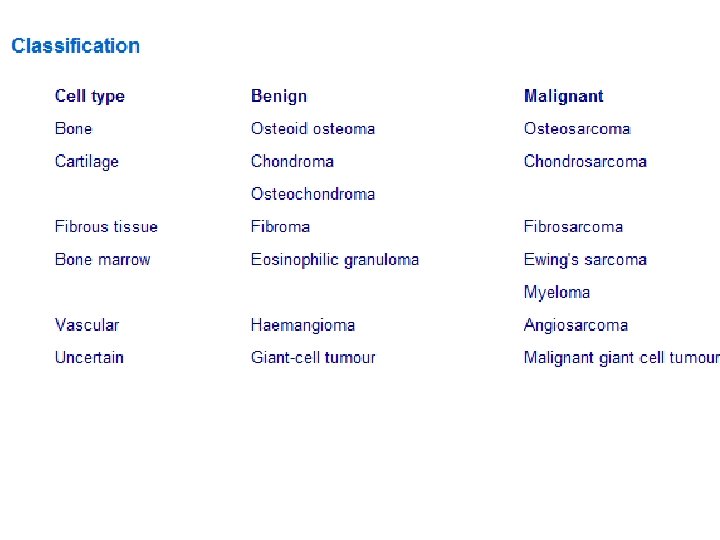
Bone Malignancies Primary bone tumours Primary bone tumours

Bone Malignancies

Primary bone tumours • Primary bone tumours are rare • Secondaries tumours are more common especially in the elderly

Clinical features • Most present with pain, swelling and localised tenderness • Rapid growth and erythema are suggestive of malignancy • May cause pathological fractures • Diagnosis confirmed by: – Plain x-ray – CT scan – Bone scan – Carefully planned biopsy

Osteoid osteoma • Benign bone tumour • Usually less than 1 cm in diameter and surround by dense osteoid • Occurs in young adults • Tibia and femur are the commonest site • Pain (relieved by aspirin) is presenting complaint • Xray has characteristic appearance of a radiolucency surrounded by dense bone • Local excision is curative

Osteochondroma • Commonest bone tumour • Lesions can be single or multiple • Appears in adolescence as cartilaginous overgrowth at epiphyseal plate • Grows with underlying bone • Metaphyses of long bones are the commonest sites • Presents as painless lump or occasionally joint pain • Excision should be considered if causing significant symptoms

Chondroma • Benign tumour of cartilage • Lesions may be single or multiple (Ollier's disease) • Appears in tubular bones of hands and feet • Xray shows well defined osteopenic area in the medulla • Lesion should excised and bone grafted

Osteoclastoma • Equal proportions are benign, locally invasive and metastatic • Found in sub-articular cancellous region of long bones • Only occurs after closure of epiphyses • Patients are usually between 20 and 40 years • Xray shows an asymmetric rarefied area at the end of a long bone • Cortex is thinned or even perforated • Treatment by local excision and grafting often leads to recurrence • Wide excision and joint replacement is the treatment of choice • Amputation if malignant or recurrent tumour

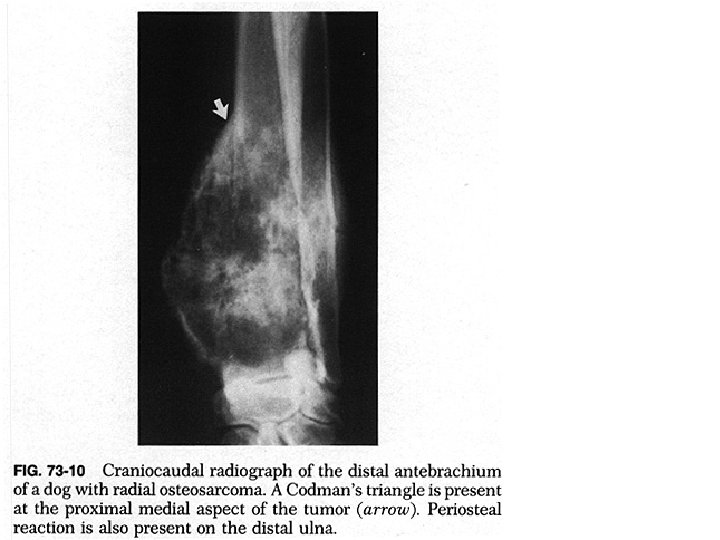
Osteosarcoma • Occurs in the metaphyses of long bones • Commonest sites are around the knee or proximal humerus • Destroys bone and spreads into the surrounding tissue • Rapidly metastasizes to the lung • Usually occurs between 10 and 20 years • In later life is seen associated with Paget's disease • X-ray shows combination of bone destruction and formation
 • Soft tissue calcification produces a")
Osteosarcoma • Periosteum may be lifted (Codman's triangle) • Soft tissue calcification produces a 'sunburst' appearance • Treatment involves amputation and chemotherapy • Amputations are often limited with prosthetic replacement • 50% five years survival • Worst prognosis seen with proximal and axial skeletal lesions


SECONDARY BONE TUMOURS

2 ry bone tumours • 30% of patients with malignant disease will develop bone metastases • 10% of these patients will develop a pathological fracture • Tumours spread to bone by: – Direct invasion – Haematogenous spread – Lymphatic spread – Spread via paravertebral venous plexus • Commonest sites lumbar vertebrae, pelvis and ribs
 Prostate")
1 ry tumours which spread to the bone • • • Breast (35%) Prostate (30%) Bronchus (10%) Kidney (5%) Thyroid (2%) Others (18%)

Clinical features • • Pain or localised bone lump Pathological fracture Hypercalcaemia Cord compression

Radiology • Plain x-rays can be normal • If abnormal will show either an osteolytic or sclerotic lesion

Radiology • Bone scan has higher sensitivity than x-rays • May identify other asymptomatic lesions

DD • • • Calcified enchondroma Hyperparathyroidism Chronic sclerosing osteomyelitis Bone infarct Myeloma deposit

Tx • The aims of treatment are to relieve pain and preserve mobility • If pathological fracture consider internal fixation for early mobilisation and pain relief • Consider radiotherapy for back pain • Spinal decompression may be needed for cord compression • Prophylactic internal fixation may be required if: – Greater than 50% erosion of a long bone cortex – A metastasis of more than 2. 5 cm in diameter – Metastasis in high risk area (e. g. subtrochanteric femur) – Metastasis with persistent pain
- Slides: 20