Bleeding Disorders of Early Pregnancy Bleeding Disorders of

Bleeding Disorders of Early Pregnancy
 Abortion pregnancy")
Bleeding Disorders of Early Pregnancy n Abortion n Spontaneous n. A (non-intentional) Abortion pregnancy that ends before 20 weeks n Threatened Abortion n Light spotting; cervix is closed & no tissue is passed n Inevitable Abortion n Increased n Incomplete n Bleeding tissue bleeding & cervix dilates Abortion dilation of cervix & passage of
 n Abortion n Complete n Passage of all")
Bleeding Disorders of Early Pregnancy (continued) n Abortion n Complete n Passage of all products of conception, cervix closes and bleeding stops n Missed n Fetus dies in utero but is not expelled, uterine growth stops and spetis is possible n Recurrent n 2 or more consecutive spontaneous abortions

Induced Abortions n Therapeutic Abortion n Intentional termination of pregnancy before age of viability to preserve the health of the mother n Elective Abortion n Intentional termination of pregnancy for reasons unrelated to mothers health

Abortion

threatened incomplete inevitable missed

Nursing Care of Early Pregnancy Bleeding Disorders n n n Document amount and character of bleeding Save anything that looks like clots or tissue for evaluation by a pathologist Perineal pad count with estimated amount of blood per pad, such as 50% (could weight pads before/after) Monitor vital signs If actively bleeding, woman should be kept NPO in case surgical intervention is needed

Post-Abortion Teaching n n n Report increased bleeding Take temperature every 8 hours for 3 days Take an oral iron supplement if prescribed Resume sexual activity as recommended by the health care provider Return to health care provider at the recommended time for a checkup and contraception information Pregnancy can occur before the first menstrual period returns after the abortion procedure

Emotional Care Spiritual support from someone of the family’s choice and community support groups may help the family work through the grief of any pregnancy loss n Review effective and ineffective communication techniques found in Table 5 -4 on page 84 n

Effective Communication

Ectopic Pregnancy n n 95% occur in fallopian tube Scarring or tubal deformity may result from: n Hormonal abnormalities n Inflammation n Infection n Adhesions n Congenital defects n Endometriosis

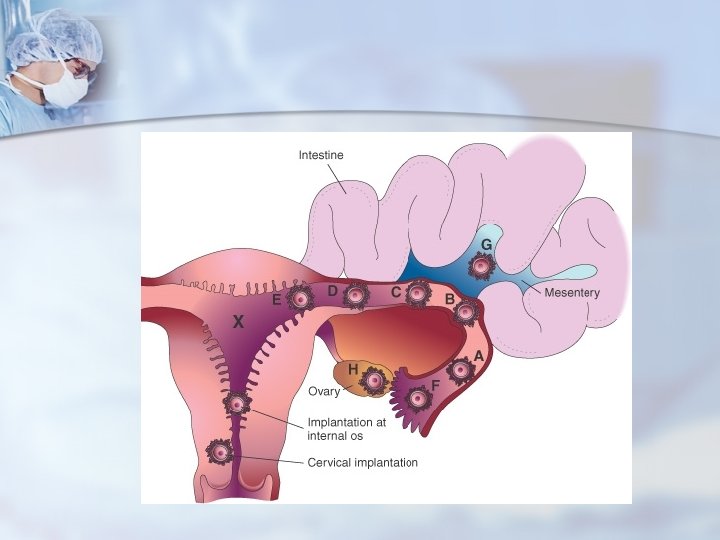
Ⅰ. Definition The blastcyst normally implants in the endometrial lining of the uterine cavity. Implantation anywhere else is an ectopic pregnancy. n It is one in which the fertilized ovum is implanted and developed outside of the uterine cavity. n

