Bone disorders Rickets and osteomalacia Dr Somaya Taha

Bone disorders Rickets and osteomalacia Dr. Somaya Taha Saleem

Definition �Defective mineralization of bone due to calcium and vitamin D deficiency, �Rickets affect growing children �osteomalacia affecting adults.
 Lack of sunlight")
Rickets and osteomalacia Causes: • Dietary deficiency (calcium and vitamin D) Lack of sunlight exposure Less common causes include : • Renal disorders (chronic renal failure • Phosphate depletion. • Malabsorption disorders.

Clinical features of rickets • Delayed development • Muscle hypotonia • Bone abnormality

lumbar lordosis and bowing of the legs "rachitic rosary. "

Clinical features of osteomalacia • • Asymptomatic or present with fractures Malaise Proximal muscle weakness Bone and muscle pain and tenderness
D Raised PTH Low or")
Investigations • • • Raised serum alkaline phosphatase Low 25(OH)D Raised PTH Low or normal serum calcium & phosphate X-rays Treatment: Vitamin D supplementation

DISEASES ASSOCIATED WITH DECREASED BONE MASS Osteoporosis : characterized by increased porosity of the skeleton resulting from reduced bone mass. May be localized to a certain bone or region, or may involve the entire skeleton.

Causes of Generalized Osteoporosis: Primary • Postmenopausal • Senile Secondary ENDOCRINE DISORDERS : e. g. • Hyperparathyroidism • Hypo or hyperthyroidism • Pituitary tumors • Diabetes, type 1 GASTROINTESTINAL DISORDERS : e. g. • Malnutrition Malabsorption NEOPLASIA • Multiple myeloma

Pathogenesis: In adults there is a dynamic equilibrium between bone formation by osteoblasts, maintenance by osteocytes, and resorption by osteoclasts. Osteoporosis occurs when the balance tilts in favor of resorption.

Clinical Course : Depends on which bones are involved. Pulmonary embolism and pneumonia are common complications of fractures.
 Osteopetrosis: also")
DISEASES ASSOCIATED WITH DEFECTS IN METABOLIC PATHWAYS (ENZYMES, ION CHANNELS, AND TRANSPORTERS) Osteopetrosis: also known as marble bone disease Group of rare genetic disorders characterized by reduced bone resorption and diffuse symmetric skeletal sclerosis due to impaired formation or function of osteoclasts Manifistations : 1. Fractures. 2. Cranial nerve problems (due to compression from surrounding bone).
 Disease characterized by 3 stages")
DISEASES CAUSED BY OSTEOCLAST DYSFUNCTION Paget Disease (Osteitis Deformans) Disease characterized by 3 stages : 1 - osteolytic stage : repetitive episodes of regional osteoclastic activity and bone resorption 2 - followed by bone formation (mixed osteoclastic-osteoblastic stage), 3 - exhaustion of cellular activity (osteosclerotic stage). The net effect of this process is a gain in bone mass; however, the newly formed bone is disordered and lacks strength.

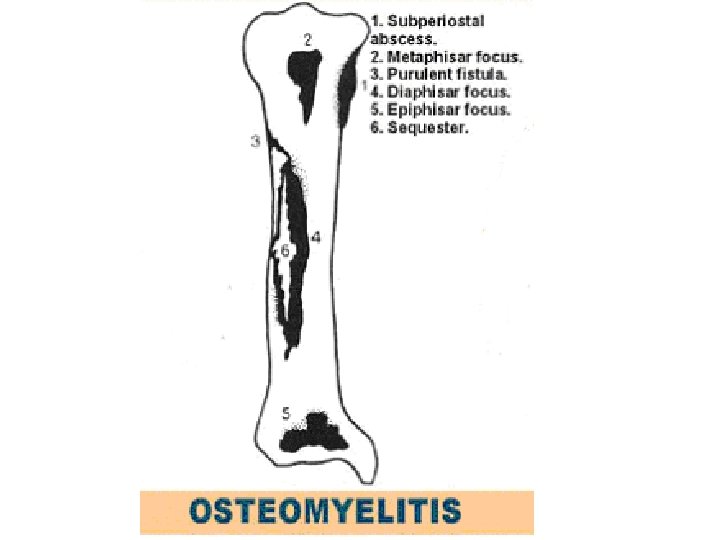
DEFINITION • Definitions : infectious process involving the various component of bone characterized by progressive Inflammatory destruction of the bone, necrosis and new bone formation

Classification Acute and chronic Mechanism of infection – exogenous or hematogenous The type of host response to the infectionpyogenic or non Pyogenic Most common etiologic agents: 1. Pyogenic bacteria 2. Mycobacterium tuberculosis.
 Group")
Organisms Commonly Isolated in Osteomyelitis Based on Patient Age • Infants (<1 year) Group B streptococci Staphylococcus aureus Escherichia coli Children (1 to 16 years) S. aureus Streptococcus pyogenes Haemophilus influenzae Adults (>16 years) Staphylococcus epidermidis S. aureus Pseudomonas aeruginosa Serratia marcescens E. coli • Staphylococcus aureus is the most common cause.

