BOWEL INJURY F AlMashat Dep of Surgery Kauh

BOWEL INJURY F. Al-Mashat Dep of Surgery Kauh

TYPES : 1. Blunt 2. Penetrating: Stab, Gunshot 3. Operative

Mechanism: 1. Crushing: Compression 2. Shearing: Sudden Deceleration 3. Bursting: Abdominal Pressure
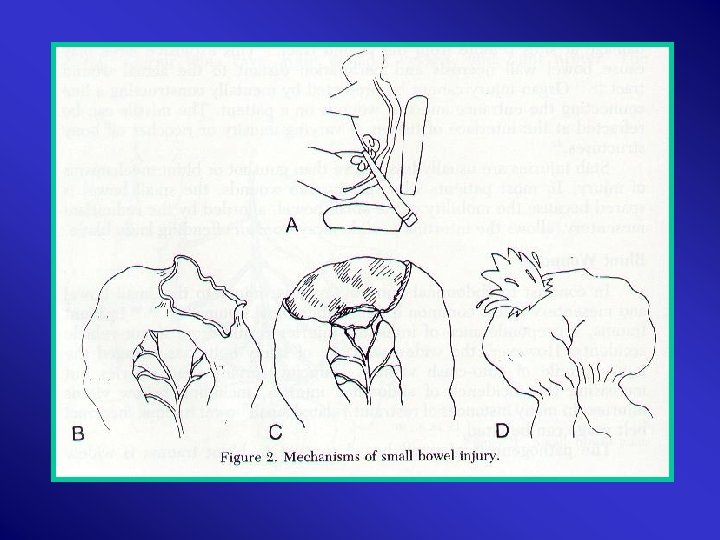

Causes: 1. 2. 3. 4. Motor – Vehicle: 75% High – Speed Vehicular Fall from Heights Seat Belt

Unrecognized : frequent cause of preventable death

Symptoms and Signs: Unreliable Often Masked: 1. Head Injury 2. Major Fractures 3. Alcohol

Signs: 1. 2. 3. 4. 5. 6. 7. Echymosis & Abrasions Tender ribs Peritonitis a. Tenderness and Guarding : 75% b. Rebound and Rigidity: 28% Pelvic Fracture DRE Urethral blood Tests, Perineum , Vagina

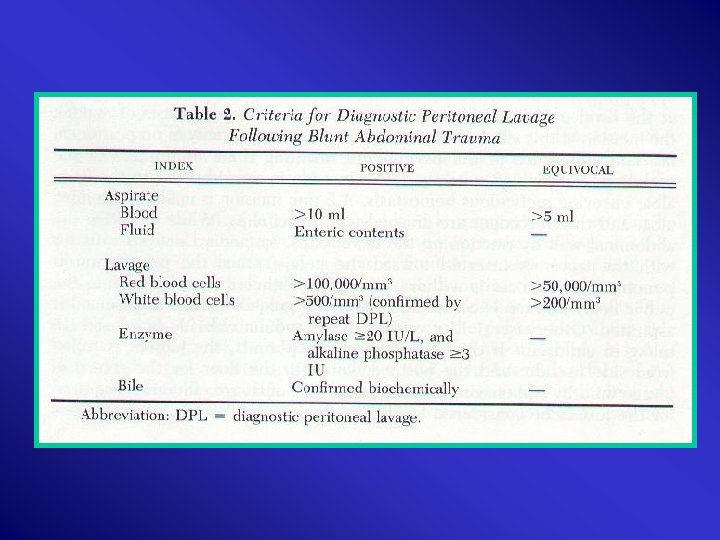
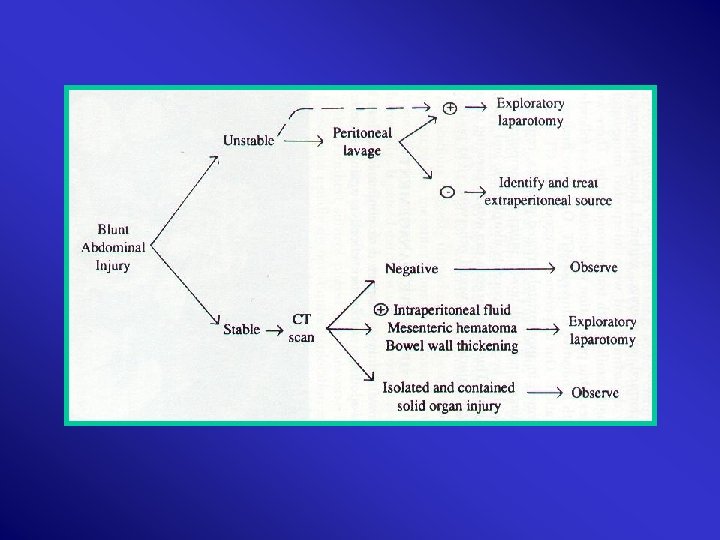
Investigations: 1. CBC 2. U&E’s 3. LFT’s 4. Amylase 5. Clotting Profile 6. ABG 7. Urinalysis 8. CXR : A-P 9. KUB 10. DPL : 95 % Accurate

