Body composition and Practical Nutritional Assessment Khursheed Jeejeebhoy

Body composition and Practical Nutritional Assessment Khursheed Jeejeebhoy

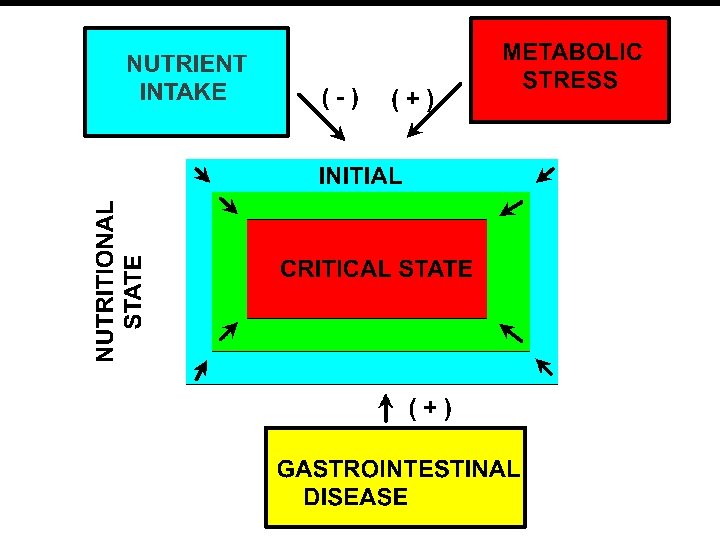
Determinants of Nutritional Status w Nutritional health • a state of equilibrium • nutrient intake and requirements balance. w Malnutrition • net nutrient intakes < requirements. • change in body and blood composition • changes in body and blood composition have traditionally used to assess nutritional status.

Nutritional Assessment: Veterinary approach C -- C– P--

Objective of Nutritional Assessment w Veterinary Objective: • Mass of muscle, fat and viscera in the carcass. w Clinical Objective: • To improve patient outcome. w Can measurement of muscle, fat and viscera predict outcome?

Levels of Body Components Tissue-Organs Adipose tissue Skeletal Muscle Cellular Molecular Atomic Adipocyte Lipid Hydrogen Water Cells Carbon Visceral Organs Skeleton Oxygen ECF Protein ECS Mineral N, Ca, P, K, Na, Cl

Nutritional Assessment: Tissue-Organs 1. Body Weight and Weight Loss 1. BMI = Wt/Ht 2 < 15 is associated with mortality 2. Unintentional weight loss is associated with mortality 3. Weight is difficult to assess due to: 1. Dehydration 2. Edema 3. Dialysate 4. Weight loss estimate has errors of recall

Nutritional Assessment: Tissue-Organs 1. How much muscle and fat: Anthropometry Arm muscle circumference Skin Fold thickness 2. How much circulating protein: Visceral Protein Albumin Prealbumin Transferrin 3. Errors of Antropometry Errors due to Baseline values Variability of measurement What is abnormal? Errors due to edema 4. Errors of Visceral Protein Altered by hydration status Altered by Protein loss (GI and renal) Altered by Infection
 Two low level energy xrays to differentiate")
Nutritional Assessment: Tissue-Organs DUAL-ENERGY XRAY ABSORPTIOMETRY (DEXA) Two low level energy xrays to differentiate tissues of different densities. w The only method for assessing the skeleton. w Differentiates body composition into: w • Fat • Muscle • Bone w No data to predict outcome

Levels of Body Components Tissue-Organs Cellular Molecular Atomic Adipose tissue Adipocyte Lipid Hydrogen Water Skeletal Muscle Cells Carbon Visceral Organs Skeleton Oxygen ECF Protein ECS Mineral N, Ca, P, K, Na, Cl

Nutritional Assessment: Cellular Cell mass = Total body potassium / 150 X 1/80 w Potassium content of cells = 150 mmol/L w Solid to fluid in cells = 1: 4 w Intracellular potassium is very sensitive to malnutrition and refeeding w
 1117 -1127 w w w")
Nutritional Assessment: Cellular Am J Clin Nutr 1982; 35(suppl) 1117 -1127 w w w Patients with anorexia Nervosa Weeks of feeding TBN TBK K/TBN kg m. M 0 1. 2 1590 1. 31 4 1. 33 1897 1. 42 8 1. 37 2103 1. 53

