BONE DISEASES 1 Dr Hani Al Sheikh Radhi

BONE DISEASES 1 Dr. Hani Al Sheikh Radhi
")
Types of Bone Intramembranous Endochondral (epiphyseal bone)
). cells change into bone immediately")
Intramembranous Small bones Immediately from Mesynchymal cells (Mesynchymal (osteocytes)). cells change into bone immediately
 Long bones Intermediate cartilage formation")
Endochondral (epiphyseal) Long bones Intermediate cartilage formation

 Defect in the Endochondral bone formation. Mutation in FGFR 3 gene. Mid-")
Achondroplasia (Dwarfism) Defect in the Endochondral bone formation. Mutation in FGFR 3 gene. Mid- face forms by epiphyseal while the rest is intermembranous. Defect in fibroblast growth factor which will affect cartilage.


Posterior cross bite. Anterior open bite. Class III malocclusion

Associated features Macroglossia and tongue thrust. Increase caries rate No disturbance in eruption dates Backache due to spine stenosis in some patients form late childhood until early adolescence



Management Psychological therapy Lower dental chair with the need of steps sometimes Back and head pillow for children to reduce discomfort associated with backache

Bone Remodeling
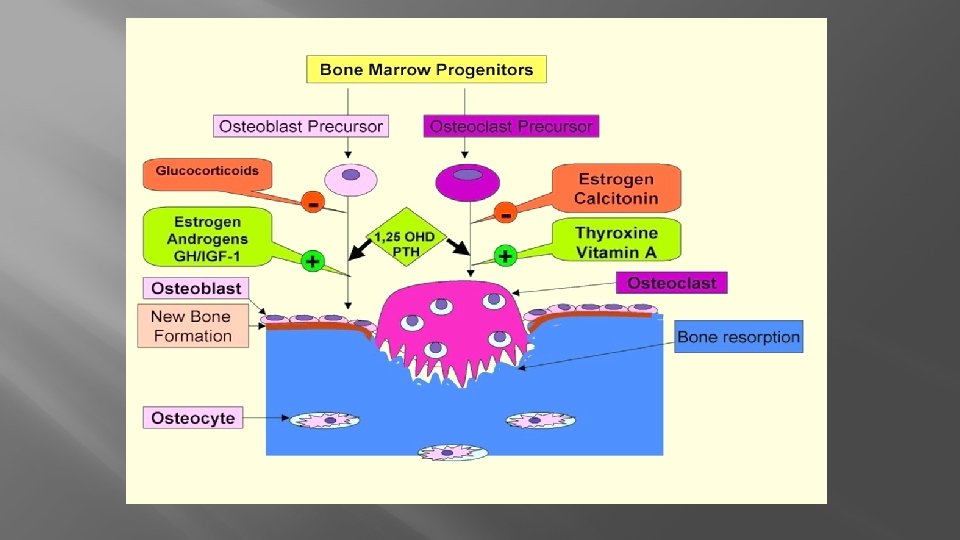

Factors affecting bone remodeling PTH Vit. D Collagenases Lysosome Cytokines Prostaglandins BMP

Inhibitors of Bone remodeling Calcitonin Interferon Bisphontae Cortisol

Brown Tumor of Hyperparathyroidism Increased PTH conc. Can increase the activity of osteoclasts a which will increase bone resorption.

Giant cell granuloma CGCG due to action of osteoclasts, not related to PTH Although histologically identical to brown’s tumor differentiated by investigations of PTH conc. And alkaline phosphatase. The World Health Organization has defined CGCG as an intraosseous lesion consisting of cellular fibrous tissue containing multiple foci of hemorrhage, aggregations of multinucleated giant cells and, occasionally, trabeculae of woven bone. Can be mild and asymptomatic or it can be aggressive and painful and it can perforate the cortical plates.


Treatment and Prognosis For central lesions: Conservative but complete surgical resection is the preferred treatment. Radiation treatment generally not indicated Recurrence rates vary and reported from 11% to near 50%

Treatment and Prognosis For peripheral lesions: Conservative but complete surgical resection to include the entire depth of the lesion with curettage of subjacent bone. May recur in a small percentage of cases (approximately 10%)

Bisphonate Induced Osteochemonecrosis Bisphonate used to be commonly administered to control bone resorption conditions caused due to over activity of osteoclasts

Osteoradionecrosis

Osteopetrosis Alber-Schonberg Disease

Osteopetrosis Osteoclasts malfunction. Normal osteoblasts. 2 types: Infantile: at birth. Severe cranial nerve problems, almost all bones, anemia (bone marrow), osteomyelitis, delayed eruption and ankylosis. Adult (Benign osteopetrosis) long bone rarely affected, less problems 40% discovered by routine examination


• Difficult to distinguish roots from bone. • ankylosis delayed eruption of teeth. • risk of osteomyelitis with extraction due to poor blood supply of bone
 • Osteomyelitis management is")
Management 2 PROBLEMS (bone marrow failure, and increased bone density) • Osteomyelitis management is difficult. • Bone marrow transplantation to improve cellularity.
- Slides: 28