BONE AND JOINT INFECTIONS BONE AND JOINT INFECTIONS

BONE AND JOINT INFECTIONS
 NON-SPECIFIC IN")
BONE AND JOINT INFECTIONS EXOGENOUS OPEN FRACTURES POST-OPERATIVE HAEMATOGENOUS SPECIFIC( TB, …) NON-SPECIFIC IN BONES OSTEOMYELITIS (OM) IN JOINTS SYNOVITIS … ARTHRITIS

ACUTE HEMATOGENOUS OSTEOMYELITIS

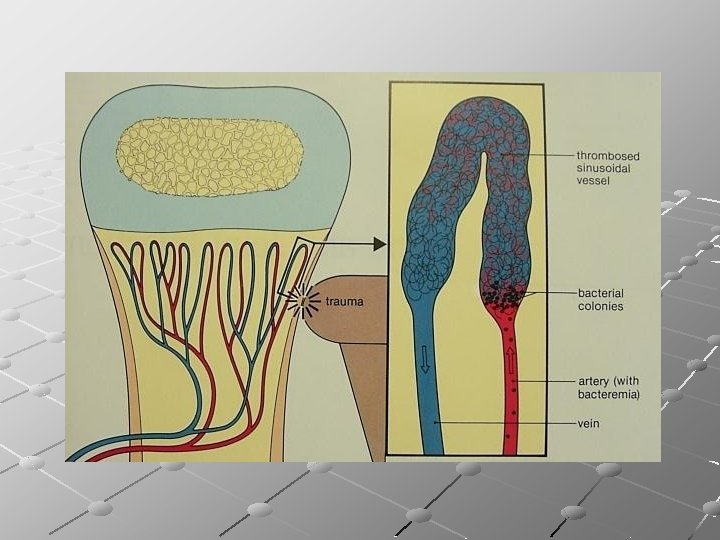
ACUTE HEMATOGENOUS OSTEOMYELITIS Age group: Acute hematogenous osteomyelitis is almost a disease of children. When adults are affected it is usually because of defective immunity by debility, disease or drugs, e. g. Diabetes mellitus, AIDS, …. Trauma may determine the site of infection , possibly by causing a fluid collection or a small hematoma
Staph aureus…. Most common 2)Strept pyogenes 3)Strept pneumonaie 4)Haemophilus influenzae(5 -50% in")
Causative organisms: 1)Staph aureus…. Most common 2)Strept pyogenes 3)Strept pneumonaie 4)Haemophilus influenzae(5 -50% in children under 4 years) 5)Salmonella (common in patients with Sickle cell anaemia) 6)Others ; gram negative and anaerobic organisms) Source and Route of infection: In children, blood stream may be invaded from a minor skin abrasion, boil, a septic tooth or infected umbilical cord. In adults entry could be through an indwelling catheter, arterial line or contaminated syringe.

Sites of infection: Usually in the metaphysis, mostly in proximal tibia or distal and proximal ends of femur. This predilection to the metaphysis is due to its peculiar vascular pattern: the non- ananstmosing terminal branches of the nutrient artery twist back in hair –pin loops before entering the sinusoidal veins causing relative vascular stasis. In adults, hematogemous infection is more common in vertebrae than in long bones.

PATHOLOGIC STAGES OF OSTEOMYELITISM *ACUTE *SUBACUTE *CHRONIC
Inflammation 2)Suppuration : Intra-osseous abscess Sub-periosteal abscess 3)Resolution(with ttt) or Subacute")
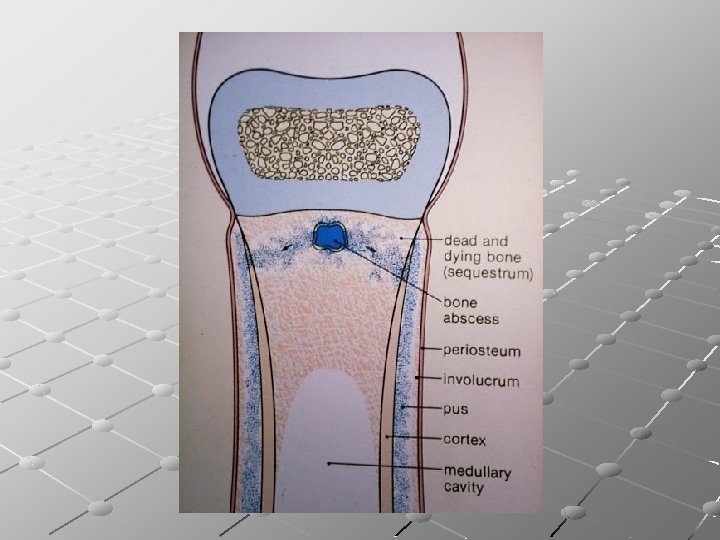
Pathology : ACUTE 1)Inflammation 2)Suppuration : Intra-osseous abscess Sub-periosteal abscess 3)Resolution(with ttt) or Subacute CHRONIC 1)Bone necrosis Sequestrum 2)New bone formation Involucrum 3)Cavity, discharging sinus Cloaca