Levels of Body Components Tissue-Organs Adipose tissue Skeletal Muscle Cellular Molecular Atomic Adipocyte Lipid Hydrogen Water Cells Carbon Visceral Organs Skeleton Oxygen ECF Protein ECS Mineral N, Ca, P, K, Na, Cl
 + Fat Free Mass (FFM)")
Nutritional Assessment: Molecular Body Weight = Fat mass (FM) + Fat Free Mass (FFM) w Hydration of FFM = 73% w FFM= Total Body Water/0. 73 w Total Body Water can be assessed by: w • Isotope dilution • Bioelectric Impedance

Nutritional Assessment: Molecular 1. Isotope dilution 1. Total body water 2. Extracellular water 3. No correlation with outcome 2. Bioimpedance Analysis 1. Easy to perform 2. Measures body water 3. No correlation with outcome 3. DEXA 1. Measures FM 2. Muscle mass from which FFM can be derived 3. Bone mass

Levels of Body Components Tissue-Organs Adipose tissue Skeletal Muscle Cellular Molecular Atomic Adipocyte Lipid Hydrogen Water Cells Carbon Visceral Organs Skeleton Oxygen ECF Protein ECS Mineral N and Ca

Nutritional Assessment: Atomic w w w Measured By: Hydrogen Neutron Activation Carbon Inelastic Neutron scattering Nitrogen Prompt Gamma Emission Calcium Neutron Activation