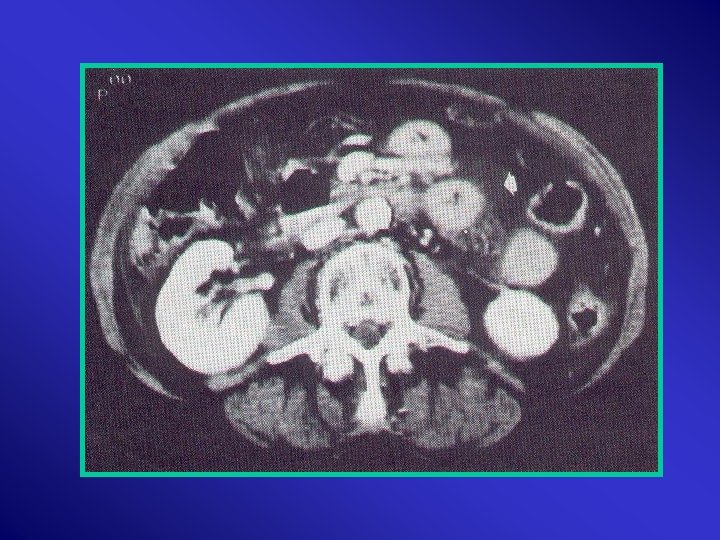
11. Contrast 12. CT 13. U/S 14. IVU /Contrast CT 15. Double – Contrast CT 16. Aortography : Embolization
 The 3 rd in")
Small Bowel Injuries The most frequently involved in penetrating (90%) The 3 rd in blunt Penetrating: Gunshot: > 80% Stab: 30% Occurs in 5 -15% of blunt

Penetrating: 1. History 2. Examination Not Sufficient
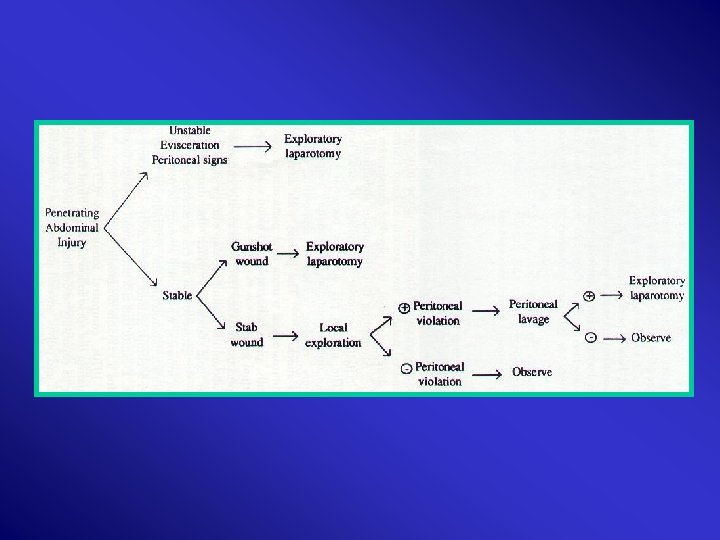

Blunt : “High Index of Suspicion” Physical signs: Non Specific 1. associated injury 2. Alcohol 3. Neutral PH & bacteria – minimal inflammation Delay

Laparotomy: 1. Four: Quadrant Survey 2. Control Enteric Contamination 3. Exploration ? ?