Clinical picture of acute OM: General : Typically the child looks ill feverish. Pulse>100 Infants fail to thrive, drowsy but irritable. In neglected cases, toxemia may be marked. Local : The limb is held still(Pseudo-paralysis) there is acute tenderness near a major joint; joint movement becomes restricted. Local swelling and redness are late signs and indicate that pus escaped from the interior of the bone.

Diagnostic imaging: Plain X-ray - Shows no abnormality of the bone before the second week - After 2 weeks, there may be a faint extra cortical line due to periosteal new bone formation. - An important late sign is a combination of regional osteoporosis with a localized segment of increased density. U. S: - may detect subperiosteal collection but cannot differntiate between pus and hematoma MRI - is extremely sensitive even in the early phases of bone infection RADIOACTIVE ISOTOPE SCAN - sensitive even in the early phases of bone infection Hot spot
The most certain way is to aspirate pus from the metaphyseal subperiosteal abscess")
Investigations: 1)The most certain way is to aspirate pus from the metaphyseal subperiosteal abscess or adjacent joint 2)Elevated WBC count, C reactive protein and ESR 3)Blood culture: +ve in 50% of cases N. B: osteomyelitis in an unusual site or unusual organism should alert to the possibility of heroin addiction, deficient immunity or sickle cell anaemia.
Cellulitis. 2) Acute suppurative arthritis. 3) Acute rheumatic arthritis. 4) Sickle cell")
Differential diagnosis: 1)Cellulitis. 2) Acute suppurative arthritis. 3) Acute rheumatic arthritis. 4) Sickle cell crisis. 5) Streptococcal necrotizing myositis.

Treatment : Once osteomyelitis is suspected, blood and fluid samples should be taken, then treatment is started immediately before confirmation of the diagnosis. Patient should be admitted to hospital 1)Supportive treatment: Antipyretics –analgesics 2)Splintage : Rest – prevent joint contracture 3)Antibiotics : Start imperically then according to lab investigations. Start with parentral (I. V. ) treatment till CRP returns to normal values, then continue oral therapy for 3 -6 weeks 4)Drainage : If clinical features don’t improve within 36 hours of starting treatment or even earlier if there are signs of deep pus (rednesshotness-swelling)

Follow-up Once signs of inflammation subside, movements are encouraged. Full weight bearing is possible after 3 -4 weeks.
Metastatic infection: Involving others bones, joints, serous cavities, brain or lung. 2)Suppurative")
Complications : 1)Metastatic infection: Involving others bones, joints, serous cavities, brain or lung. 2)Suppurative arthritis: A-In young patients before closure of the epiphysis B-Intracapsular metaphysis; e. g. head of femur C-Metastatic infection 3)Altered bone growth: In infants with physeal damage 4)Chronic osteomyelitis: In neglected cases or immune-compromised patients.

Subacute hematogenous osteomyelitis Age : Usually childhood and adolescence. Pathology : - Common sites include metaphyseal areas of distal femur and proximal and distal tibia. -There is a well defined cavity in the cancellous bone, containing sero-purulent fluid (rarely pus). -The cavity is lined by granulation tissue containing a mixture of acute and chronic inflammatory cells. -The surrounding bone trabeculae are often thickened.

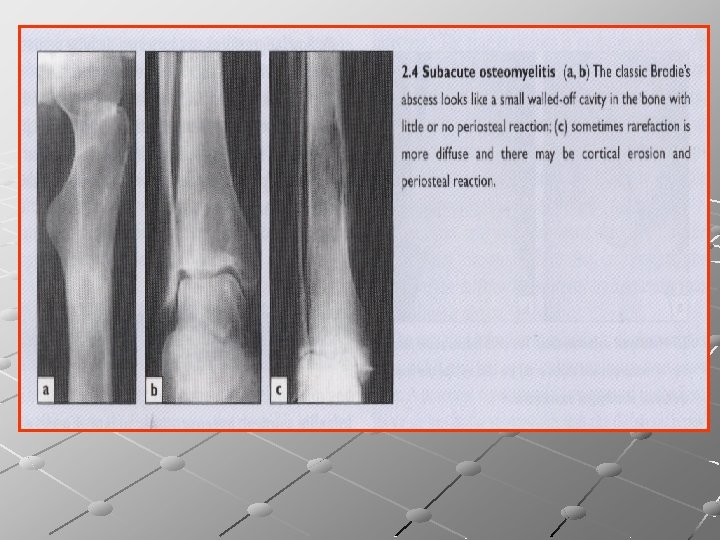
Clinical picture: Patient complains of pain near one of the big joints for several weeks. There may be a limp, slight swelling, muscle wasting and local tenderness. Patient may present with pathological fracture Imaging : Well circumscribed round or oval cavity, 1 -2 cm in diameter. Sometimes surrounded by a halo of sclerosis [Brodie’s abscess]; Metaphyseal lesions cause little or no periosteal reaction , yet diaphyseal lesions may be associated with periosteal reaction and marked cortical thickening