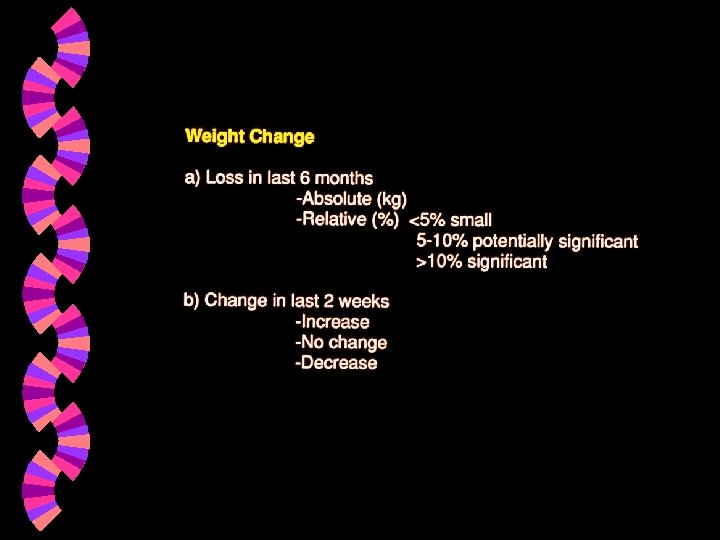
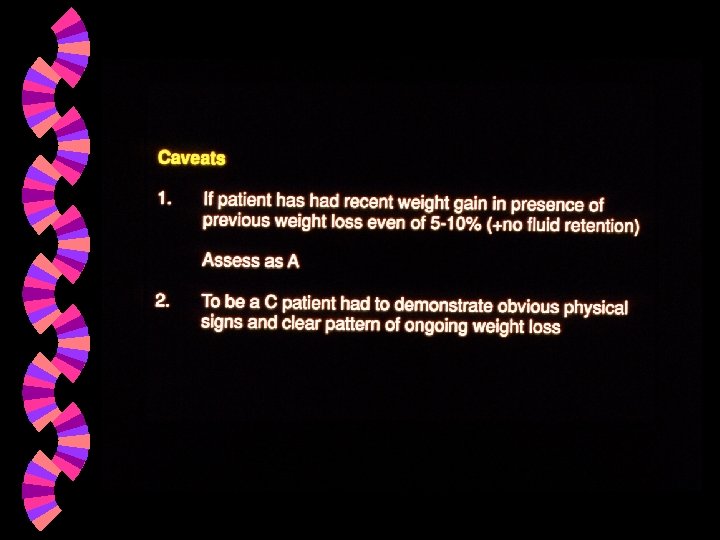
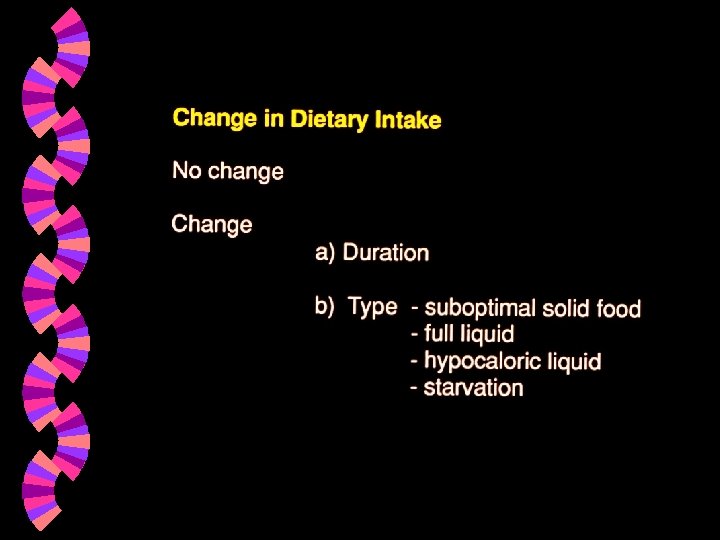
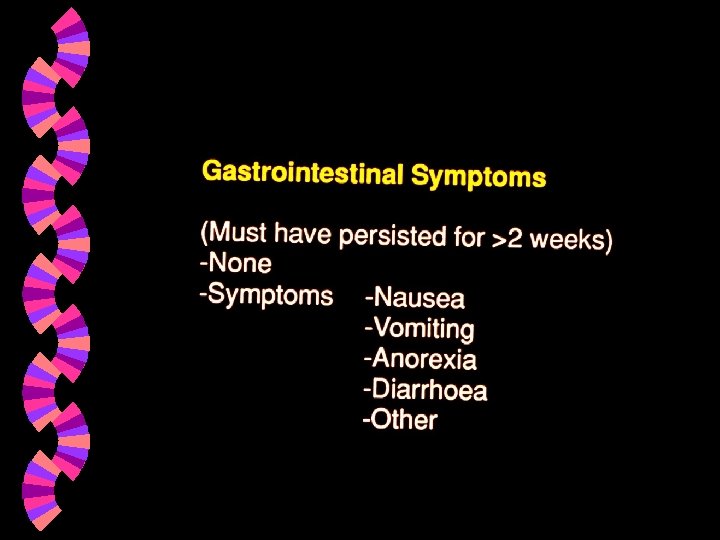
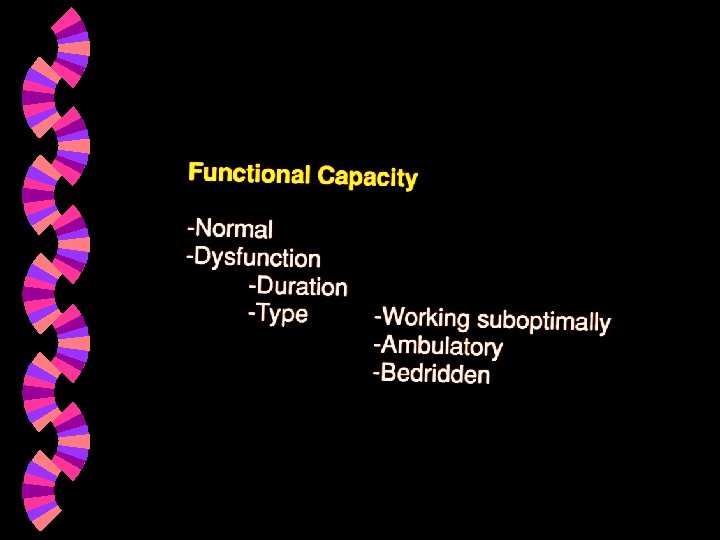
