BPCO E PATIENTRELATED OUTCOMES IL VALORE AGGIUNTO DEI

BPCO E PATIENT-RELATED OUTCOMES: IL VALORE AGGIUNTO DEI NUOVI TRATTAMENTI FARMACOLOGICI Azienda Ospedaliera Pisana Università degli Studi di Pisa Pierluigi Paggiaro Dipartimento Cardio-Toracico e Vascolare, Università di Pisa Ottica Respiro 2016 Verona, 6 -7 maggio 2016

2

3

Cazzola et al, ERJ 2008 4

Clinical outcomes for COPD • Are they relevant ? • Measurable by MRC scale, BDI/TDI, rescue med. , … • Impact on quality of life and mortality • Are they improved by the pharmacologic treatment ? • Bronchodilators • Anti-inflammatory drugs • Focus on LABA/LAMA combinations • Are they better than single drug ? • Which relevance for the patient ?

Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD § Assess symptoms § Assess degree of airflow limitation using spirometry § Assess risk of exacerbations § Assess comorbidities © 2014 Global Initiative for Chronic Obstructive Lung Disease

COPD Importance of symptoms • Symptoms • Dyspnea • Cough • Sputum • Wheezing • Mild Variability • Day-by-day • Morning/night

COPD Importance of symptoms • Symptoms • Dyspnea • Cough • Sputum • wheezing • Mild Variability • Day-by-day • Morning/night

Poor correlation between symptoms and FEV 1

Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD § Assess symptoms Assess degree of airflow limitation using spirometry COPD Assessment Test (CAT) Assess risk of exacerbations Assess comorbidities or Clinical COPD Questionnaire (CCQ) or m. MRC Breathlessness scale © 2014 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD § Assess symptoms § Assess degree of airflow limitation using spirometry Assess risk of exacerbations Use spirometry for grading severity Assess comorbidities according to spirometry, using four grades split at 80%, 50% and 30% of predicted value © 2014 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD § Assess symptoms § Assess degree of airflow limitation using spirometry § Assess risk of exacerbations Assess comorbidities Use history of exacerbations and spirometry. Two exacerbations or more within the last year or an FEV 1 < 50 % of predicted value are indicators of high risk. Hospitalization for a COPD exacerbation associated with increased risk of death. © 2014 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD § Assess symptoms § Assess degree of airflow limitation using spirometry § Assess risk of exacerbations Combine these assessments for the purpose of improving management of COPD © 2014 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Assess symptoms first (C) (A) (D) (B) If CAT < 10 or m. MRC 0 -1: Less Symptoms/breathlessness (A or C) If CAT > 10 or m. MRC > 2: More Symptoms/breathlessness (B or D) CAT < 10 CAT > 10 Symptoms m. MRC 0– 1 m. MRC > 2 Breathlessness © 2014 Global Initiative for Chronic Obstructive Lung Disease
 or > 1 leading")
Global Strategy for Diagnosis, Management and Prevention of COPD (C) or > 1 leading to hospital admission (D) 3 2 (B) (A) 1 1 (not leading to hospital admission) 0 CAT < 10 CAT > 10 Symptoms m. MRC > 2 m. MRC 0– 1 Breathlessness © 2014 Global Initiative for Chronic Obstructive Lung Disease Risk 4 (Exacerbation history) ≥ 2 Risk (GOLD Classification of Airflow Limitation)) Combined Assessment of COPD

The different components of COPD • Different components of the disease: • Airway obstruction and hyperinflation • Responsable of: • Increased work of breathing limitation in exercise capacity • Dyspnea, poor Qo. L muscolo-scheletal consequences • Airway and lung inflammation • Responsable of: • Progression of the airway and lung parenchima damage • Rate and severity of exacerbations

The central role of airflow limitation in COPD Exercise Expiratory flow limitation Air trapping Hyperinflation Exacerbations Breathlessness Bronchodilators Quality of life Deconditioning Inactivity improve symptom control and clinical outcomes Reduced exercise capacity Disability Disease progression Death

