Body Fluids Balance MOHAMED O EZWAIE MD ASSOCIATE

Body Fluids Balance MOHAMED O. EZWAIE, MD ASSOCIATE PROFESSOR OF MEDICINE AND NEPHROLOGY

Learning objectives/ lecture agenda Importance of fluid homeostasis Basic hemodynamic principles Regulation of sodium balance (ECF volume) Body fluid distribution Clinical evaluation of hydration status Diuretics clinical use & adverse effects Body response to hypovolemia Principles of fluid therapy
 Maintaining normal volume and composition of the body fluids is vital")
Fluid homeostasis (balance) Maintaining normal volume and composition of the body fluids is vital to life Correct fluid and electrolyte balance is essential to maintain normal physiological function; tissue perfusion, metabolism and enzymatic reactions

Fluid balance Hospitalized patients may not be able to eat and drink normally and often have depleted fluid and/or electrolyte levels. It is important to distinguish between fluid and electrolytes required for normal existence (daily maintenance) and for resuscitation or replacement of abnormal losses Intravenous provision of fluid and electrolytes is therefore often needed to maintain or restore balance.
 Homeostasis: Fluid balance Electrolyte balance Osmotic balance Acid-base balance")
Fluid homeostasis (balance) Homeostasis: Fluid balance Electrolyte balance Osmotic balance Acid-base balance

Basic hemodynamic principles Blood volume distribution; divided between five circulatory beds and pools Capillary bed 7% Venous pool ( capacitance ) 64% Pulmonary bed 9% Heart pool 7% Arterial bed ( effective arterial blood volume) 13%
")
Basic principles Major determinant of ECF volume; is ECF Na content ( sodium balance) Major determinant of blood volume distribution between arterial and venous circulation, is efficiency of cardiac contractility Major determinant of plasma volume; is plasma oncotic pressure Major determinant of ICF volume/ hydration: is ECF tonicity (water balance)
 Facts/ concepts in nephrology to realize; Control of")
Regulation of sodium balance (ECF volume) Facts/ concepts in nephrology to realize; Control of ECF volume is dependent on regulation of sodium balance (intake and excretion), clinically manifested as: Hypovolemia/ hypotension Hypervolemia-edema/ hypertension ECF volume disorder Control of sodium concentration is dependent on regulation of water balance, clinically manifest as: Hyopnatremia Hypernatremia ECF / ICF osmolality disorder
 Sensor Stimulus Effector Baroreceptors Reduced tissue perfusion; -")
Regulators of sodium balance (ECF volume) Sensor Stimulus Effector Baroreceptors Reduced tissue perfusion; - Hypovolemia; - Hypervolemia (apparent) Sympathetic nervous system ANP Non-osmotic release of ADH (intra-vascular arterial receptors) - Low pressure; atria - High pressure; carotids and aortic arch Nephron; Juxtaglomerular appartus (JGA) with↓EABV; CCF ( reduced cardiac output), liver cirrhosis (systemic vasodilation) Nephron tubules; Arterial blood Renal tubules Sodium pressure, tubular handling in PCT, loop sodium load of Henle. EABV: effective arterial blood volume CCF: congestive cardiac failure ANP: atrial natriuretic peptide ADH: antidiuretic hormone RAAS: renin-angiotensin-aldosteron system: CCD: cortical collecting ducts Balance effect Salt and water retention or excretion RAAS: mineralocorticoids effect on DCT & CCD Pressure natriuresis at PCT, and loop Na-K 2 Cl cotransporter
 70 kg man has ~42 L")
Body fluid distribution total body water ( TBW) 70 kg man has ~42 L (%60) of body weight In females 50% if body weight In infants water accounts for >70% body weight. Distribution of fluid in the body : 1/3 in extracellular fluid ( 14 L, 20% BW) Interstitial fluid 10 L ( 25% of TBW) Plasma 3 L ( 7% of TBW) Transcellular fluid 1 L ( 1 -2% of TBW) 2/3 in intracellular fluid ( 28 L, 40% BW) Red blood cells 2 L Other cells 26 L
 Transcellular fluids third space, include cerebrospinal")
Body fluid distribution total body water ( TBW) Transcellular fluids third space, include cerebrospinal fluid, synovial fluid, pleural fluid, ocular fluid, etc. Blood volume in adult about 7% of body wt. in males cellular elements 40% and plasma 60%, in females hematocrit is 35%, while plasma is 65% Fluid movement between these compartments are governed by osmotic and Starling forces