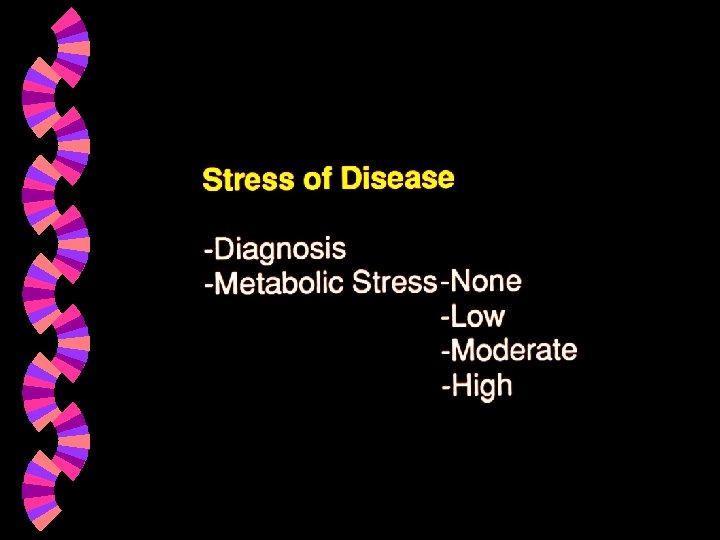
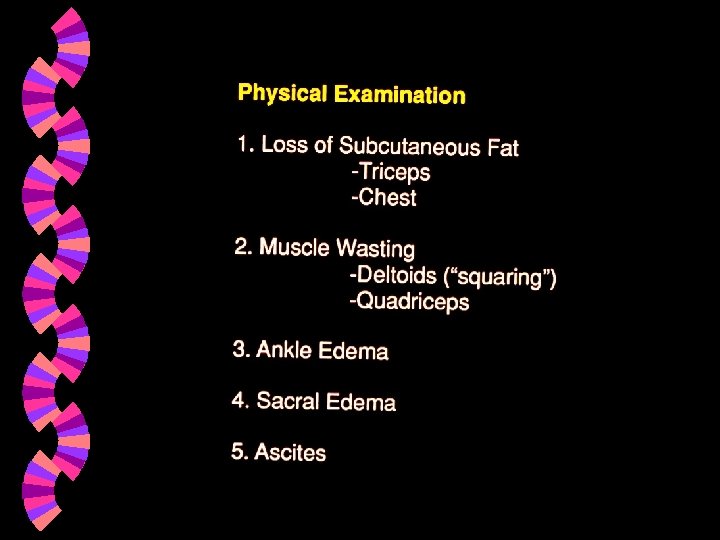
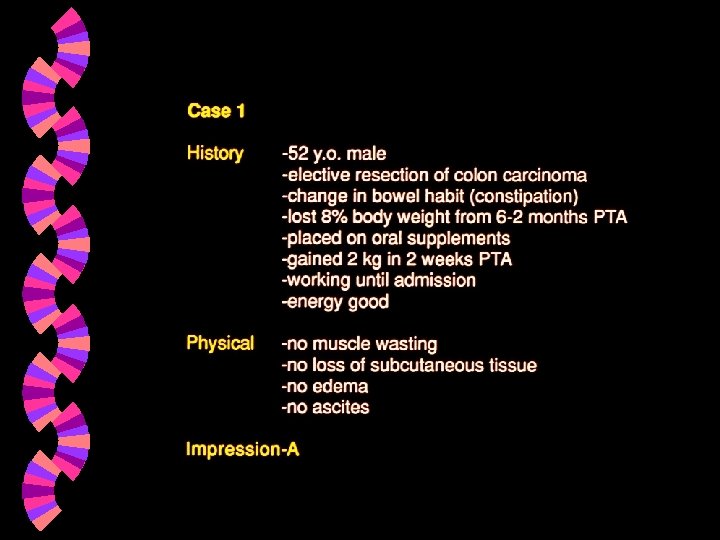
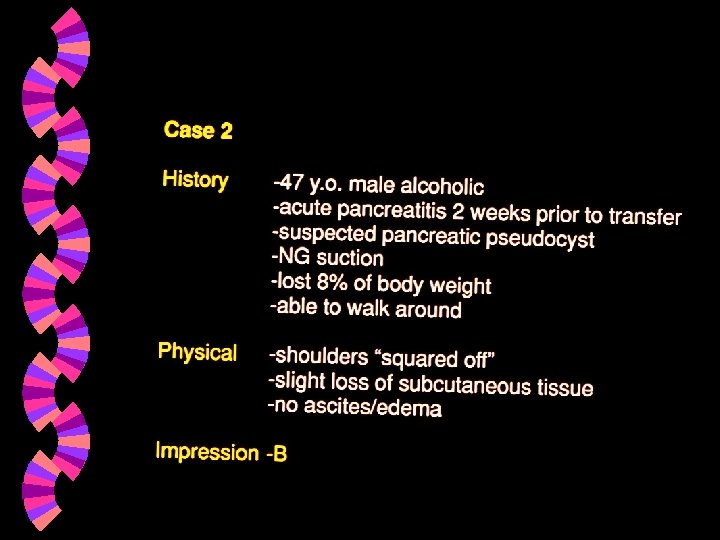