Old and new long-acting bronchodilators • Beta 2 -agonists • Over 12 hrs: salmeterol, formoterol • Over 24 hrs: indacaterol, olodaterol, vilanterol • Anticholinergic drugs • Over 12 hrs: aclidinium • Over 24 hrs: tiotropium, glycopirronium umeclidinium

Long-acting Anticholinergic drugs for COPD Common characteristics • Highly selective for M 3 receptor • High affinity • Long half life

How to measure the efficacy of anticholinergic drugs in COPD Tiotropium Glycopirronium Aclidinium FEV 1 + 150 -200 ml + 120 -250 ml + 120 -150 ml Exacerbations - 14 -35% (3 yrs) - 34% TFE (1 yr) - 35% (6 mts) Exercise tolerance + 4 min ET + 90 sec + 116 sec PROs - 23 -3. 3 SGRQ - 4 SGRQ FEV 1 decline In moderate COPD n. a. Mortality - 11 -16 % n. a. Safety Large numbers Long follow-up CV AE (? ) > 2000 pts Up to 1 yr No MAE > 1000 pts Up to 6 mts No MAE

Izquierdo et al, IJCOPD 2016 PDC: proportion of days covered

Clinical outcomes for COPD Symptoms and rescue medication • Dyspnoea • Measurable by MRC scale, BDI/TDI • Cough and sputum • Rescue medication use • Short-acting beta 2 • Are they sensitive to pharmacologic treatment ? • Single drugs vs combinations

Clinically significant improvement in Qo. L and dyspnea with aclidinium 400 mcg bid Kevin et al, JCOPD 2012

LAS 39: study design 6 settimane Randomizzazione: 2: 2: 1 Aclidinio Bromuro 400 µg BID (n=171) Tiotropio 18 µg QD (n=158) Run in Giorni 1 & 2: − TFP seriati 24 ore l l Placebo (n=85) Farmaco di salvataggio e sintomi quotidiani della BPCO - EXACT-RS - Altri sintomi Giorni 42 & 43 – TFP seriati 24 ore – Preferenza per il device Studio multicentrico di Fase IIIb, randomizzato, in doppio cieco, double-dummy, controllato con placebo e confronto attivo, della durata di 6 settimane, su pazienti (n=414) con BPCO da moderata a grave Dopo lo screening e un run-in di 2 -3 settimane, i pazienti sono stati randomizzati (2: 2: 1) a ricevere il trattamento con Aclidinio Bromuro 400 μg b. i. d. al mattino e alla sera mediante l’inalatore multidose a polvere secca Genuair, Tiotropio 18 μg u. i. d. al mattino mediante l’inalatore Handi. Haler, oppure placebo per 6 settimane EXACT-RS, : EXAcerbations of Chronic Pulmonary Disease Tool-Respiratory Symptom)s; TFP, test di funzionalità polmonare Beier J et al. COPD 2013

Clinically significant improvement in through FEV 1 with aclidinium 400 mcg bid Beier et al, JCOPD 2013

Aclidinium bid improves diurnal and nocturnal symptoms better than tiotropium od Beier et al, JCOPD 2013

