BLOOD PHYSIOLOGY Anemia PROF MAGDY KAMEL 1 Objectives

BLOOD PHYSIOLOGY Anemia PROF MAGDY KAMEL 1

Objectives To demonstrate basic Knowledge of : Definition of anemia Types and causes of anemia Normocytic Normochromic Microcytic hypochromic Macrocytic Effects of anemia Diagnosis of anemia

Anemia Definition : Decreased RBCs count or hemoglobin content or both below the normal range for age and sex. - HB content of the blood (HB%) : In adult males 15 gm% (ranging between 14 -16 gm%). In adult females 14 gm% (ranging between 13 -15 gm%). More in children and higher in newly born infants (up to 19 gm% ).
 : It is the average volume of")
Blood Indices - Mean Corpuscular Volume (MCV) : It is the average volume of a single RBC Normal value = 90 cubic µ ( 80 – 100 cubic µ) - Mean Corpuscular Hemoglobin (MCH) : It is the average amount of HB in a single RBC Normal value = 30 pg ( 27 – 33 pg ) - Mean corpuscular hemoglobin concentration (MCHC): It is the amount of hemoglobin in 100 ml packed RBCs Normal value = 33 ± 3%

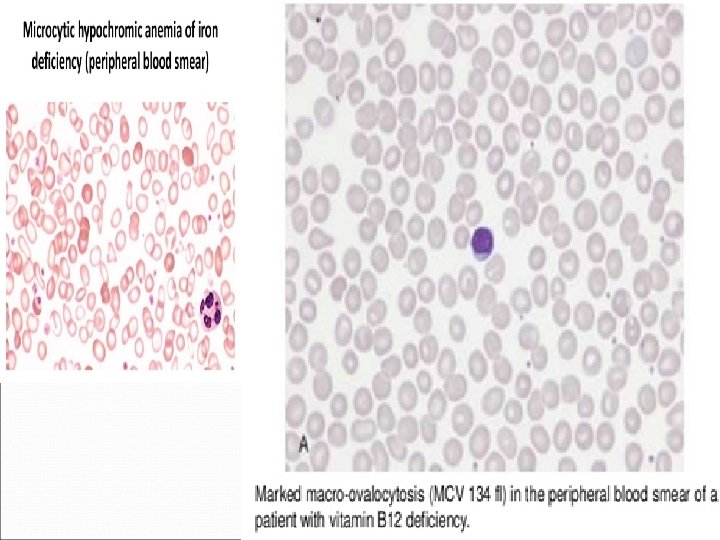
Types of Anemia According to the blood indices , there are 3 types : I- Normocytic normochromic anemia: RBCs are normal regarding MCV (Normocytic ) & MCH ( Normochromic) , but their number and the blood HB content are both decreased 2 -Micorocytic hypochromic anemia (as Iron deficiency anemia ) : In this type MCV , MCH , RBCs count & HB content of the blood are all decreased 3 - Macrocytic anemia (as B 12 & folic acid deficiency anemia or megaloblastic anemia) : In this type MCV is increased

I-Normocytic normochromic anemia Causes : A - Hemolytic anemia Means excessive destruction of RBCs due to abnormality in either the RBCs or in the blood environment 1 - Hereditary spherocytosis: as in in which RBCs loss its biconcavity and become spherical in shape due to defect in cell membrane. and on passing through the splenic pulp and some other tight vascular beds they are easily ruptured by even slight compression.

Spherocytes marked as black arrow and poikilocytes marked as green arrow
: The structure of hemoglobin is abnormal , as in")
2 - Hemoglobin defects (hemoglobinopathies): The structure of hemoglobin is abnormal , as in : A-Sickle cell anemia patient have hemoglobin-S. When this hemoglobin is exposed to low concentrations of oxygenit precipitates into long crystals give RBCs the appearance of a sickle. Sickle-shaped cells don’t move easily through blood. They’re stiff and sticky and tend to form clumps and get stuck in blood vessels. The clumps of sickle cell block blood flow in the blood vessels that lead to the limbs and organs. Blocked blood vessel can cause pain, serious infection, and organ damage.

Deoxygenation of SS erythrocytes leads to intracellular hemoglobin polymerization, loss of deformability and changes in cell morphology. OXY-STATE DEOXY-STATE

Normal and Sickled Red Blood Cells in Blood Vessels Figure B shows abnormal, sickled red blood cells clumping and blocking the blood flow in a blood vessel. The inset image shows a cross-section of a sickled red blood cell with abnormal strands of hemoglobin. Figure A shows normal red blood cells flowing freely in a blood vessel. The inset image shows a cross-section of a normal red blood cell with normal hemoglobin.