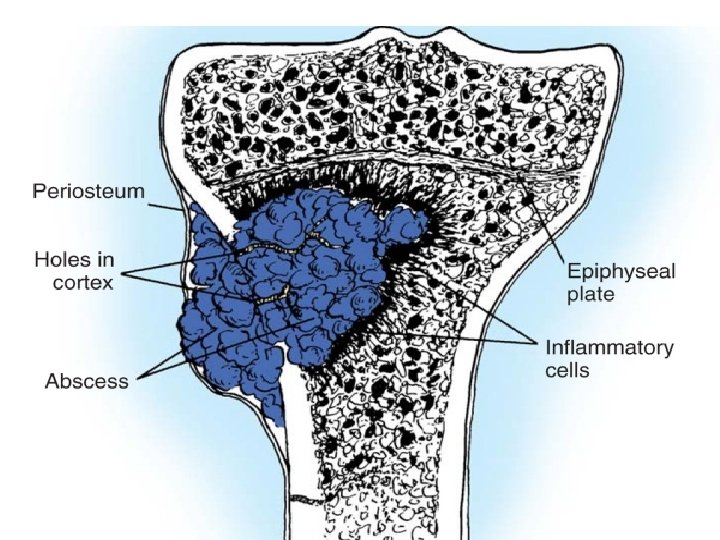
Acute hematogenous osteomyelitis pathology • In children the infection generally involves the metaphyses of rapidly growing long bones • Causal bacteria proliferate, induce an acute inflammatory reaction, and cause cell death. Entrapped bone undergoes early necrosis(called a sequestrum). Bacteria and inflammation reach the periosteum. Subperiosteal abscesses • Rupture of the periosteum can lead to an abscess in the surrounding soft tissue and formation of a draining sinus. • bone formation can be deposited; forms an involucrum.

OSTEOMYELITIS Resected femur in a person with draining osteomyelitis. The drainage tract in the subperiosteal shell of viable new bone (involucrum) reveals the inner native necrotic cortex (sequestrum).

Clinical Features 1. Malaise. 2. Fever. 3. Leukocytosis. 4. Throbbing pain over the affected region.

Diagnosis 1. X Ray 2. Positive Blood cultures. 3. CBC

Complications 1. Pathologic fracture. 2. Secondary amyloidosis. 3. Endocarditis. 4. Sepsis. 5. Development of squamous cell carcinoma in the sinus tract. 6. Rarely osteosarcoma.

Bone tumors Classification • Bone tumors are diverse in their gross and morphologic features and range from benign to rapidly fatal • Most bone tumors are classified according to the normal cell or tissue of origin • matrix-producing and fibrous tumors are the most common. • osteochondroma is the most common benign tumors, • osteosarcoma is the most common primary cancer of bone.
 Morphology Facial bones, skull 40 -50 Exophytic growths")
Tumor Type Common Locations Age (yr) Morphology Facial bones, skull 40 -50 Exophytic growths attached to bone surface; histologically resemble normal bone Osteoid osteoma Metaphysis of femur and 10 -20 tibia Cortical tumors, characterized by pain; histologically interlacing trabeculae of woven bone Osteoblastoma Bone-Forming: BENIGN Osteoma Vertebral column 10 -20 Arise in vertebral transverse and spinous processes; histologically similar to osteoid osteoma Primary osteosarcoma Metaphysis of distal femur, proximal tibia, and humerus 10 -20 Grow outward, lifting periosteum, and inward to the medullary cavity; microscopically malignant cells form osteoid; cartilage may also be present Secondary osteosarcoma Femur, humerus, pelvis >40 Complications of polyostotic Paget disease; histologically similar to primary osteosarcoma MALIGNANT

Cartilaginous: BENIGN Osteochondroma Metaphysis of long tubular bones 10 -30 Bony excrescences with a cartilaginous cap; may be solitary or multiple and hereditary Chondroma Small bones of hands and feet 30 -50 Well-circumscribed single tumors resembling normal cartilage; arise with medullary cavity of bone; uncommonly multiple and hereditary Bones of shoulder, pelvis, proximal femur, and ribs 40 -60 Arise within medullary cavity and erode cortex; microscopically well differentiated cartilage-like or anaplastic Giant-cell tumor (usually benign) Epiphysis of long bone 20 -40 Lytic lesions that erode cortex; microscopically, contain osteoclast-like giant cells and round to spindle-shaped mononuclear cells; majority are benign Ewing tumor (malignant) Diaphysis and metaphysis 10 -20 Arise in medullary cavity; microscopically, sheets of small round cells that contain glycogen; aggressive neoplasm MALIGNANT Chondrosarcoma Miscellaneous

Clinical presentation: • asymptomatic. • pain • slow-growing mass. • pathologic fracture. Diagnosis: • Clinical • Radiography • biopsy

Osteosarcoma: Is a bone-producing malignant mesenchymal tumor. primary : Osteosarcomas occur in all age groups but 75% of patients are younger than age 20, Secondary ( in the elderly), to Paget disease, bone infarcts, and prior irradiation.

Clinical Features: 1. painful enlarging masses. 2. pathologic fracture. 3. Radiographs usually show a large, destructive, mixed lytic and blastic mass A triangular shadow on x-ray between the cortex and raised periosteum (Codman triangle) is characteristic of osteosarcomas.

Osteosarcoma

• Thank you
- Slides: 31