II. Incidence more than 1 in every 100 pregnancy III. Types of ectopic pregnancy Tubal Ovarian 95% 0. 5 -1% Cervical Abdominal Broad ligament
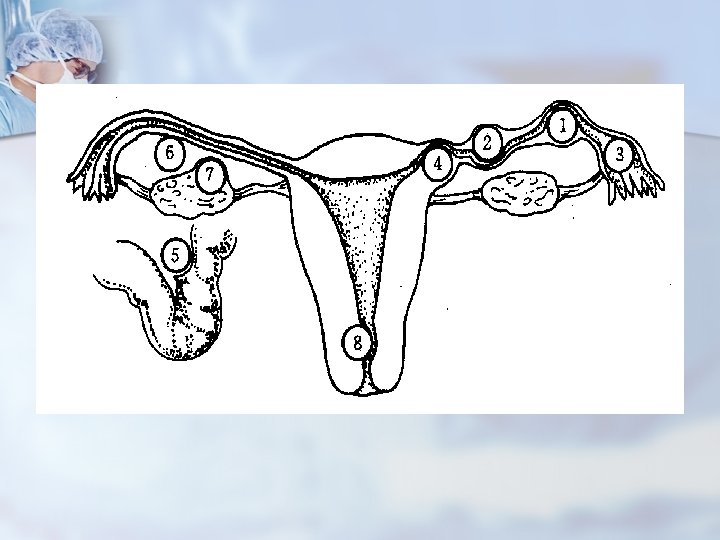

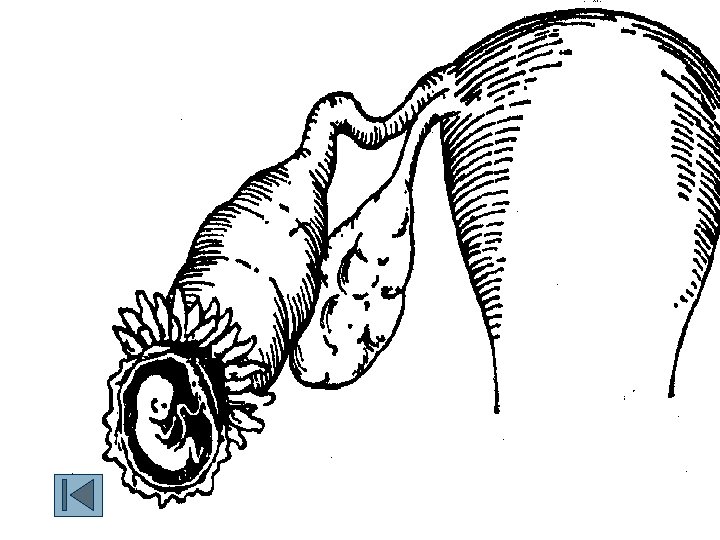
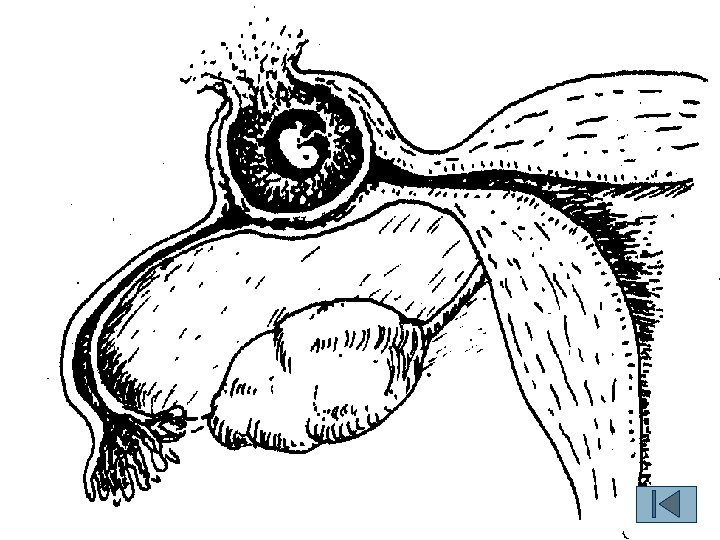
Ⅳ. Tubal pregnancy It is one of abdominal emergency. n Interabdominal hemorrhage sever hemorrhge shock died n 1. site n ※(1)Ampullar 60% (2)isthmic 25% (3)fimbrial 17% (4)Interstitial 2%~4%
amenorrhea n (2)low abdominal pain n (3)vaginal bleeding n (4)shock and collapse n")
Symptoms (1)amenorrhea n (2)low abdominal pain n (3)vaginal bleeding n (4)shock and collapse n
general condition n (2)abdominal examination n (3)pelvic examination ①the posterior fornix: tendness ②pain")
Signs (1)general condition n (2)abdominal examination n (3)pelvic examination ①the posterior fornix: tendness ②pain on motion of cervix ③uterus: 6~8 w size, soft, float ④a soft and elastic mass n
 n Clinical Presentation Amenorrhea Bleeding/Spotting Abdominal Pain")
Complications of Pregnancy n Ectopic Pregnancy (EP) n Clinical Presentation Amenorrhea Bleeding/Spotting Abdominal Pain
tubal abortion common in ampular tubal pregnancy (2)tubal")
A. tubal pregnancy n n n (1)tubal abortion common in ampular tubal pregnancy (2)tubal rupture: profuse hemorrhage common in isthmic TP: 6 w interstitial TP: 16 w (3)abdominal pregnancy
. Irregular")
n n n n n Clinical Manifestations Abdominal or pelvic pain (most common). Irregular vaginal bleeding — usually scanty and dark (most common). Amenorrhea”in 75% of the cases. Uterine size is usually similar to what it would be in a normally implanted pregnancy. Abdominal tenderness on palpation. Shoulder pain. Increased pulse and anxiety. Nausea, vomiting, faintness, or vertigo and syncope with abdominal pain may develop. Pelvic examination reveals a pelvic mass, posterior or lateral to the uterus, adnexal tenderness, and cervical pain on movement of the cervix.