Symptom variability in COPD patients • Partidge, CMRO 2009 Online survey in COPD patients • Kessler, ERJ 2011 Clinic-based survey (GPs and specialists) • Agusti, ERR 2011 Nocturnal symptoms in COPD patients of different severity • «unreported exacerbations» • Asthma COPD Overlap Syndrome (ACOS)
 31. 0")
Respiratory symptoms are more frequent at early morning Mancanza di fiato (n=1769) 31. 0 24. 0 20 22. 5 19. 5 10 0 Pazienti (%) 40 Pazienti (%) 30 48. 9 A sera Tosse (n=1433) 10 0 Nel Più tardi nel Al risveglio mattino pomeriggio 26. 1 21. 7 18. 7 17. 3 A sera Di notte 25. 1 18. 3 Al Nel Più tardi nel A sera risveglio mattino pomeriggio Di notte Costrizione toracica (n=690) 40 22. 3 14. 9 31. 1 20 0 Di notte 30 20 30 10 10. 6 Nel Più tardi nel Al pomeriggio mattino risveglio Respiro sibilante (n=1018) 40 Pazienti (%) 40 30 28. 8 20 25. 9 25. 4 25. 5 16. 7 10 0 Nel Più tardi nel Al A sera pomeriggio risveglio mattino Di notte Kessler R et al. Eur Respir J 2011

COPD: nocturnal symptoms Incremento percentuale Prevalenza percentuale dei pazienti Intervalli di confidenza al 95% PRESENZA DI SINTOMI NOTTURNI SECONDO LA GRAVITÀ DELLA BPCO % del VEMS predetto più recente Uno studio condotto su 2. 848 pazienti ha mostrato che i sintomi notturni sono presenti in tutti gli stadi di gravità della malattia (presenti nel 67 % dei pazienti) La percentuale di pazienti che presentano sintomi notturni aumentava con il peggiorare della gravità della BPCO. Agusti A et al Eur Respir Rev 2011; 20: 121, 183– 194

Santus et al, Pulm Pharm & Ther 2015

Marth et al, Respir Med 2015

Clinical outcomes for COPD Exercise tolerance • Important impact on daily life activities • «vicious cyrcle» of COPD • Measurable with different tests • 6 MWT, SWT, daily activity • Improvement may strongly impact on nonrespiratory manifestations of COPD • Muscolo-skeletal function • Cardiovascular consequences 32

Poor physical activity is associated with high risk of hospitalization and mortality in COPD patients Mortality Hospitalization Garcia-Rio et al, Chest 2012

Long-lasting brochodilation improves systemic consequences of COPD o Allowing a better physical activity o Additional doses of bronchodilators on top on regular treatment o Bronchodilators on top of rehabilitation o Reducing systemic consequences of inactivity o As demonstrated in rehabilitation programmes o Increasing physical activity o Reducing cardiovascular events, osteoporosis, muscular disfunction, etc

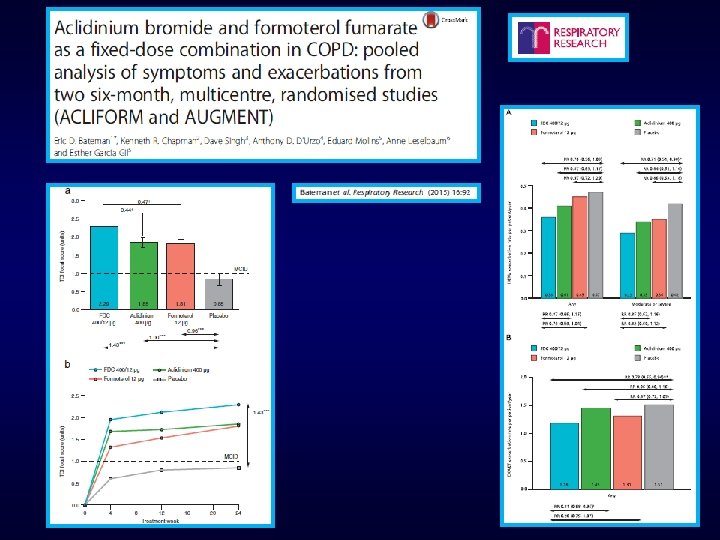
Beeh et al, BMC Pulm Med 2015

Pre-clinical data • Studied in normal subjects up to 6000 mcg Single doses No relevant side effects • Rapidly converted in two inactive metabolites by plasma hydrolysis Maximum plasma concentration in 5 -7 min T 1/2: 4. 6 -7 hours Steady state plasma concentration at 7 th day No accumulation • Predominantly renally excreted
 % remaining compound 120 100")
Aclidinium is rapidly hydrolyzed in human plasma (in vitro) % remaining compound 120 100 80 Aclidinium 60 Aclidinium half-life 2. 4 mins 40 Ipratropium Tiotropium 20 0 0 12 24 36 48 60 Time (minutes) Sentellas et al, Eur J Pharm Sci 2010