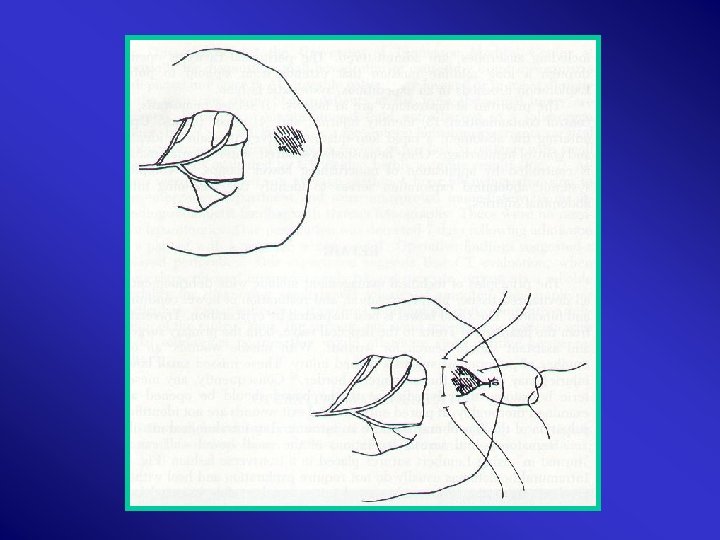
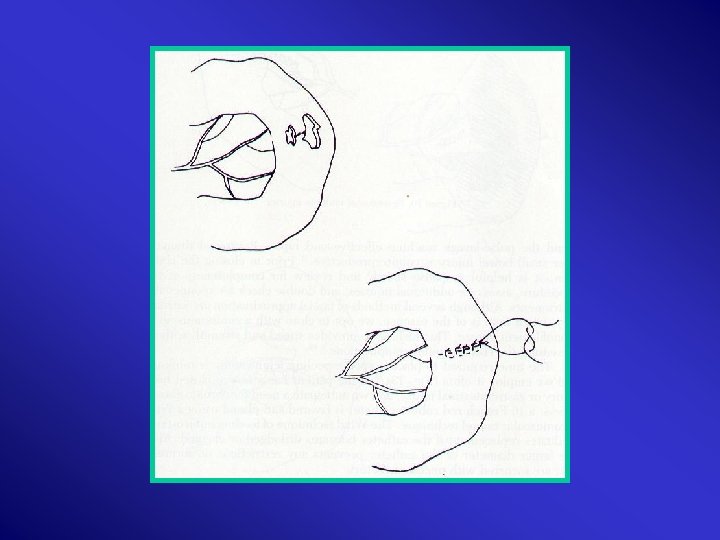
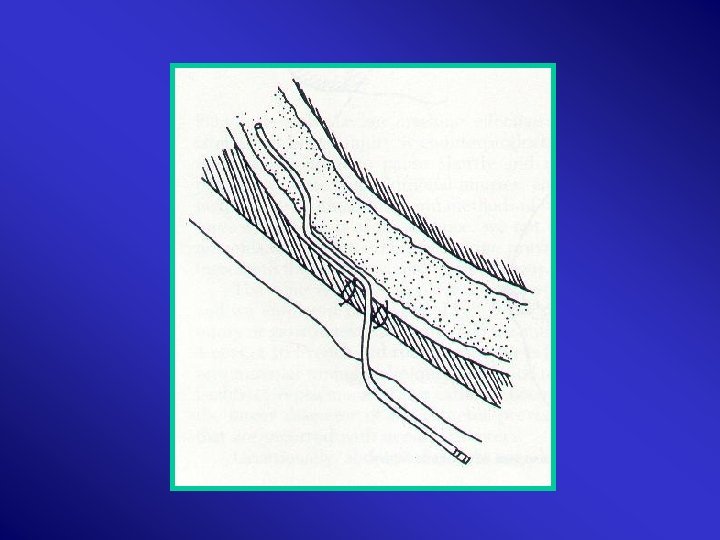
1. Haematoma & Laceration : Lembent, Transverse 2. Mural haematoma <1 cm: Inversion 3. Small perforation : Close transverse 4. Adjacent perforations: divide, close transverse

5. Resection: A. Enterroraphy ½ diameter B. Multiple injuries C. Devascularized Single, Double, Stapler High Bacteria in terminal S. Bowel: repair in a distal to proximal fashion