5. Diagnosis Symptom Sign axillary examination
 pregnancy tests: β-HCG>25 u n quantitive serum β-HCG n (2) pelvic ultrasound n")
(1) pregnancy tests: β-HCG>25 u n quantitive serum β-HCG n (2) pelvic ultrasound n (3) the bloody fluid does not clot (4)laproscopy: diagnosis and treatment n (5)endometrial histology: Arias-Stella reaction n
 n Management n Pertinent n n n")
Complications of Pregnancy n Ectopic Pregnancy (EP) n Management n Pertinent n n n Missed menses Sexually active Previous EP, STD, surgery, etc. n Lower n quadrant pain/tenderness Avoid aggressive palpation/repeated exam n Vital n hx signs Orthostatic as appropriate n High flow O 2 n Treat for shock n n Position IV access n Surgical intervention usually required

Surgical Treatment n If woman does not consent to or meet criteria for methotrexate, surgical intervention is instituted. The surgical procedure depends on the extent of tubal involvement and if rupture has occurred. n n n The surgery of choice used to preserve future fertility is a salpingostomy. Should a woman not desire future fertility, the surgery of choice is salpingectomy. Other surgeries range from removal of ectopic pregnancy with tubal resection, salpingostomy (removes conceptus leaving tube intact, yet scarred), and possibly salpingooophorectomy. Treat shock and hemorrhage if necessary. Administer Rh. IG (immune globulin) per your facility's policy if woman is Rh negative.
 Complications Infertility n Hemorrhage and death n")
Ectopic Pregnancies (Continued) Complications Infertility n Hemorrhage and death n

Nursing Assessment n Evaluate the following to determine pregnancy and to monitor for changes in patient's status, such as rupture or hemorrhage: n Maternal vital signs n Presence and amount of vaginal bleeding n Amount and type of pain n Presence of abdominal tenderness on palpation/shoulder pain n Date of last menstrual period n Presence of positive pregnancy test n Rh type

Nursing Diagnoses n Risk for Deficient Fluid Volume related to blood loss from ruptured tube n Acute Pain related to ectopic pregnancy or rupture and bleeding into the peritoneal cavity n Anticipatory Grieving related to loss of pregnancy and potential loss of childbearing capacity

