW): 3 Very high energy (high speed trauma + gross contamination): 4 Limb ischemia No ischemia: 0* Pulse reduced or absent but perfusion normal: 1* Pulseless; paresthesias, diminished capillary refill: 2 * Cool, paralyzed, insensate, numb: 3* Shock Systolic BP always > 90 mm Hg: 0 Hypotensive transiently: 1 Persistent hypotension: 2 Age (years) < 30: 0 30 -50: 1 > 50: 2 * Score doubled for ischemia > 6 hours from Johansen et. al. 1990
: Lower extremity trauma")
MESS as a predictor for amputation • Johansen et al (1990): Lower extremity trauma • Slauterbeck et al (1994): Upper extremity trauma – MESS of > 7 was associated with a 100% amputation rate.
 -Amputation: clinical signs of irreversible limb ischemia")
-52 UEVI patients (52% penetrating, 48 %blunt) -Amputation: clinical signs of irreversible limb ischemia (skin & muscle changes) -Amputation rate 13%, all suffered from blunt injuries and had MESS > 7, 0% mortality rate. - We could avoid amputation in 12 of 19 patients (63%) who had a MESS >7. - MESS of >7 does not always mandate amputation.

Can the revised MESS score (i. e. , focusing more on the degree of skeletal/soft tissue injury) be applied to all comers to be a more sensitive predictor of limb salvage and the need for amputation?

Results Amputation rate 0 -6%, Compartment syndrome 1 -29%

Conclusions: Brachial a. injury • The most common vascular injury in upper extremities. • Early diagnosis – Hard signs, API < 0. 9 – Angiography Uncertain Dx or location • Early treatment – Hard signs+ limb threatening ischemia OR! • Outcome is good with low amputation rate.

CASE • 40 y/o male • 1 hr PTA: Bomb bleeding wound over Rt. Cubital fossa (arterial bleeding) • GCS 15 • Stable V/S • Further assessments

• Good sensation and motor function • Rt radial pulse not palpable, not dopplerable • Temporary bleeding control with digital pressure • X-ray Shrapnel, No fracture • IV fluid resuscitation • OR

Preparations? , incision?

• • • Prep whole Rt arm and shoulder Prep Rt groin SVG Heparin 5, 000 unit iv x 1 No tourniquet S shape incision

Repair options?

• • Interposition graft with reversed SVG Prolene 6 -0 No fasciotomy Good radial pulse after anastomosis No completion angiography 1 close suction drain Good function, D/C 1 wk Post op

THANK YOU
- Slides: 47