Fluid and electrolyte requirements Daily requirements Water: 35 -40 ml/kg/day, average 70 kg adult 2. 5 -3. 0 liters per day Insensible water losses; male 15 ml/kg/day, females 10 ml/kg/day Sodium ~ 100 -150 m. Eq Potassium ~60 -80 m. Eq Minimum urine volume 0. 5 -1. 0 ml/ kg/ hour Oliguria; urine output < 0. 5 ml/kg/hour Anuria; urine output < 100 ml/ day

Fluid and electrolyte requirments Daily fluid balance of 70 kg man: Intake: ~2500 ml 1500 ml – liquid intake 750 ml – food 250 ml – oxidative phosphorylation Output: ~ 2500 ml 1500 ml – urine* 100 ml – feces 900 ml – insensible loss (skin, lungs) * Minimal volume of urine a healthy person needs to produce is 0. 5 – 1 ml/kg/hr

Assessment of fluid balance; conservative methods In most cases fluid requirements have to be assessed and monitored using the usual clinical approach of history, clinical examination and investigations No symptom or sign is pathognomonic in isolation so that a proper assessment can only be made using a combination of different variables interpreted in the light of the underlying pathophysiology

Assessment of fluid balance; invasive methods The gold standard for volume replacement is invasive cardiac monitoring, especially in high dependency patients With the availability of minimally invasive techniques for measurement of stroke volume and cardiac index, using trans-oesophageal, or using central venous pressure ( CVP) as a rough guide
: Is a measure of adequacy")
Assessment of fluid balance Central venous pressure ( CVP): Is a measure of adequacy of venous vascular volume and right ventricular filling pressure Surrogate marker of ECF volume state, and fluid therapy can be adjusted according to its level Normal range: 6 -8 cm. H 2 O or 4 -6 mm. Hg 1 cm. H 2 O = 0. 74 mm. Hg 1 mm. Hg = 1. 36 cm. H 2 O

Assessing volume status History: Patient history, observation and fluid charts, patient notes, etc. Examination: Blood pressure, pulse, body weight, skin turgor and capillary refilll time Investigations: urine output, central venous pressure readings, blood tests, chest x-ray Response to fluid challenge: Give a 0. 5 - 1 liter 0. 9% saline or 250 ml colloid through large bore 14 G (brown) or 16 G (grey) cannula over 30 -60 minutes. Measure response: CVP monitoring, BP, or resumption of urine output. Repeat as necessary. Fluid challenge is safe if lungs are clear.

Signs of hypo / hypervolaemia: Volume depletion Signs of … Volume overload Postural hypotension Hypertension Tachycardia Absence of JVP @ 45 o Raised JVP / gallop rhythm Decreased skin turgor Oedema Dry mucosae Pleural effusions Supine hypotension Pulmonary oedema Oliguria Ascites
 �Palpable swelling produced by expansion of the interstitial fluid volume �The")
Volume overload (edema) �Palpable swelling produced by expansion of the interstitial fluid volume �The expansion takes several liters ( 2 -3 L ) before overt manifestations of edema (i. e. weight gain of several kg. ) �Massive and generalized edema = Anasarca

Causes of edema Localised Generalised Others Venous obstruction; thrombophlibitis, DVT, SVC obstruction Lymphatic obstruction ; filariasis, malignancy, lymphoma, trauma Renal ; Nephrosis, AGN, ARF, CRF Cyclic edema Cardiac ; CCF, Cor pulmonale Pregnancy Inflammatory edema; infection, angiodema, urticaria Post-paralysis; CVA Liver cirrhosis Pre-menstrual edema Hypoalbuminemia; nephrosis, liver cirrhosis, protein losing enteropathy, malnutrition, catabolic states Drug-induced; NSAID, vasodilators, Ca-channels blockers, steriods, estrogens Non-pitting edema (idiopathic) myxedema

Clinical approach to edematous patient �Physical examination: Body weight blood pressure JVP Pitting character& sarcral Signs of ch. Liver disease Localized edema �Systemic examination; pleural effusion, basal crepitations, ascites

Laboratory work up Renal function testing Urine chemistry & sediment examination 24 hour urine collection S. albumin Liver function testing Pleural or ascites fluid analysis ( transudative Vs. exudative) Imaging; chest-x ray, ultrasonography / echocardiography
 and concomitant water excretion (aquaresis) Diuresis")
Diuretics; clinical use Diuretics increase renal sodium (natriuresis) and concomitant water excretion (aquaresis) Diuresis refers to increased urine volume in response to diuretic use Most diuretics enter urine by active proximal tubular secretion, and act on luminal surface to reduce sodium reabsorption at selected nephron segments Renal insufficiency impairs proximal secretion ( relative diuretic resistance), so higher doses needed in CKD patients; risk of toxicity

