BLEEDING DISORDERS Dr Rashmi HEMOSTASIS 1 VASCULAR PHASE

BLEEDING DISORDERS Dr. Rashmi

HEMOSTASIS 1. VASCULAR PHASE 2. PLATELET PHASE 3. COAGULATION PHASE 4. FIBRINOLYTIC PHASE

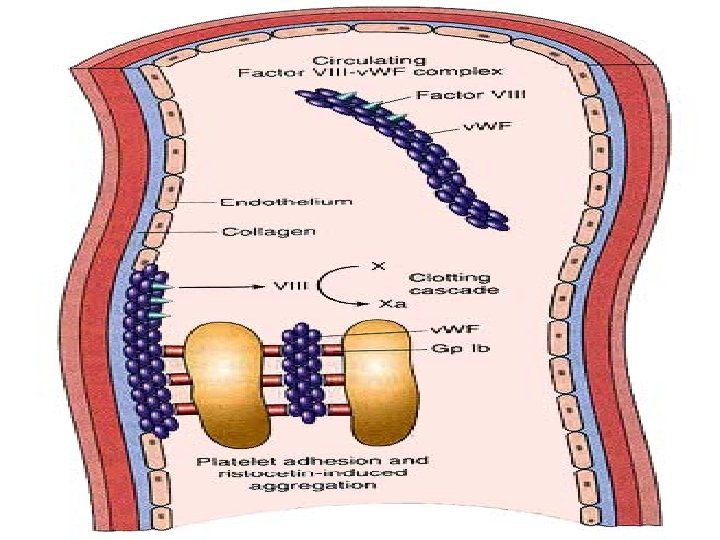
NORMAL CLOTTING Response to vessle injury 1. Vasoconstriction to reduce blood flow 2. Platelet plug formation (von willebrand factor binds damaged vessle and platelets) 3. Activation of clotting cascade with generation of fibrin clot formation 4. Fibrinlysis (clot breakdown)

CLOTTING CASCADE Normally the ingredients, called factors, act like a row of dominoes toppling against each other to create a chain reaction. If one of the factors is missing this chain reaction cannot proceed.

VASCULAR PHASE WHEN A BLOOD VESSEL IS DAMAGED, VASOCONSTRICTION RESULTS.

PLATELET PHASE PLATELETS ADHERE TO THE DAMAGED SURFACE AND FORM A TEMPORARY PLUG.

COAGULATION PHASE THROUGH TWO SEPARATE PATHWAYS THE CONVERSION OF FIBRINOGEN TO FIBRIN IS COMPLETE.

THE CLOTTING MECHANISM INTRINSIC Collagen EXTRINSIC Tissue Thromboplastin XII XI IX VIII VII X FIBRINOGEN (I) V PROTHROMBIN (II) THROMBIN (III) FIBRIN

FIBRINOLYTIC PHASE ANTICLOTTING MECHANISMS ARE ACTIVATED TO ALLOW CLOT DISINTEGRATION AND REPAIR OF THE DAMAGED VESSEL.

HEMOSTASIS DEPENDENT UPON: Vessel Wall Integrity Adequate Numbers of Platelets Proper Functioning Platelets Adequate Levels of Clotting Factors Proper Function of Fibrinolytic Pathway
 Prothrombin time (PT) Partial")
LABORATORY EVALUATION • • • Platelet count Bleeding time (BT) Prothrombin time (PT) Partial thromboplastin time (PTT) Thrombin time (TT)

PLATELET COUNT NORMAL 100, 000 - 400, 000 CELLS/MM 3 < 100, 000 Thrombocytopenia 50, 000 - 100, 000 Mild Thrombocytopenia < 50, 000 Sev Thrombocytopenia

BLEEDING TIME l PROVIDES ASSESSMENT OF PLATELET COUNT AND FUNCTION NORMAL VALUE 2 -8 MINUTES

PARTIAL THROMBOPLASTIN TIME l Measures Effectiveness of the Intrinsic Pathway l Mnemonic - PITT NORMAL VALUE 25 -40 SECS

PROTHROMBIN TIME l Measures Effectiveness of the Extrinsic Pathway l Mnemonic - PET NORMAL VALUE 10 -15 SECS

THROMBIN TIME • Time for Thrombin To Convert Fibrinogen Fibrin • A Measure of Fibrinolytic Pathway NORMAL VALUE 9 -13 SECS

So What Causes Bleeding Disorders? p. VESSEL DEFECTS p. PLATELET DISORDERS p. FACTOR DEFICIENCIES p. OTHER DISORDERS ? ?