Signs and Symptoms Individual signs and symptoms varies. Some have mild symptoms, others have very severe symptoms and may be hospitalized for treatment Present at birth, many infants doesn’t show signs until after 4 months of age Anemia: Fatigue (tiredness), pale skin and nail beds, jaundice, and shortness of breath Pain (Sickle Cell Crisis): Sudden episode of pain throughout the body. Common sites: bones, lungs, abdomen, and joints. Lack of blood flow can cause pain and organ damage.
 Due to defective biosynthesis of globin chains of Hb. So, individuals")
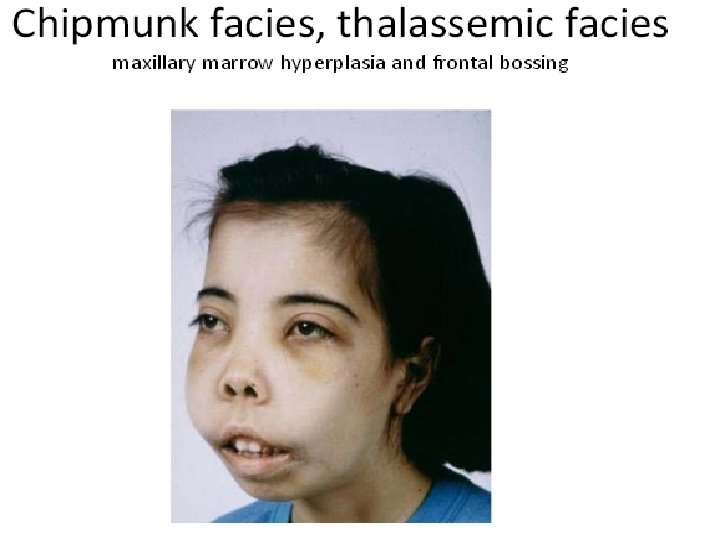
B-Thalassemia (Mediterranean anemia) Due to defective biosynthesis of globin chains of Hb. So, individuals with Thalassemia don’t produce enough alpha & beta globin chain of Hb. This causes the red blood cells to be unable to carry enough oxygen through the body ( anemia) * α Thalassemia : fewer alpha-globin chains are produced, resulting in an excess of β-chains in adults and excess γ-chains in newborns. This excess of the β-globin & γ-globin chains relative to αGlobin chains → Bart's Hb (γ 4) in fetal life & Hb. H (β 4) after birth, which → extravascular hemolysis. *β thalassemia : there is an excess of the α-globin chains relative to the β-globin chains & γ-globin chains, which→ α-globin tetrameric inclusions (α 4) which interact with RBC membrane & ↓ RBC survival → anemia & ↑ erythroid production.
. Glucose-6")
3 - Enzymatic defect as in glucose 6 - phosphate dehydrogenase deficiency (Favism). Glucose-6 -phosphate dehydrogenase (G 6 PD) is an important element (enzyme) in the glucose oxidation process RBCs and for maintaining their normal life span. G 6 PD deficiency is an inherited disorder caused by a defect or deficiency in the production of that enzyme. Consequently, G 6 PD deficiency may cause the destruction of RBCs leading to a hemolytic anemia in which the body cannot compensate for the destroyed cells. males usually affected and females are carriers). Favism: Form of hemolytic anemia that can occur after eating fava beans (broad beans) or walking through a field of the plants.

The abnormal cells had the appearance of having had a piece bitten and are, therefore, termed "bite cells". Heinz bodies (also referred to as "Heinz-Ehrlich bodies") are inclusions within red blood cells composed of denatured hemoglobin.
 Extracorpuscular causes (Acquired hemolytic anemia): -Antibodies against RBCs e. g. hemolytic disease of")
(4) Extracorpuscular causes (Acquired hemolytic anemia): -Antibodies against RBCs e. g. hemolytic disease of the newborn and incompatible blood transfusion -Bacterial toxins e. g. malaria -Chemical poisons e. g. lead and arsenic -Drugs e. g. sulphonamides -Snake venoms B- Aplastic anemia Due to : a- Irradiation b- Chemicals e. g. cytotoxic drugs c- Chronic renal diseases , due to decreased erythropoietin production d- Malignancy C- Hemorrhagic anemia After rapid hemorrhage, the body replaces the fluid portion of the plasma in 1 to 3 days, but this leaves a low concentration of red blood cells.