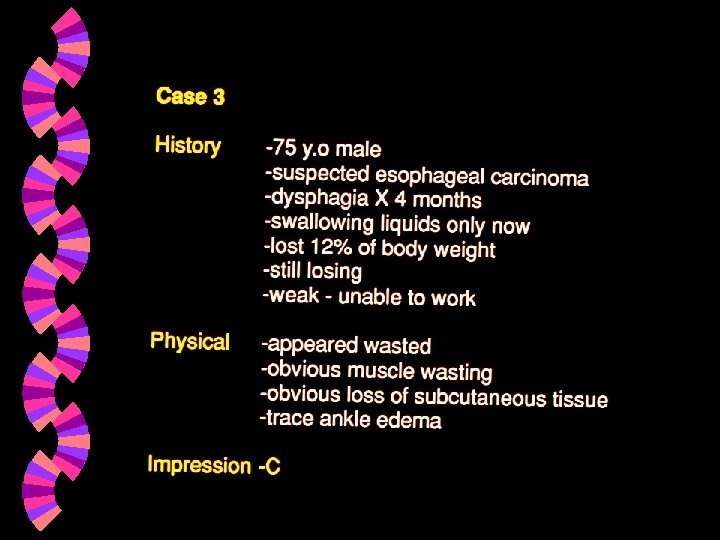
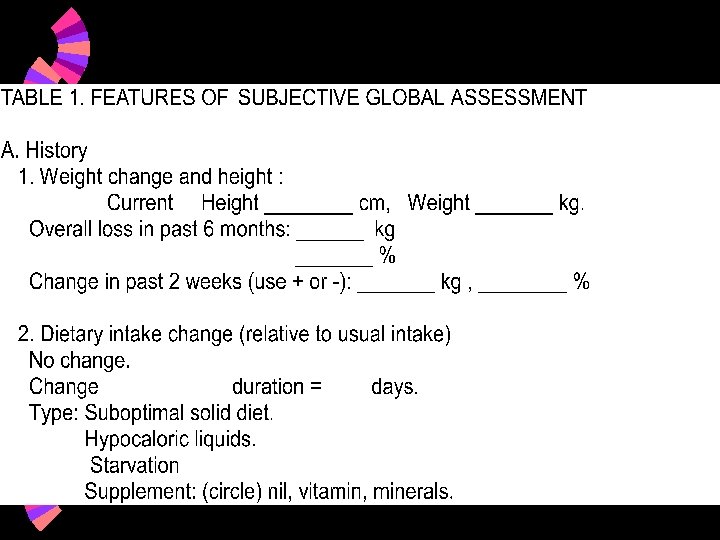
Subjective Global Assessment
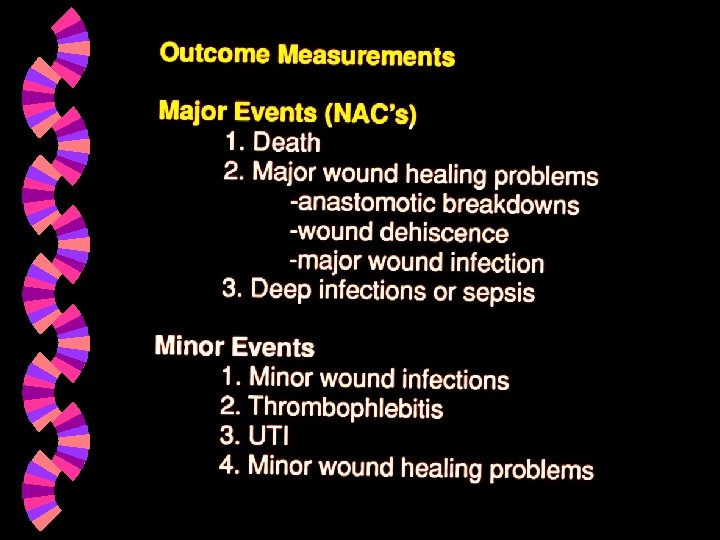
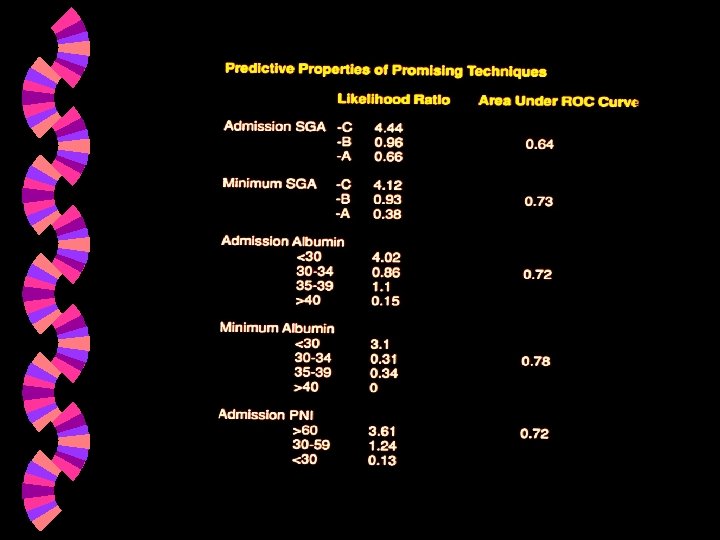