VESSEL DEFECTS q VITAMIN C DEFICIENCY q BACTERIAL & VIRAL INFECTIONS q ACQUIRED & q. HEREDITARY CONDITIONS
")
l Infectious and hypersensitivity vasculitides - Rickettsial and meningococcal infections - Henoch-Schonlein purpura (immune)

PLATELET DISORDERS p THROMBOCYTOPENIA p THROMBOCYTOPATHY

THROMBOCYTOPENIA INADEQUATE NUMBER OF PLATELETS

THROMBOCYTOPATHY ADEQUATE NUMBER BUT ABNORMAL FUNCTION

THROMBOCYTOPENIA l DRUG INDUCED l BONE MARROW FAILURE l HYPERSPLENISM l OTHER CAUSES
")
OTHER CAUSES FLymphoma FHIV Virus FIdiopathic Thrombocytopenia Purpura (ITP)

THROMBOCYTOPATHY Uremia Inherited disorders Myeloproliferative disorders Drug induced
 Hemophilia A Hemophilia B von Willebrand’s disease")
FACTOR DEFICIENCIES (CONGENITAL) Hemophilia A Hemophilia B von Willebrand’s disease
 • 80 -85% of all Hemophiliacs • Deficiency")
FACTOR DEFICIENCIES HEMOPHILIA A (Classic Hemophilia) • 80 -85% of all Hemophiliacs • Deficiency of Factor VIII • Lab Results - Prolonged PTT HEMOPHILIA B (Christmas Disease) • 10 -15% of all Hemophiliacs • Deficiency of Factor IX • Lab Test - Prolonged PTT

FACTOR DEFICIENCIES VON WILLEBRAND’S DISEASE Deficiency of VWF & amount of Factor VIII Lab Results - Prolonged BT, PTT
 Oral anticoagulants COUMARIN HEPARIN Liver disease Malabsorption Broad spectrum antibiotics")
OTHER DISORDERS (ACQUIRED) Oral anticoagulants COUMARIN HEPARIN Liver disease Malabsorption Broad spectrum antibiotics

INHIBITORS 30% of people with haemophilia develop an antibody to the clotting factor they are receiving for treatment. These antibodies are known as inhibitors. These patients are treated with high does of FVIIa for bleeds or surgery. This overrides defect in FVIII or FIX deficiency. Longterm management involves attempting to eradicate inhibitors by administering high dose FVIII (or FIX) in a process called immune tolerance


Coagulation factor disorders • Inherited bleeding disorders – Hemophilia A and B – von. Willebrands disease – Other factor deficiencies • Acquired bleeding disorders – Liver disease – Vitamin K deficiency/warfarin overdose – DIC

Hemophilia A and B Hemophilia A Hemophilia Factor VIII Factor IX X-linked recessive 1/10, 000 males 1/50, 000 B Coagulation factor deficiency Inheritance Incidence males Severity Related to factor level <1% - Severe - spontaneous bleeding 1 -5% - Moderate - bleeding with mild injury
 Hemarthrosis (most common) Fixed joints")
Hemophilia Clinical manifestations (hemophilia A & B are indistinguishable) Hemarthrosis (most common) Fixed joints Soft tissue hematomas (e. g. , muscle) Muscle atrophy Shortened tendons Other sites of bleeding Urinary tract CNS, neck (may be life-threatening) Prolonged bleeding after surgery or dental extractions
")
Hemarthrosis (acute)

Treatment of hemophilia A • Intermediate purity plasma products – Virucidally treated – May contain von Willebrand factor • High purity (monoclonal) plasma products – Virucidally treated – No functional von Willebrand factor • Recombinant factor VIII – Virus free/No apparent risk – No functional von Willebrand factor

von Willebrand Disease: Clinical Features • von Willebrand factor – – – Synthesis in endothelium and megakaryocytes Forms large multimer Carrier of factor VIII Anchors platelets to subendothelium Bridge between platelets • Inheritance - autosomal dominant • Incidence - 1/10, 000 • Clinical features - mucocutaneous bleeding

Laboratory evaluation of von Willebrand disease • Classification – Type 1 – Type 2 – Type 3 Partial quantitative deficiency Qualitative deficiency Total quantitative deficiency • Diagnostic tests: von. Willebrand type 2 Assay 3 1 v. WF antigen ßß v. WF activity ßß Multimer analysis ß Normal ß ß Normal

Treatment of von Willebrand Disease • Cryoprecipitate – Source of fibrinogen, factor VIII and VWF – Only plasma fraction that consistently contains VWF multimers • DDAVP (deamino-8 -arginine vasopressin) – plasma VWF levels by stimulating secretion from endothelium – Duration of response is variable – Not generally used in type 2 disease – Dosage 0. 3 µg/kg q 12 hr IV • Factor VIII concentrate (Intermediate purity) – Virally inactivated product