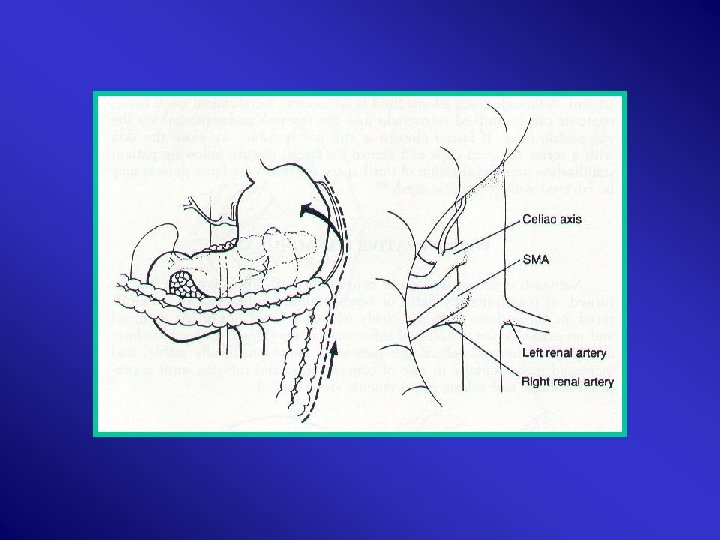
Mesentry Haematoma & Lacerations: >2 cm, expanding, uncontained, near root mesentomy Lesser Sac Proximal Control Root Mesentry Mattox Evacuation Ligation/SMA repair – saphenous vein/ graft Second look 24 H

Injury distal SMA Bowel Resection + Enteroenterostomy

Colon Injuries • Majority: Penetrating • Mortality: < 5%

Risk Factors : • Shock: Sustained hypotension mortality significantly • Duration from injury to surgery morbidity not up to 12 H • Faecal Contamination Quantity ? Major: > one Quadrant Class II & III: Major -- Sepsis

• Associated injuries: Class I, II, & III: > 2 organs -- Sepsis PATI > 25, FSS > 25 , Flint >11 Class I: Greater # of associated organ injury Mortality & Sepsis But : NO Contraindication to 1º repair of non destructive

• Anatomic Location: – Class I , II , & III: NO Significant difference in complications between right & Left for 1º repair • Blood Transfusion: 4 units critical > 4 → ↑ morbidity

Flint Severity Score: • Isolated colon injury, minimal contamination, no shock, minimal delay. • Perforation, lacerations, moderate contamination • Severe tissue loss, devascularization, heavy contamination
 Prospective")
Methods of Repair: Primary Repair: The Standard Safe Right & Left (I, III) Prospective Colostomy : Safe, conservative, acceptable Closure: 10% Morbidity W. Infection I. Obstruction Fistula Incisional Hernia

Exteriorization: a. Healing: 5 – 10 days b. Colostomy Abandoned: Failure & Complications

1. Drains : NO W. Infection Sepsis 2. Peritoneal Irrigation 3. Wound: Definition a: Open: Significant Contamination b: Delayed primary closure: 7 days

Prophylactic Antibiotics 1. Class I & II: Single Pre - OP aerobic & Anaerobic 2. Class I & II: 24 H hollow viscus 3. Shock : dose 2 – 3 folds

Type: Single = Combination Aminoglycocide + Clindamycin or Aminoglycocide + metroindazole Duration: Class I & II: 24 H Optimal Dose: Fluid Shift High Dose Aminoglycocide: 3 mg/Kg Loading
 2. Destructive:")
Recommendations: 1. Class I & II: Non Destructive: 1º repair (Peritonitis º) 2. Destructive: 1º repair if: 1 – Haemodynamic stable 2 – Shock ° 3 – Significant underlying disease º 4 – Minimal associated injuries 5 - Peritonitis º

3. Complex: Shock + substantial contamination or trauma to other organs Resection + proximal diversion Colostomy/ Ileostomy Mucous Fistula Hartmann’s

Pr egnancy 1. Blood Volume 2. Lax Abdominal Muscles 3. Enlarged Uterus 4. Pulse, BP, Haematocril, WBC, HCO 3 5. Compressed Uterus: peripheral venous Pressure 6. GIT motility

Diagnostic Procedures: Same 1. Limit Radiation/ Shielding 2. Avoid Anaesthesia 3. DPL: Open 4. IVU: Single exposure 5. DIC 6. Early Mobilization of fracture
 2. U/S 3. Placental Separation: Fetal")
Special 1. Fetal Heart: Doppler (12 w) 2. U/S 3. Placental Separation: Fetal cells in maternal blood

Treatment: Vigilant Mother must be saved first Options: as non pregnant 1. Uterine Injuries 2. Termination In Majority: non injured uterus – V. Delivery at term Injured uterus – repair

Indicators for C –Section : 1. Uterine rupture 2. Worseness fetal distress 3. Exposure of rectum, great vessels 4. Maternal Thoracolumbar spine fracture 5. DIC 6. MOF

Maternal death Immediate Delivery Poor infant survival if maternal death >15 minutes

THANK YOU
- Slides: 48