Bone Joint sepsis Septic Limp Joint swelling R

Bone& Joint sepsis Septic Limp Joint swelling R. F Tumor What antibiotics before culture result? If negative culture? ? What way & how long Surgery Diversity of organism Location Associated conditions

Definition • Osteomyelitis Bone Inflammation Joint • Arthritis BACTERIA Peltola&Vahanen Morey&Peterson But if not?

Pletola&Vahanen Criteria Puss aspiration from bone +Bone or Blood culture Classic symptoms Morey&Peterson DEFINTE: +Cultre from bone or adjacent soft tissue Characteristic histology Probable: +Blood culture& clinical or X-Ray Likely: Typical. Clinic&X Ray+Response to Antibiotics Local pain, Swelling, Warmth&Limited ROM Roentgenography

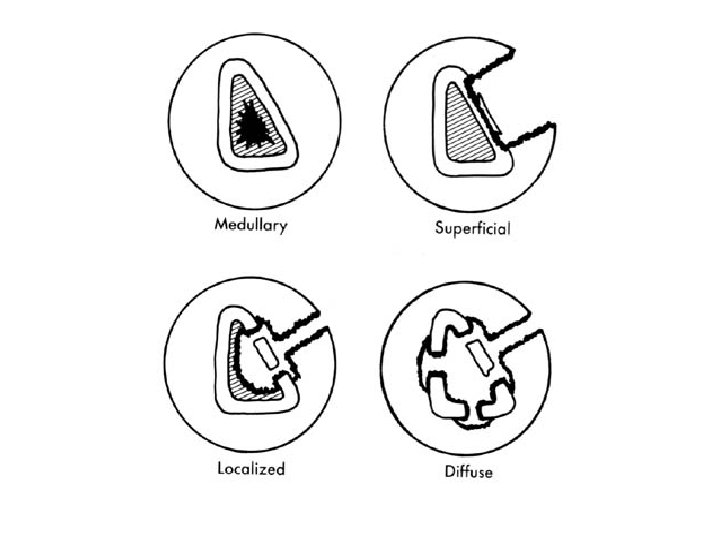
Classification Duration Acute Subacute Chronic: Medullary Superficial Localized Diffuse Mechanism Host response Exogenous Pyogenic Hematogenous Nonpyogenic

Morey T>38. 3 Pain worse with motion Swelling Systematic symptoms No other pathology Response to antibiotics

Epidemiology Childhood 50 Yr. s Early 10 Late 10 s Late summer&Early autumn Older ages M>F Race? KIngella Influenza Kingae Heamophylus 1 -4 Yr. s

Etiology The organism must be identified at the site of the disease KOCH Be identified in the produced disease Not found in other disease Produce the disease in other animals 30%-50%

Predilection for Males Lower extremities Peak age incidence Most rapidly growing ends

Pathophysiology of Osteomelitis Bacteria substrate interacting? Cortical bone 2 types Cancellous bone Turbulence Permeable Less cellular less defense Thick priostem Outside blood supply Involecrum

Before ossific nucleus Consequent growth alteration Nucleus presents Growth plate presents

Osteoblasts death Resorption by Osteoclast 12 -18 hr. Inflammation Bone resorption Few days Probability of septic joint Priosteal reaction Puss in medullary cavity ? Neglected cases Immunity deficiency

Pathophysiology of Septic Arthritis Vasclar Synovium Serum transudate Avascular Joint cartilage No Basement membrane But with defense S. aureus Glycosaminoglycan Some Bacteria Proteases Peptidases Enzymes Collagenases Collagen Live or not 8 hr. Synovitis Fibrinous exudate Synovial necrosis

Septic Arthritis

Pain Position of rest

Lab. Tests • CBC • ESR Not specific 48 hrs, 3 -5 Days, 3 Weeks • CRP 6 hrs, 2 Days, 1 Week

• . Synovial fluid analysis All studies can be performed with only 1 -2 ml. Of fluid. Only a few drops may be adequate for Cx &gram stain Total leukocyte count &Diff Crystal, glucose&proteins Culture & Gram staining Viscosity Gross. Appearance No anticuaguant except a few ml. For cytologic study to which is added 2 mg potassium oxalate per ml. of fluid.

Imaging • X-ray • CT-Scan • Radionuclide scanning

Sequestrum

Identify the organism Select the correct antibiotics Deliver the antibiotics to the organism Stop the tissue distuction Age Neonate(1 -6 weeks) Streptococcus A&B “ “. Pneumaniae E. Coli Staphylococcus aureus Cefotaxime Ceftriaxone HIB Kingella kingae Staphylococcus aureus

Antibiotics • Penicillinase-resistant syntetic penicillin+3 d generation cephalosporin • Vancomycin or clindamycin+3 d generation cephaosporin • Ciprofloxacin+Rifampin in adults & 3 d generation cephalosporin • For Salmonella in adults Fluroquinolon may be added Nafcillin or Ciprofloxacin+Cefriaxon • For post traumatics Nafcillin+ciprofloxacin or. Vancomycin+3 d g, c&Carbencillin Cloaxicillin+Cefizoxime Ciprofloxacin+Refampin+Cefizoxime Vancomycin+Cefizoxime Methycillin+Cefriaxone

Deliver the antibiotics to the organism The course of the disease is resolving I. V or Orally Duration No abcess Well tolerated orally Reliable Parents Penetration Does kill ? 4 -6 weeks +2 -3 additional weeks

Principles of surgery 1 -Incision: Only large enough to expose the area of bone envolved. 2 -Subperiosteal abcess drainage. 3 -Bone drilling: It could be enlarged enough to access B. M. Feel&Appearance dictates NORMALITY

Adequate drainage Antibiotics Rest the joint in stable position

Large joints: Antibiotics&surgery Small joints: Antibiotics Repeated aspiration!!? ? Arthroscopy?
- Slides: 26