Predictive value of a test

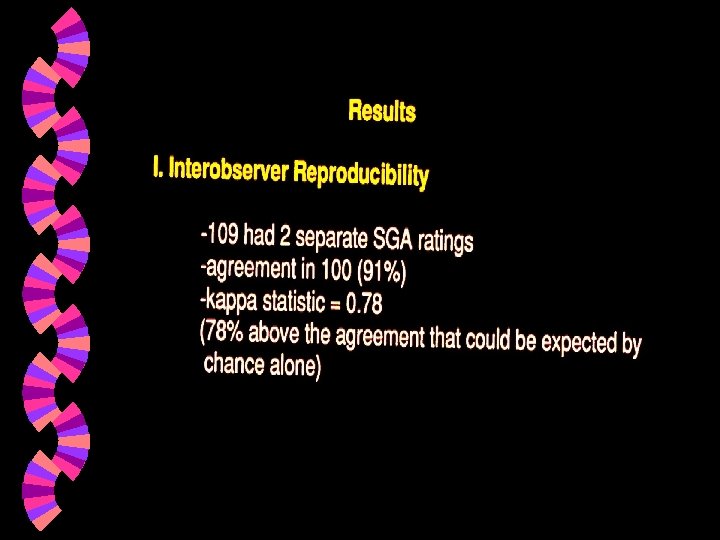
Predictive ability of SGA

Nutritional Prognosis in Hospital Patients Perman et al. Am J Clin Nutr 2002; 75: 426 S 448 Hospital Patients w SGA assessment and record of other risk factors influencing prognosis w Logistic regression to evaluate independent risk of malnutriton by SGA on complications and mortality w

Nutritional Prognosis in Hospital Patients Perman et al. Am J Clin Nutr 2002; 75: 426 S * only odds ratio of BC not different from A *

Mohandas IJG 2005; 24: 246 -250

Subjective Global Assessment and Cancer w Thoresen et al. Palliat Med. 2002 ; 16: 33 -42. • Sensitivity 96% and specificity 83% w Persson et al. Clin Nutr 1999; 18: 71 -77 • Survival Lower in SGA B+C vs A (P<0. 001)
- Slides: 48