BLUNT CHEST TRAUMA PRESENTED BY DR RAZZAQ CASE

BLUNT CHEST TRAUMA PRESENTED BY DR RAZZAQ

CASE SCENARIO • • • • A 30 -year-old male was hit by a motor vehicle about 3 h ago. At presentation, he had a threatened airway with labored breathing; his respiratory rate was 32/min with O 2 saturation of 85%. He had paradoxical chest movements and decreased air entry on the left side. His heart rate was 120/min, blood pressure was 100/80 mm. Hg, and Glasgow coma scale (GCS) score was 15/15. After initial stabilization and left-sided intercostal drainage (ICD), secondary survey revealed abdominal distention with tenderness over the left upper quadrant of the abdomen. A computed tomography (CT) scan of the chest and abdomen showed multiple rib fractures on the left side of the chest with underlying lung contusion and ICD in situ. It also revealed a shattered spleen and 3 -cm laceration in segment 6 of the liver along with 1 -cm laceration in the upper pole of the left-sided kidney. Exploratory laparotomy was performed. The liver and kidney were preserved, while the spleen was removed. The patient gradually recovered in intensive care unit (ICU ).

• Primary survey • Perform primary and secondary survey • A. Airway with cervical spine protection : Evaluation of airways is the first priority during primary survey • All patients presenting with threatened airways and respiratory distress should have the airway secured. • Cervical immobilization is maintained till the injury is excluded by radiological or clinical

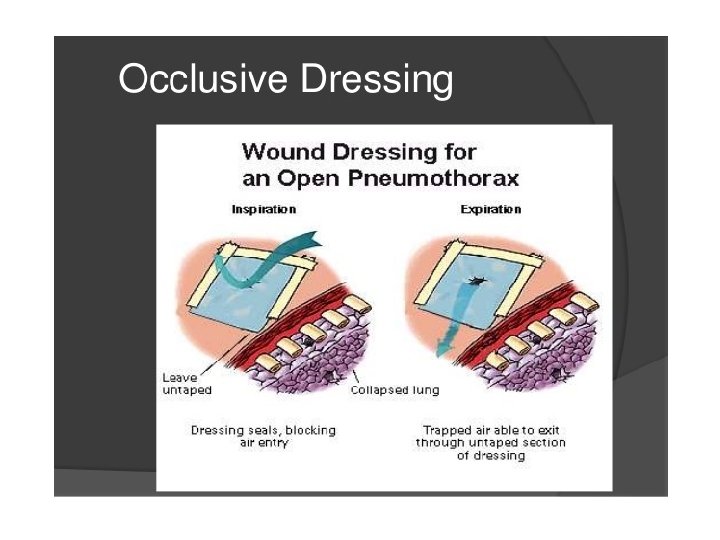
• Breathing and ventilation : Expose the chest & observe chest wall movement, breathing pattern, and neck veins; to auscultate breath sounds; and to monitor Sp. O 2. • • Injuries that should be identified and treated during the primary survey arethe following: • – Tension pneumothorax—with immediate needle thoracostomy and then with an intercostal tube • – Massive hemothorax—with insertion of a large-bore (36 F) chest tube and volume replacement • – Open pneumothorax—with flutter valve dressing, taped on three sides, till ICD is placed; thereafter, closed dressing • – Cardiac tamponade—with pericardiocentesis follwed by definitive surgery • – Flail chest with pulmonary contusion—with analgesia and elective intubation and positive pressure ventilation

• Circulation with hemorrhage control : The pulse rate, blood pressure, and levelof consciousness determine the grade of shock. • Circulation volume has to be maintained with isotonic fluids and blood transfusions. Identify the source of bleeding and control it. • D. Disability (neurologic evaluation): Assess GCS and evaluate the pupillary size and reaction to light. Low GCS score may be due to decreased cerebral oxygenation or perfusion (shock) or direct cerebral injury. • E. Exposure/environment control: Completely undress the patient for thorough examination and assessment. Do not forget to examine the back. A warm environment should be maintained to avoid hypothermia

• Secondary survey • This involves detailed patient history, complete in-depth physical examination, • relevant radiological, and laboratory investigations with reassessment of vital signs & to identify injuries

• Triage for surgery • • Once the primary survey is concluded, the next step is to triage the nonresponders to emergency surgery—exploratory laparotomy or thoracotomy for damage control • o. Chest injuries • Majority of the patients (85% of the patients) with thoracic injuries require intervention in the form of tube thoracostomy, observation, and pain control. • And other patients require a formal thoracotomy.