Diuretics; mode of action Drug class Mechanism Dosage Cabonic anhydrase inhibitor▣; acetazolamide reducing Na. HCo 3 reabsorption in PCT, but increases sodium delivery to distal portions of nephron, so considered as weak diuretic Diamox 250 mg tablet; 1 -4 times per day Loop diuretics∗; furosemide, torsemide, bumetanide Inhibit Na. K 2 Cl-cotransporter thick ascending loop of Henle, reducing Na. Cl reabosorption. Lasix 40 -80 mg tablets ; 2 -3 times per day ( available in parentral form) Thiazide diuretics∗▣; hydrochlorothiazide Inhibit Na. Cl transporter in DCT, reducing Na. Cl reabsorption. Esidrex 25 - 100 mg tablet; daily single dose Aldosterone antagonsits, K-sparing▣; spironolactone, eplerenone Inhibit Na. Cl reabsorption in CT & CD, reduce K secretion at these neprhon segments, relatively weak except in edematous condition associated with hyperaldosteronism Aldactone 25 -100 mg tablets; 2 times per day ∗Their efficacy depends on renal prostaglandins; diuretic efficacy is reduced by concomitant NSAID drug use ▣Not helpful if creatinine clearance < 30 ml/min/1. 73

Diuretics; potency & electrolytes disturbance Drug class Urinary Electrolytes Arterial p. H Na. Cl Na. HCo 3 K+ Carbonic anhydrase inhibitors + +++ + ↓ Loop diuretics ++++ 0 + ↑ Thiazides ++ + + ↑ Loop plus thiazides +++++ + ++ ↑ K-sparing agents + (+) - ↓

Response of surgical patients The injured or surgical patient, is even more difficult to excrete a salt and water load and we have to maintain normal serum osmolality The stress response to the injury or surgery causes anti- diuresis and oliguria mediated by; Vasopressin Catecholamines RAAS Water and salt are therefore retained even in the presence of overload

Response of surgical patients Following surgery, even when the serum osmolality is reduced by administration of hypotonic fluid, the ability to excrete free water is limited because the capacity of the kidney to dilute is impaired. Thus excess free water infusion risks dilutional hyponatraemia.

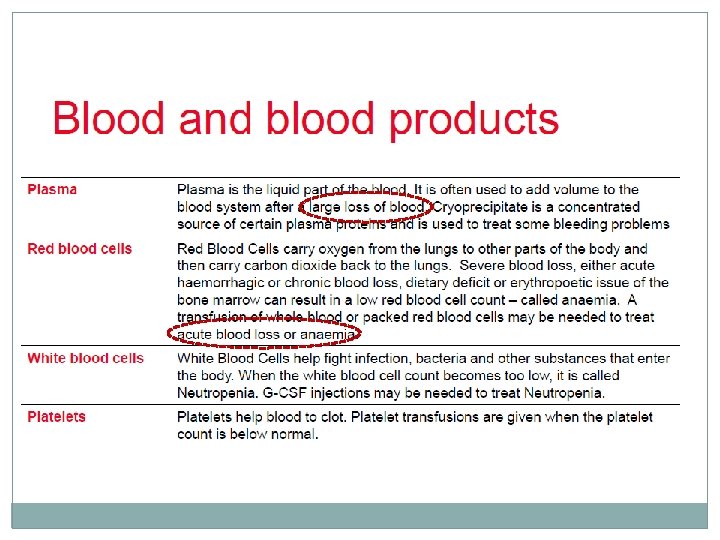
Fluid therapy; principles It is imperative that the amount and type of fluid should be correct for the patient. Inadequate fluid provision can lead to hypovolaemia and poor organ perfusion, and excessive provision can result in hypervolaemia, oedema and heart failure Fluid therapy based on: Crystalloids Colloids Blood products What difference between hypovolemia and dehydration ? ? osmolality