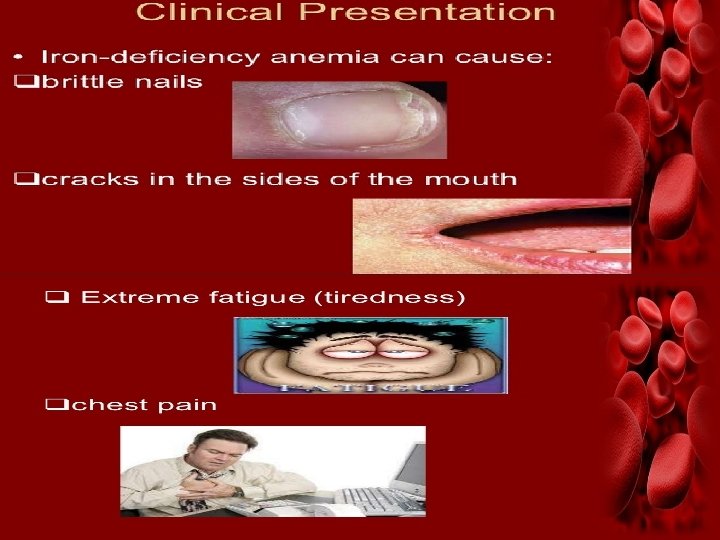
II-Microcytic hypochromic anemia e. g. Iron deficiency anemia Causes : 1 -Decreased iron intake: as in malnutrition and starvation. 2 - Decreased iron absorption: due to a) Decrease reducing substances that transform ferric iron into ferrous iron ( gastric HCl and vitamin C ) b) Presence of excess phytic acid (in tea), phosphates and oxalates which form insoluble compound with iron. c) Deficiency of bile which contain apotransferrin necessary for iron absorption. 3 - Decrease storage : as in liver disease. 4 -Increased requirement : as in pregnancy , lactation, rapid growth (infancy and puberty). 5 -Chronic blood loss: (repeated loss of small amount of blood for long period), as in: a) Gastrointestinal bleeding as bleeding peptic ulcer and piles b) Hematuria c) Excessive menstruation d) Ankylostoma infestation


Iron distribution Intracellular iron -Intracellular ferrous iron Heme iron compound : Hb, myoglobin Iron containing enzyme -Intracellular ferric iron RE cell, heart, epithelial cell of small intestine Extracellular iron -Ferric-transferrin

utilization Dietary iron 1 -2 mg/day Myoglobin 300 mg Liver 1000 mg Plasma transferrin 3 mg Slough mucosal cell 1 -2 mg/day Bone marrow 300 mg Erythrocyte 1800 mg Spleen 600 mg

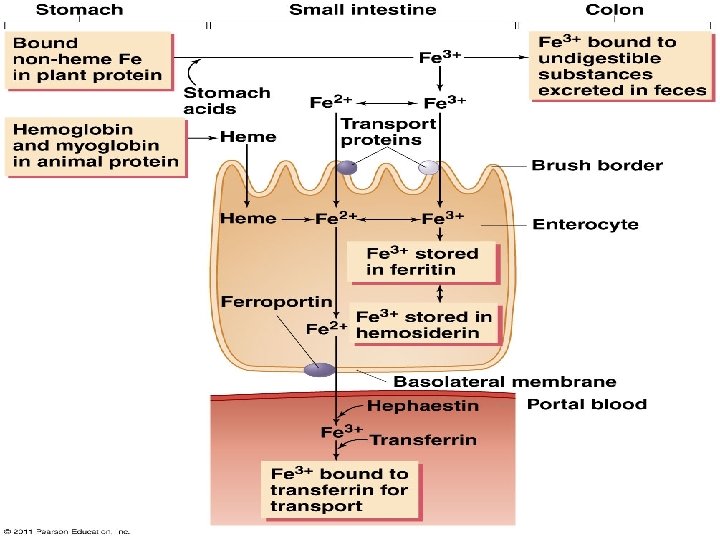
Iron absorption Promote absorption -Fructose Fe+++ -Vitamin C Fe++ -Heme iron -Amino acid HCl Inhibit absorption Fe++ -Phosphate -Phytate Fe++ ferritin -Tannin -Soil clay Fe+++ - transferrin

Iron absorption Main sites of absorbtion are; Duodenum Upper jejunum DMT-1: Divalent Metal Transporter -1
: -It is due to deficiency of vit B")
III- Macrocytic anemia (maturation failure anemia): -It is due to deficiency of vit B 12 or folic acid. -Both vit. B 12 and folic acid are essential for division of the erythroblast cells in the bone marrow. -Deficiency of either of these vitamins results in failure of the blast cell to divide , they cannot produce DNA quickly. -However they continue to grow forming large cells called megaloblast , which loose their nuclei to form large irregular fragile RBCs called megalocytes ( have a short life, one half to one third normal ) The hemoglobin content is normal, so these are normochromic anemias.