Nursing Interventions n Maintaining Fluid Volume n Establish an I. V. line with a large-bore catheter, and infuse fluids and packed RBCs as prescribed. n Obtain blood samples for complete blood count (CBC) and type and screen for whole blood, as directed. n Monitor vital signs and urine output frequently, depending on condition. n Promoting Comfort n Administer analgesics as needed and prescribed. n Encourage the use of relaxation techniques.
 n Also known as Gestational Trophoblastic Disease n Occurs when")
Hydatidiform Mole (Molar Pregnancy) n Also known as Gestational Trophoblastic Disease n Occurs when chorionic villi abnormally increase and develop vesicles n May cause hemorrhage, clotting abnormalities, hypertension, and later development of cancer n More likely to occur in women at age extremes of the reproductive life

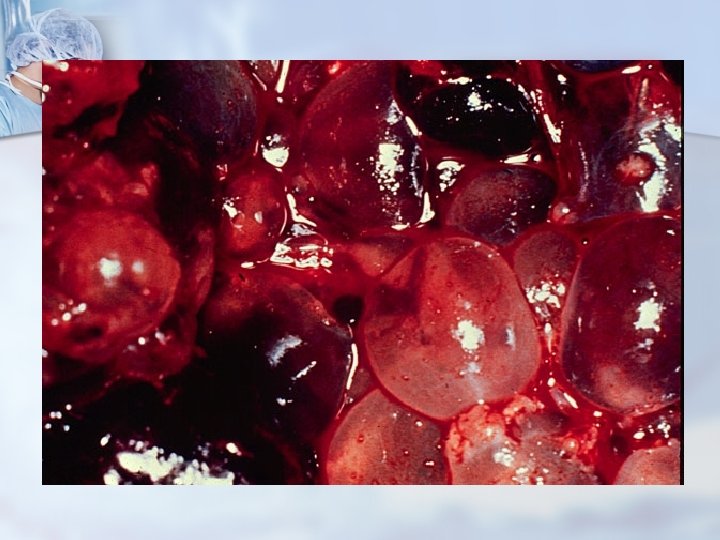

 n Manifestations n Bleeding n Rapid uterine growth n Failure to")
Hydatidiform Mole (Continued) n Manifestations n Bleeding n Rapid uterine growth n Failure to detect fetal heart activity n Signs of hyperemesis gravidarum n Unusually early development of GH n Higher than expected levels of h. CG n A distinct “snowstorm” pattern on ultrasound with no evidence of a developing fetus n Treatment n n Uterine evacuation Dilation and evacuation

Management n Suction curettage is the method of choice for immediate evacuation of the mole with possibility of laparotomy. n Follow-up for detection of malignant changes because a complication is the development of choriocarcinoma of the endometrium.

Nursing Assessment n Monitor maternal vital signs; note presence of hypertension. n Assess the amount and type of vaginal bleeding; note the presence of any other vaginal discharge. n Assess the urine for the presence of protein. n Palpate uterine height; if above the umbilicus, measure the fundal height. n Determine date of last menstrual period and date of positive pregnancy test. n Evaluate CBC results and Rh type.

Nursing Interventions n Maintaining Fluid Volume n Obtain blood samples for type and screen, and have 2 to 4 units of whole blood available for possible replacement. n Establish and maintain I. V. line; start with a large needle to accommodate possible transfusion and large quantities of fluid. n Assess maternal vital signs, and evaluate bleeding. n Monitor laboratory results to evaluate patient's status. n Decreasing Anxiety n Prepare the patient for surgery. Explain preoperative and postoperative care along with intraoperative procedures. n Educate patient and family on the disease process. n Allow the family to grieve over the loss of the pregnancy.

n n n Patient Education and Health Maintenance Advise the woman on the need for continuous follow-up care. Provide reinforcement of follow-up procedures: n n n Measure-h. CG levels every 1 to 2 weeks until normal — then begin monthly testing for 6 months, then every 2 months for a total of 1 year. Consider chemotherapy or hysterectomy if -h. CG levels rise or begin to plateau or there is evidence of metastasis. Encourage ongoing discussion of care with health care provider
- Slides: 40