Investigations : WBC count may be normal, but ESR and CRP are often elevated. Treatment : Immobilization and antibiotics for 6 weeks. If diagnosis is doubtful or there is no response to conservative treatment , open biopsy and curettage is done, followed by a further course of antibiotics.

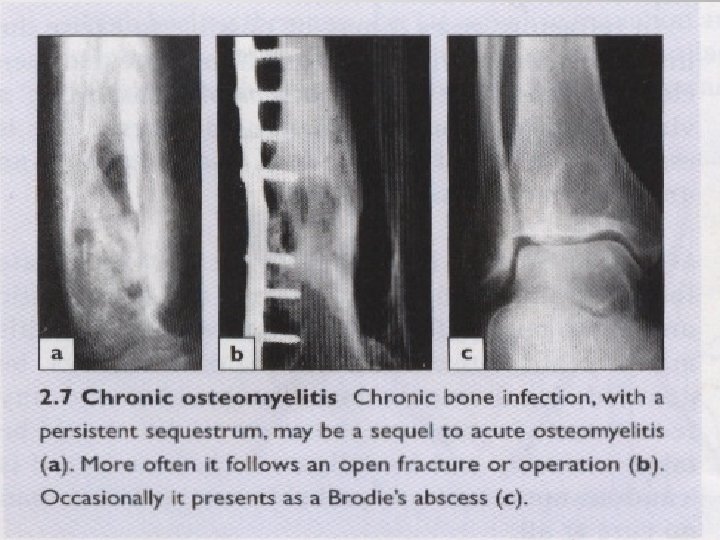
Chronic osteomyelitis Used to be a dreaded sequel to acute hematogenous osteomyelitis, nowadays more frequently follows an open fracture or operation. Causative organisms: 1)Staph aureus. 2)E coli. 3)Strept pyogenes. 4)Proteus. 5)Pseudomonas. 6)Strept epidermidis (esp. with implants)

Pathology: Affected bone is destroyed or devitalized with cavities containing pus and pieces of dead bone (sequestrum), surrounded by vascular tissue, and beyond that by areas of sclerosis. Sequestra act as substrates for bacterial adhesion causing persistence of the infection until removed or discharged through draining sinuses. Sinuses may close spontaneously then reopen when tissue tension rises. Pathological fracture may develop. • New bone formation Involucrum • Bone necrosis Sequestrum • Cavity, discharging sinus Cloaca

Clinical picture: - Patient may present with pain, pyrexia, redness and tenderness. - There may be a discharging sinus. - In long standing cases, tissues are thickened and even folded in, where a scar or sinus is attached to the underlying bone. - There may be seropurulent discharge and excoriation of the surrounding skin. - Patient may present with pathological fracture.

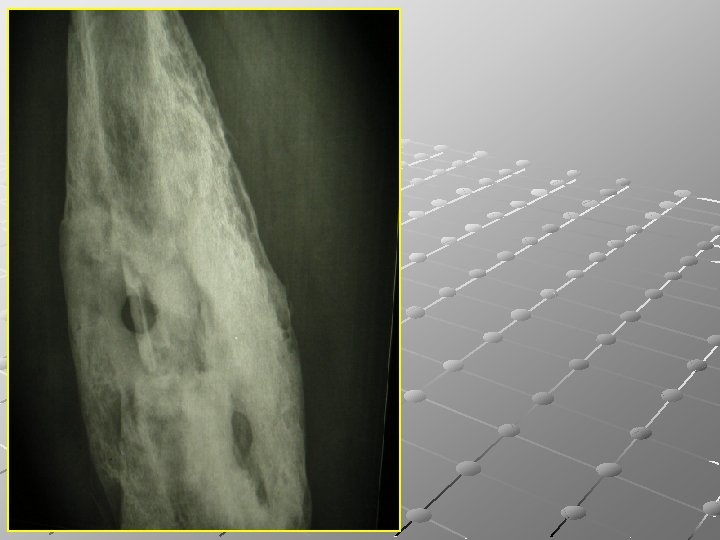
Imaging : X-ray shows bone resorption with thickening and sclerosis of the surrounding bone. Sequestra seen as unnaturally dense fragments in contrast with the surrounding vascularized bone. Sometimes the bone is crudely thickened and misshapen resembling a bone tumour, involucrum. Involucrum Sequestrum