• Abdominal injuries • Indications for urgent laparotomy include the following: • • Penetrating abdominal injury • • Hollow viscus injury • • Blunt trauma with ongoing intraperitoneal b. Triage the patients to the ICU • Triaging the patients to the ICU or to the floor (wards) is decided on the basis of the severity of the injury and the extent of surgery, requirement of the mechanical ventilator and inotropic support, age and co morbidities of the patient

• Continue observe & treatment • A. Ventilation and circulation assessment • • Monitor respiratory rate, oxygen saturation, and arterial blood gas analysis, and adjust ventilatory settings accordingly. • In case of prolonged requirement of ventilation (usually more than 7 days), tracheostomy should be considered. • Pulse rate, blood pressure, central venous pressure, urine output, hematocrit, • and lactate levels indicate the degree of perfusion and the grade of volume deficit. • Unstable / critically ill patients might warrant other invasive monitoring techniques such as intra-arterial pressure and Sc. VO 2 measurements. • Circulation is maintained with fluid and blood transfusion with or without inotropic support

• • • • • Intercostal tube insertion. After sterile preparation and drape 1% lidocaine is infiltrated in the midaxillary line at the level of the nipple. A 2 -3 cm transverse skin incision is made. Dissection is performed by blunt forceps down to the pleura passing just superior to the rib surface to avoid injury to neurovascular structures. A gloved finger is used to confirm separation of lung from chest wall. A large-bore (28– 32 Fr) intercostal tube is inserted without a trocar and advanced in a postero-superior direction. Curved forceps clamped to the distal side hole of the tube can be used to guide the tube through the chest wall. The tube is immediately connected to an underwater seal drainage system and checked for satisfactory drainage and tidal rise and fall in fluid level with respiration. Non-absorbable sutures are used to seal the skin incision around the tube and secure the tube. The intrathoracic position of the tube is checked with a chest radiograph.

• Management of the ICD tube • Monitor volume and nature of the output daily, column movement, presence of • air leak, and lung expansion clinically and radiologically. • 1. Volume • • Common causes for persistent high output: • – Hemorrhage • – Thoracic duct injury • – Hypoproteinemia • • Sudden decrease in the volume of the output: Check for tube blockage or malpositioning.

• Nature of the output • • Sanguineous output—ongoing hemorrhage: Output of more than 200 m. L/h of sanguineous fluid continuously for 2– 4 h is an indication for thoracotomy. • • Turbid output with pyrexia indicates an infective focus
. Presence of")
• Milky white, high-volume output points to thoracic duct injury( chylothorax). Presence of chyle may be confirmed at the bedside by dissolving the drained fluid in equal amount of ether. If it gets dissolved, then it is chyle; otherwise, it is pus. • Check the triglyceride level. • Low output (<1, 000 m. L/24 h) can be managed conservatively. • High output usually requires surgical management. • 3. Wide swinging of column movement (>5 cm) is suspicious of poor lung expansion or lung collapse and should be investigated further with the chest X-ray and bronchoscopy if needed.

• Air leaks indicate the presence of tracheobronchial/parenchymal communication with the pleural cavity. • Chest tube insertion sites should be checked for peritubal air entry due to loose sutures. • • Treatment of air leak: Minor air leaks usually heal with deep breathing • exercises. Persistent air leaks, not settling down with chest physiotherapy • alone, require application of negative pressure suction (usually 10 cm • H 2 O) to the underwater seal bottle. • Massive air leaks causing oxygen desaturation will require insertion of a second ICD tube and usually thoracotomy. • • After stoppage of air leak, check the chest X-ray after clamping the tube • for 24 h to look for lung collapse, and the ICD tube can be removed if the • chest X-ray is normal. • • In case of subcutaneous emphysema, the extent should be marked and • monitored daily for change in extent after insertion of the ICD tube. • There is no role for skin incisions.