Vitamin B 12 is a water-soluble vitamin Functions of vitamin B 12 - Coenzyme for DNA synthesis - Maintains myelin sheath of nerve fibers - Metabolism of amino acid homocysteine Factors that alter vitamin B 12 digestion, absorption, and balance -Requires acidic medium (gastric HCl) and protein intrinsic factor in the gastric juice for its absorption. - After its combining with intrinsic factor it will be absorbed in ileum - Stored in the liver
 -")
Masking Vitamin B 12 deficiency -Causes of Vitamin B-12 deficiency (20% of elderly) - Abnormal gastric events (acid/enzymes) Deficient intrinsic factor (parietal cell destruction) Malabsorption syndromes Diet -B-12 associated Neurological symptoms - Posterolateral spinal cord degeneration -Paresthesias -Gait ataxia -Memory loss - Folic acid at elevated intakes (> 1 mg/day) masks B-12 deficiencyinduced hematological abnormalities w/o rescuing irreversible neurological symptoms.

Causes of Vit. B 12 deficiency: 1 - Decrease absorption : as in a- Decrease of the intrinsic factor due to atrophy of gastric mucosa, this is called pernicious anemia It is usually associated with neurological lesion called subacute combined degeneration of dorsal and lateral column of the spinal cord which leads to sensory and motor disturbances. b- Diseases of lower ileum which is the site of absorption. 2 - Decrease storage : as in liver diseases. 3 - Deficient intake : rare because the stored amount in liver is sufficient for 3 years. Causes of folic acid deficiency: 1 - Decreased intake as in starvation and malnutrition. 2 - Decreased absorption as in malabsorption , frequently occurring small intestinal disease called sprue, often have serious difficulty absorbing both folic acid and vitamin B 12 3 - Decreased storage as in chronic liver disease 4 - Increased requirements as in pregnancy.
 physiological effects: 1 - On C. V. S. a-")
Effects of anemia: (1 ) physiological effects: 1 - On C. V. S. a- Decrease of blood viscosity leads to decrease of peripheral resistance which leads to decrease diastolic blood pressure. b- Increase of venous return (due to vasodilatation from hypoxia leads to increase of cardiac output & systolic blood pressure c- Increase of the pulse pressure d- Increase of the heart rate and lastly may lead to heart failure 2 - Hypoxia i. e. anemic hypoxia that causes dyspnea on exertion. 3 - In hemolytic anemia there is increase of formation of bilirubin which leads to jaundice. 4 - In pernicious anemia, because vit. B 12 is important for metabolism of myelin sheath , there is subacute combined degeneration of the spinal cord. (2) Clinical effects: Pallor, palpitation, fatigue, fainting, headache and blurring of vision.
 To diagnose that there is anemia : we calculate")
Diagnosis of anemia: (A ) To diagnose that there is anemia : we calculate : 1 - RBCs count 2 - Hemoglobin content 3 - Hematocrit value (packed cell volume) All are decreased in anemia (B) To diagnose the type of anemia : We calculate the blood indices (hematological indices): 1 - Mean corpuscular volume (MCV) 2 - Mean corpuscular hemoglobin (MCH) 3 - Mean corpuscular hemoglobin concentration percent (MCHC) All blood indices are: 1 - Normal in normocytic normochromic anemia 2 - Decreased in microcytic hypochromic anemia 3 - MCV increased in macrocytic anemia
 To diagnose the cause of anemia: 1 -Blood film A) To see the")
(C) To diagnose the cause of anemia: 1 -Blood film A) To see the shape of RBCs e. g. -Spherocytes in spherocytosis -Sickle shaped in sickle cell anemia B) To detect the associated finding as : -Hypersegmented neutrophils in macrocytic anemia , -Pencil-shaped cells in iron deficiency anemia -(bite cells) in hemolytic anemia

2 - Estimation of serum bilirubin, hemolytic anemia is associated with increased serum bilirubin. 3 - Microcytic hypochromic anemia is essentially due to iron deficiency which can be confirmed by measuring plasma iron , transferrin & ferritin - Macrocytic anemia may be due to vit B 12 or folic acid deficiency can be differentiated by estimating their plasma level & RBC folate level. 5 -Reticulocytes % in the blood is usually 0. 5% to 2. 5% in adults and 2% to 6% in infants In a hemolytic anemia , there is high % of reticulocytes (there is an increased production of red blood cells). Low % reticulocytes can be found in aplastic anemia, pernicious anemia, various vitamin or mineral deficiencies (iron, vitamin B 12, folic acid )
; Text book of medical physiology, 12 th")
Resources -Guyton AC, and Hall JE (2010); Text book of medical physiology, 12 th ed. , W. B. Saunders Company -Ganong WF. (2012) ; Review of Medical Physiology, 24 th ed. , Lange Basic Science -Lauralee Sherwood (2012); Human physiology, from cell to system, 8 th ed. , Blackwell Press
- Slides: 35