Imaging : CT and MRI are invaluable in planning operative treatment, showing extent of bone destruction, reactive edema, hidden abscesses, and sequestra. Bone scan is sensitive but not specific.

Investigations : ESR , CRP and WBC count are elevated in acute flares. Organisms cultured from the discharging sinuses should be tested repeatedly for antibiotic sensitivity.

. Treatment : Antibiotics : seldom eradicate infection alone, yet given to prevent local spread of the infection and to control acute flares(C&S to be done). Operative treatment: saucerization & sequestrectomy. External fixator may be appliied to avoid fracture In refractory cases it may possible to excise the infected segment and perform segment transfer using Ilizarov technique.


JOINT INFECTION PATHOLOGIC STAGES OF JOINT INFECTION *ACUTE : SYNOVITIS ARTHRITIS *CHRONIC SYNOVITIS ARTHRITIS

CLINICAL PRESENTATION OF JOINT INFECTION *ACUTE : SYNOVITIS ARTHRITIS *CHRONIC SYNOVITIS ARTHRITIS

ASPIRATION

Septic Arthritis Aetiology: Organisms: S. aureus, streptococcus or E. coli in adults and H. influenza in infants. Route of infection: either haematogenous spread or direct spread from penetrating wound, injection or after surgery or from adjacent osteomyelitis. P. F. : septic focus, trauma, R. A. and immunocompromised patient.

Pathology of Septic Arthritis Synovitis; serous, then seropurulent, then purulent exudates. Joint subluxation and/or dislocation. Progressive damage of articular cartilage. Destruction of bony ends with reactive new bone formation later. Fibrous or bony ankylosis.

Diagnosis Symptoms: fever, pain, inability to move the joint or weight bear. Signs: high fever, tachycardia, tenderness, deformity and loss of all passive and active movement. Discharging sinus in late cases. Laboratory: leukocytosis, elevated ESR and CRP.

Diagnosis Radiology: X-ray: irregular and reduced joint space, sclerosis of subchondral bone, bony destruction, subluxation or dislocation and finally bony ankylosis. U. S. : to detect amount and type of fluid. Aspiration: to obtain fluid for culture and sensetivity.

Differential Diagnosis Trauma. Rheumatic fever. Gout. Acute osteomyelitis. T. B. arthritis.


INVESTIGATIONS OF JOINT INFECTION *ACUTE : SYNOVITIS ARTHRITIS *CHRONIC SYNOVITIS ARTHRITIS LAB TESTS RADIOGRAPHY SONOGRAPHY SCIETIGRAPHY PARACETHESIS(Aspiration)
. Supportive treatment. Antibiotics for 4 weeks starting")
Treatment Rest and immobilization (traction or spica). Supportive treatment. Antibiotics for 4 weeks starting with I. V. antibiotics for 5 -7 days. Surgical drainage must be done early to save the articular cartilage and may be done by arthroscopy or arthrotomy. Arthrodesis may be required to achieve fusion in the position of function.

TREATMENT OF JOINT INFECTION *ACUTE : SYNOVITIS ASPIRATION ARTHRITIS ARTHROTOMY *CHRONIC SYNOVECTOMY EXCISIONSYNOVITIS ARTHROPLASTY ARTHRITIS ARTHRODESIS(FUSION)