Global Strategy for Diagnosis, Management and Prevention of COPD Therapeutic Options: Bronchodilators § Long-acting inhaled bronchodilators are convenient and more effective for symptom relief than short-acting bronchodilators. § Long-acting inhaled bronchodilators reduce exacerbations and related hospitalizations and improve symptoms and health status. § Combining bronchodilators of different pharmacological classes may improve efficacy and decrease the risk of side effects compared to increasing the dose of a single bronchodilator. © 2013 Global Initiative for Chronic Obstructive Lung Disease

New LABA-LAMA combinations Singh, B J Clin Pharm 2015

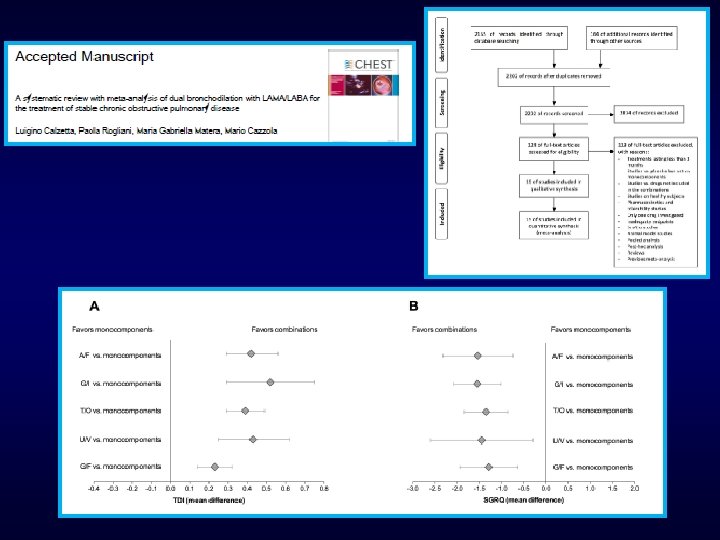
Oba et al, Thorax 2016

Oba et al, Thorax 2016

Oba et al, Thorax 2016

Oba et al, Thorax 2016

Oba et al, Thorax 2016

Oba et al, Thorax 2016

Maximizing bronchodilation with LABA/LAMA Which advanteges for patients ? o Improving symptoms and symptom-free days o Improving exercise capacity o Reducing exacerbations Improving quality of life o Prevention of FEV 1 decline ? o Small signal with monotherapy o Suggestions from experimental models

Effects of mechanical stress o On several airway structures o Epithelial cells o Smooth muscle cells o Through various mechanisms o Release of pro-inflammatory cytokines (IL-8) o Neoangiogenesis and globet cell increase o Actin-myosin changes o Potential role in remodelling o Persistent airway obstruction o Progression of the disease

Repeated mechanical stress induces neo -angiogenesis and VEGF production from human airway smooth muscle cells Hasaneen et al, AJPLCMP 2007

Which patient for LABA/LAMA combination ? Singh, B J Clin Pharm 2015

COPD: multiple targets for intervention • Bronchodilators – Effective on airway calibre and hyperinflation – Positive effects on symptoms, exercise tolerance and quality of life – Positive effect on exacerbation rate • LAMA are first choise – Depending on additional findings (nocturnal and early morning symptoms, comorbidities, …) • LABA/LAMA fixed combinations may be used – In alternative to LABA or LAMA, when poorly effective – In more severe patients (MRC >2, FEV 1 <50%)
- Slides: 53