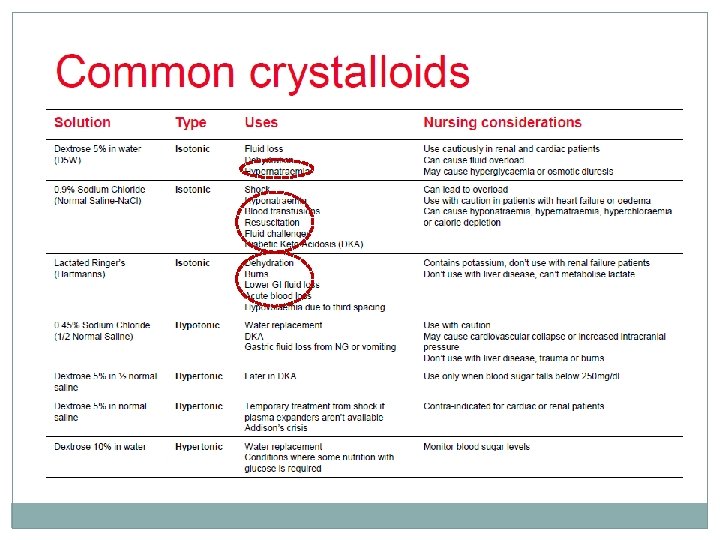
Crystalloid A solution of water and electrolytes; that can pass through semipermeable membrane They remain in vascular space less than 30 minutes, equilibrate with ISF or space For this reason larger volumes are required during fluid resuscitation Vs. colloids Eventually water of crystalloids diffuses into intracellular fluid

Colloids contain solutes in the form of large proteins or mucopolysaccharides Because of large molecular size, they remain longer periods in the vascular space 3 -6 hours, by that time metabolized Considered main volume expanders in shock state, if the cause was not due to hemorrhage Excessive volumes can lead to cellular dehydration


Maintenance Fluid replacement; NPO � In infants: 0 -10 kg: 11 -20 kg: > 20 kg: 100 ml/kg/d 50 ml/kg/d 20 ml/kg/d � Patient (70 kgs, male), role of 4 -2 -1 ml/kg/h: 1 -10 kg 11 -20 kg >20 kg 4 ml/kg/h 2 ml/kg/h 1 ml/kg/h 40 ml/h 20 ml/h 50 ml/h Together: 110 ml/h 2640 ml/d ( in female 15 -20% less) If patient is NPO, and with normal renal function, then needs electrolytes supplments: � Sodium ~ 100 -150 m. Eq/day (1 -2 m. Eq/kg/day), average 2. 5 -3. 0 liters � Potassium ~60 -80 m. Eq/day ( 0. 5 -1 m. Eq/kg/day), upto 100 m. Eq if has diarrhea or hypokalemia
 Calculate daily fluid requirement;")
Fluid balance chart Evaluate pt. volume state ( shock state) Calculate daily fluid requirement; deficit & maintenance Calculate input and output fluids Formulate fluid balance; Deficit ( resuscitatioin) Ongoing sugical losses ( bowel mechanical preprations) Euvolemic ( maintenance) Overloaded ( hypervolemic) Determine amount, type, and rate of fluid supplement Treat any electrolyte problem Provide nutritional/ caloric support

Fluid management outline Fluid resuscitation/ challenge in hypovolemic patient: infusion of crystalloid one liter over one hour, should produce a response by stabilizing vital signs ( pulse and B. P), then Maintenance fluid volume according to the role of 4, 2, 1 Half life of 0. 9% Na. Cl in intravascular compartment is 20 -30 minutes, while for colloid solution is 3 -6 hours One liter of 0. 9% Na. Cl will increase plasma volume by 250 ml within 2 - 3 hours of equilibrium with ISF space 20% albumin expands plasma volume upto 5 times volume infused

q Simon Steddon, Neil Ashman. Handbook of nephrology and hypertension, 2 nd edition, 2014, oxford university press. q Maxime papadakis, Stephen Mcphee. Current medical diagnosis and treatment. 55 th edition, 2016, Mc. Graw Hill. q Brian Walker, Nicki Colledge, et al. Davidson’s principles and practice of medicine. , . 22 nd edition, 2014. Churchill Livingstone Elsevier q Parveen Kumar, Michael Clark. Kumar and Clark’s clinical medicine, 8 th edition, 2012. Saunders Elsevier press.

Case senario 60 year old woman with intestinal obstruction, B. P 96/58 mm. Hg, has the following fluid balance chart: - Intake: nil by mouth, 3000 ml IV normal saline - Output: 500 ml urine, 3500 ml from nasogastric tube Last blood results show low potassium. She weighs 60 kg, is apyrexial. She complains of a dry mouth. Which fluids are required for the next day before surgery? ? ? ?
- Slides: 39