CHRONIC SPECIFIC INFECTIONS

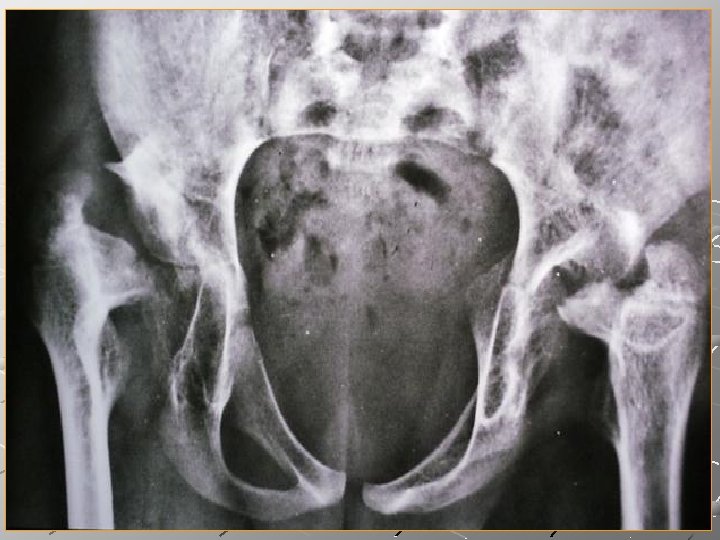
Tuberculosis of The Hip Joint Aetiology: Always secondary T. B. Organism: mycobacterium T. B. Predisposing factor: poor nutrition and health conditions, D. M. , and immuno-compromise.
: focus at upper part")
Pathology of T. B. of the hip Osseous type (common): focus at upper part of the acetabulum or inferior part of the head of the femur (Babcok’s triangle). Synovial type (rare): granulation tissue causes hypertrophy of synovial membrane followed by destruction of articular cartilage. Wandering acetabulum and path. dislocation. Cold abscess formation.

. Pathology: Usually starts in the vertebral body")
T. B. of the Spine (Pott’s Disease). Pathology: Usually starts in the vertebral body and very rarely in the vertebral arch. Vertebral body is destroyed and replaced by necrotic caseous material. Early involvement of the disc and adjacent vertebra leading to kyphosis and cold abscess formation. Paraplegia may develop due to cord compression.
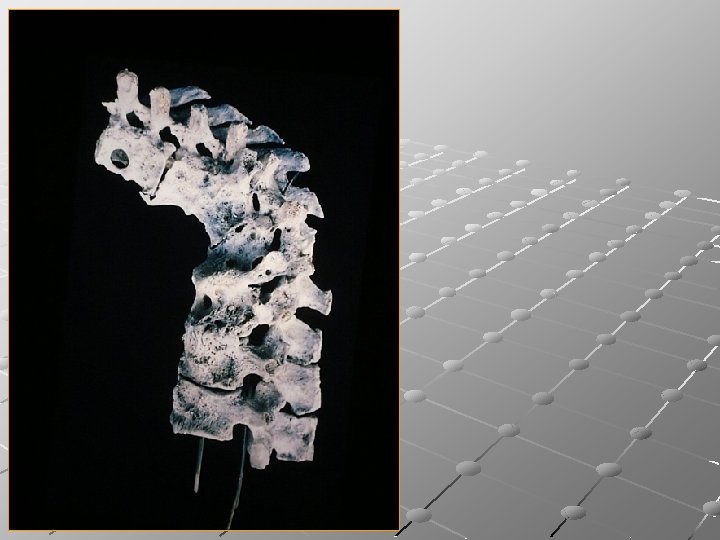

Diagnosis Tuberculous toxaemia and weakness. Pain local or reffered. Tenderness. Angular kyphus deformity Limited movements of te spine. Cold abscess formation (psoas abscess). Varying degrees of neurological deficit.

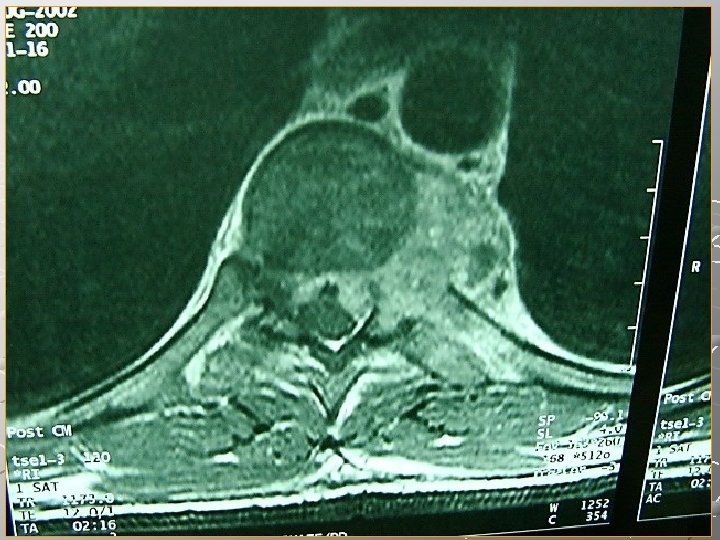

Pott’s Paraplegia Occurs in about 10% of cases. It may result from compression of the thoracic spine due to, cold abscess formation, granulation tissue, inflammatory oedema, progressive kyphus deformity, and thrombosis of vessels of the cord. It is usually spastic and it may progress to be flaccid at the end.

- Slides: 57