Common clinical conditions associated with Disseminated Intravascular Coagulation Activation of both coagulation and fibrinolysis Triggered by • Sepsis • Trauma – Head injury – Fat embolism • Malignancy • Obstetrical complications – Amniotic fluid embolism – Abruptio placentae • Vascular disorders • Reaction to toxin (e. g. snake venom, drugs) • Immunologic disorders – Severe allergic reaction – Transplant rejection
 Mechanism Systemic activation of coagulation Intravascular deposition of fibrin Thrombosis")
Disseminated Intravascular Coagulation (DIC) Mechanism Systemic activation of coagulation Intravascular deposition of fibrin Thrombosis of small and midsize vessels with organ failure Depletion of platelets and coagulation factors Bleeding

Pathogenesis of DIC Release of thromboplastic material into circulation Coagulation Fibrinolysis Fibrinogen Plasmin Thrombin Fibrin Monomers Fibrin Clot (intravascular) Consumption of coagulation factors; presence of FDPs a. PTT PT TT Fibrinogen Presence of plasmin FDP Fibrin(ogen) Degradation Products Plasmin Intravascular clot Platelets Schistocytes

Disseminated Intravascular Coagulation Treatment approaches • Treatment of underlying disorder • Anticoagulation with heparin • Platelet transfusion • Fresh frozen plasma • Coagulation inhibitor concentrate (ATIII)

Classification of platelet disorders • Quantitative disorders – Abnormal distribution – Dilution effect – Decreased production – Increased destruction • Qualitative disorders – Inherited disorders (rare) – Acquired disorders • Medications • Chronic renal failure • Cardiopulmonary bypass

Thrombocytopenia Immune-mediated Idioapthic Drug-induced Collagen vascular disease Lymphoproliferative disease Sarcoidosis Non-immune mediated DIC Microangiopathic hemolytic anemia

Liver Disease and Hemostasis 1. 2. 3. 4. 5. 6. Decreased synthesis of II, VII, IX, X, XI, and fibrinogen Dietary Vitamin K deficiency (Inadequate intake or malabsortion) Dysfibrinogenemia Enhanced fibrinolysis (Decreased alpha-2 -antiplasmin) DIC Thrombocytoepnia due to hypersplenism

Laboratory Evaluation of Bleeding Overview CBC and smear Platelet count RBC and platelet morphology Thrombocytopenia TTP, DIC, etc. Coagulation Prothrombin time Partial thromboplastin time Coagulation factor assays 50: 50 mix Fibrinogen assay Thrombin time Extrinsic/common pathways Intrinsic/common pathways Specific factor deficiencies Inhibitors (e. g. , antibodies) Decreased fibrinogen Qualitative/quantitative fibrinogen defects Fibrinolysis (DIC) FDPs or D-dimer Platelet function disorders von Willebrand factor Bleeding time Platelet function analyzer (PFA) Platelet function tests v. WD In vivo test (non-specific) Qualitative platelet and v. WD Qualitative platelet
 Prothrombin time (PT) Surface")
Laboratory Evaluation of the Coagulation Pathways Partial thromboplastin time (PTT) Prothrombin time (PT) Surface activating agent (Ellagic acid, kaolin) Phospholipid Calcium Thromboplastin Tissue factor Phospholipid Calcium Intrinsic pathway Extrinsic pathway Thrombin time Common pathway Thrombin Fibrin clot

Coagulation factor deficiencies Summary Sex-linked recessive Factors VIII and IX deficiencies cause bleeding Prolonged PTT; PT normal Autosomal recessive (rare) Factors II, V, VII, X, XI, fibrinogen deficiencies cause bleeding Prolonged PT and/or PTT Factor XIII deficiency is associated with bleeding and impaired wound healing PT/ PTT normal; clot solubility abnormal Factor XII, prekallikrein, HMWK deficiencies do not cause bleeding

Thrombin Time • Bypasses factors II-XII • Measures rate of fibrinogen conversion to fibrin • Procedure: – Add thrombin with patient plasma – Measure time to clot • Variables: – Source and quantity of thrombin

Causes of prolonged Thrombin Time • • • Heparin Hypofibrinogenemia Dysfibrinogenemia Elevated FDPs or paraprotein Thrombin inhibitors (Hirudin) Thrombin antibodies

Classification of thrombocytopenia • Associated with thrombosis – Thrombotic thrombocytopenic purpura – Heparin-associated thrombocytopenia – Trousseau’s syndrome – DIC • Associated with bleeding – Immune-mediated thrombocytopenia (ITP) – Most others

Bleeding time and bleeding • 5 -10% of patients have a prolonged bleeding time • Most of the prolonged bleeding times are due to aspirin or drug ingestion • Prolonged bleeding time does not predict excess surgical blood loss • Not recommended for routine testing in preoperative patients

- Slides: 56