Blowout Fracture M Rinaldi Dahlan Cicendo Eye Hospital

Blow-out Fracture M Rinaldi Dahlan Cicendo Eye Hospital Bandung Department of Ophthalmology Faculty of Medicine Universitas Padjadjaran

Introduction Orbital fracture is the most common type of fracture of the orbital walls

Introduction Medial wall Orbital floor most vulnerable The term Blow-out fracture refers specifically to the fracture of an orbital wall in the presence of an intact orbital rim The thin part of the maxillary bone ( 0, 5 mm thick in this area)
 describe floor fracture Smith and Converse (1956) blow out fracture")
Introduction Mc Kenzie (1844) describe floor fracture Smith and Converse (1956) blow out fracture Mechanism: Blunt trauma pushes the orbital tissue posteriorly increase in intraorbital pressure the orbital bones to break at their weakest point posterior medial aspect of the orbital floor

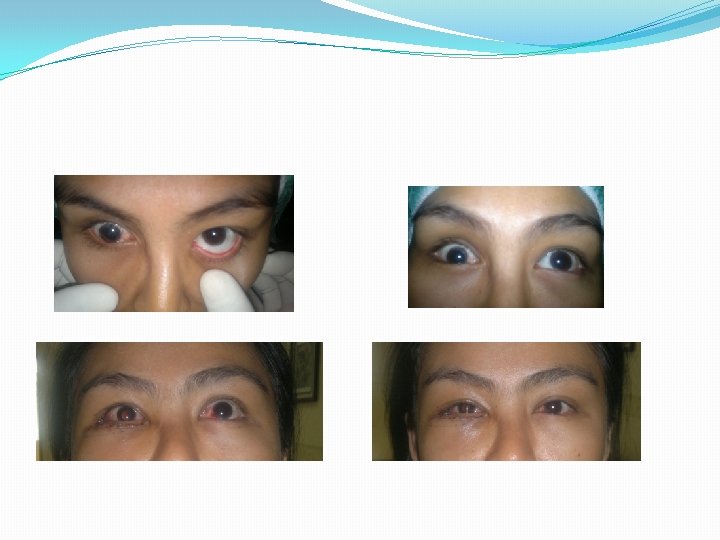
Clinical Presentation External sign: Lid edema, subcutaneous or orbital emphysema, Ecchymosis, Subconjunctival hemorrhage, enophthalmos, globe ptosis on some occasions, there may be little or no signs of external injury Ocular injury anisocoria can occur with inferior floor fracture Diplopia Infraorbital nerve hypesthesia Ocular Motility, small fracture incarcerate

Evaluation Visual acuity, pupil, intraocular pressure, biomicroscopy and fundus. Globe position hertel exophthalmometry Ocular motility injury to the extra ocular muscle or cranial nerve palsy Diplopia visual fields Photographs as documentation for patients to appreciate an acceptable operative result Force duction test paretic and restrictive motility patterns X ray , CT scans

Cicendo 102, Cares for Vision

Management Smith and Converse: early surgical correction Putterman et al: 4 -6 months surgical and non surgical Dutton: early repair symptomatic persistent diplopia with positif force ductions, CT evidence of orbital tissue or muscle entrapment, no clinical improvement over 1 -2 weeks, enophthalmos of 3 mm or more, significant globe ptosis, floor defect > 50% Conservative/ observation: minimal diplopia with good motility, no CT evidence of tissue entrapment, absence enophthalmos or globe ptosis.

The goal of blowout # repair : - Free entrapped orbital tissue - Return orbital volume to normal In children: early surgery ( 2 -4 days) has been advocated trapdoor defect cause ischemic damage and tissue fibrosis

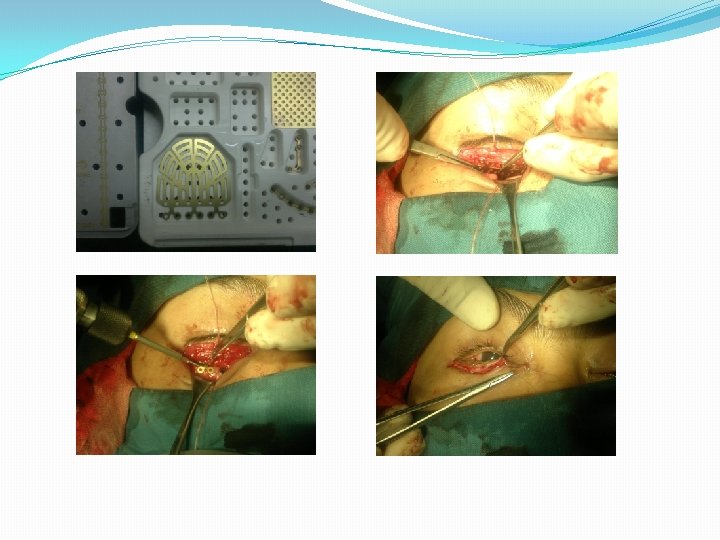
Treatment and repair Surgical: 7 -10 days to allow swelling and hemorrhage to subside Anesthesia: general, neurolepsia Approached: subcilia or transconjunctival orbital rim periosteum elevated off the orbital floor until the fracture site is identified entrapped tissue is freed carefully and elevated from the defect insert material for floor reconstruction Cicendo 102, Cares for Vision

Cicendo 102, Cares for Vision

Cicendo 102, Cares for Vision

Postoperative Care Ice packs +/- 48 hours Broad spectrum antibiotics: 5 -7 days Patients are advised not to blow their nose

Complications The result of injury itself or the surgical repair Optic nerve injury Retrobulbar hemorrhage immediate surgical exploration and drainage is necessary Implant migration and extrusion

Another technique:


Thank you Cicendo 102, Cares for Vision
- Slides: 19