• In cases of clotted hemothorax, declotting is done with streptokinase. • • 1 – 1. 5 million units of streptokinase is diluted in 100 m. L and infused through the ICD tube under aseptic precautions. The tube is then clamped for 3– 4 hrs ; chest physiotherapy is done and then the tube is opened. This may be repeated once a day for 3– 4 days till clots are evacuated. • This procedure is not indicated in patients with coagulopathy or patients on warfarin. • 6. Fever, productive cough, and infiltrates in the chest X-ray indicate pulmonary infections. Broadspectrum antibiotics should be started empirically and changed to specific antibiotics depending on the sensitivity.

• Radiological investigations • • Chest X-rays should be done to monitor the lung expansion and after the removal of the ICD tube to look for pneumothorax. • • Usg and CT scans should be done for suspected loculated effusions and pneumothorax and to guide its drainage percutaneously. • The following conditions should be fulfilled before the removal of the ICD tube: • – Less than 50– 100 m. L output and serous in nature • – Less than 5 cm swinging of air column with normal breathing

• – Absence of fever and air leak • – Full lung expansion • • Chest tube insertion sites must be inspected every day for infections and air or fluid leakage with regular care of the wound site • Tracheostomy site and surgical wound sites • Inspect for surgical site infection. • D. Regular active and passive chest physiotherapy • This is required to prevent atelectasis and pneumonia. • E. Pain control • By nsaids, opioids, epidural analgesia can be given

• Abdominal injuries • Solid organ injuries are managed either non operatively or operatively depending on the severity of the injury and the hemodynamic stability of the patient. Hollow viscous injuries are usually managed operatively. • Step 5: Nonoperative management of solid organs (spleen, liver, and kidney) • • Nonoperative management should be practiced only in highly specialized trauma centers that have 24 -h availability of trauma surgeons. • • Daily clinical examination of the abdomen with hemodynamic status assessment is based on pulse rate, blood pressure, urine output, abdominal girth, intra abdominal pressure, and fall in hemoglobin and hematocrit levels. • • Complete bed rest should be advised for the fi rst 48 h and then gradual mobilization is done

• Ultrasound examination of the abdomen is done, if clinical situation demands, to • look for significant increase in the intraabdominal collection. Abdominal distention, development of peritoneal signs, and decrease in urine output indicate ongoing hemorrhage and need for operative management. • Progressive drop in hematocrit with hemodynamic instability should also indicate the consideration for operative management

• • In case of liver injuries, billary peritonitis may present the clinical picture of • intestinal perforations. Clinical and radiological examinations should be performed to rule out missed intestinal injuries, and in their absence, percutaneous • drainage of the bile collection can be done, can avoid laparotomy.

• POST OP MANAGEMENT IN ICU • In case the abdominal closure seems to be difficult during the primary surgery( due to bowel edema/retroperitoneal collection, etc. ), it is prudent to leave it open. • as forceful closure would lead to increase in intra-abdominal pressure resulting in the abdominal compartment syndrome. • Oral diet is started at the earliest and gradually advanced to regular diet as tolerated.

• Care of the feeding jejunostomy tube should be taken properly. Postoperatively, tube feed at the rate of 30 m. L/h for 3– 6 h should be given. If the patient tolerates, & gradually increase feed as tolerated to meet calories and protein requirement over 24– 48 h. • • Conditions suggesting the need for parenteral nutrition are as follows: • – Oral intake less than 50% of the energy needs • – Unable to tolerate nasogastric or nasojejunal feed for more than 7 days in previously wellnourished patient. • – Nonfunctioning gastrointestinal tract

• • Following precautions to be taken. Inspection of the surgical sites is done for signs of inflammation and infection. • Monitoring of the drain output and nature of fluid should be done. • In case the drains show persistent and or purulent output, it can be indicative of deep surgical site infections or intestinal fistulae. If such is the case, rapid clinical/ radiological examination followed by opening of laparotomy incision site and thorough lavage is indicated. If intestinal fistulae are present, it should be treated either surgically or non operatively depending on its location and output. • • • Persistent high drain output in cases of pancreatic and splenic injury should raise suspicion of the pancreatic fistula. • • Drain amylase should be requested on or after the third postoperative day in cases of suspected pancreatic fistula in cases of pancreatic and splenic injury. • • • Drain amylase three times that of serum amylase confirms pancreatic fistula. Continuing the drains, antibiotic coverage (if signs of infections present), serial radiological examinations, and drainage of collections is recommended for the treatment of pancreatic fistulae. Use of somatostatin or its analogue may be useful in such situations.




- Slides: 28