Bleeding control in ED focusing on multiple trauma

Bleeding control in ED : focusing on multiple trauma 부산대학교병원 염 석 란

Acute Massive Hemorrhage in ER • Multiple trauma - peritoneal cavity : liver, spleen, kidney, mescenteric vvs - thoracic cavity : massive hemothorax - open wound : street - retroperitoneal space : pelvic fracture • Obstetric bleeding – PPH • GI Bleeding
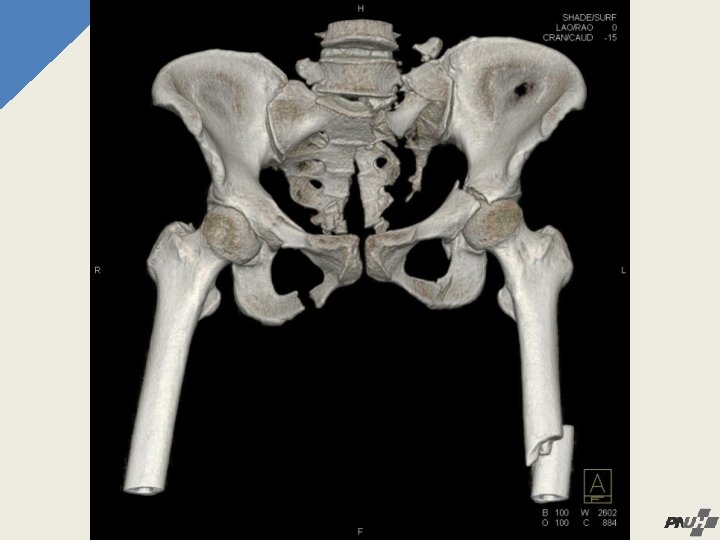

Importance 1. Complex anatomic relation, pathway of nerves and vessels networks – hemorrhagic shock 2. Substantial force. 3. Many internal organs 4. Connects to abdominal and retroperitoneal space

Classification of pelvic bone fracture 1. Tile/AO classification Type A stable fractures Type B rotationally unstable fractures Type C rotationally and vertically unstable fractures 2. Young and Burgess’s modified classification APC (anterior-posterior compression) LC (lateral compression) VS (vertical shear) CM (combined mechanism)


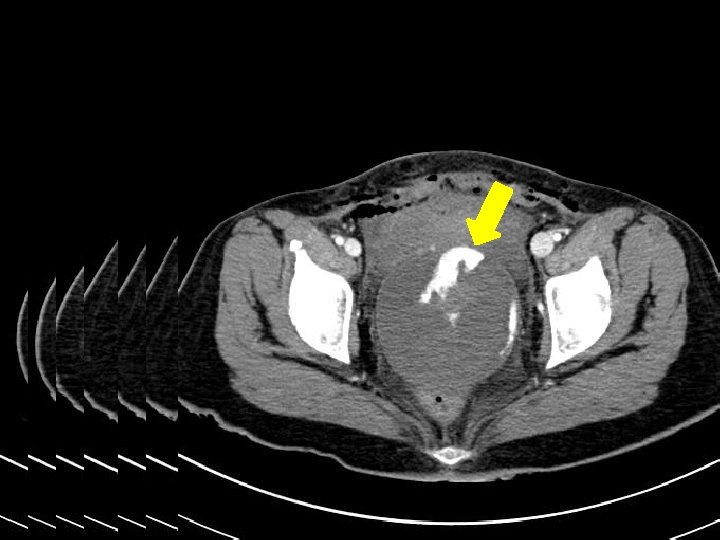
Diagnosis 1. General: external wound over bony prominence of pelvis, scrotal, vulvar hematoma. 2. PE: DRE - Rectal vaginal laceration 3. X-ray – pelvis AP, inlet & outlet view, 4. CT poor correlation between the severity of the pelvic fracture pattern and the need for emergent haemostasis

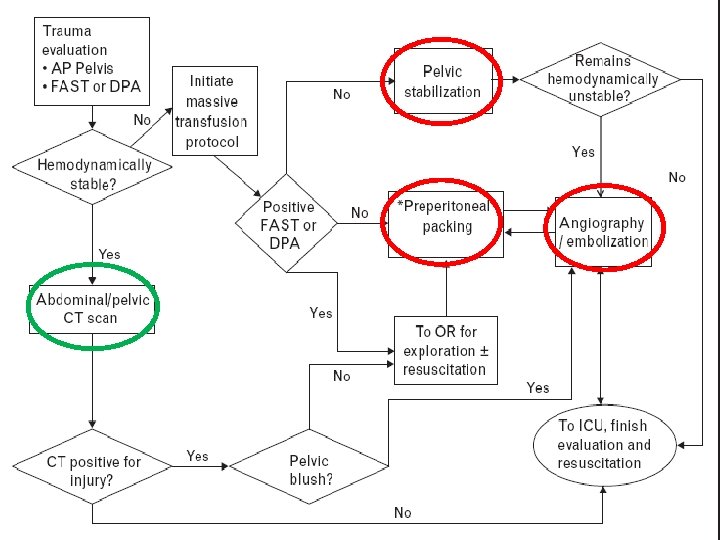
Management • Overall mortality of pelvic bone fracture : 5% • Haemodynamically unstable pelvic fractures mortality : 40 -60%. • Open pelvic fractures : 70% (loss of the self-tamponade effect) • 90% of unstable pelvic fractures - associated injuries • 50% - major haemorrhage other than pelvic fractures Principle of management – shock management, bleeding control

Management • Requiring 4 units↑of blood transfusion within 24 h or 6 units↑ within 48 h aggressive haemostasis • Recurrence of hypotension within 2 h of an initially successful resuscitation pelvic angiography • Patients older than 60 years Higher likelihood of need for advanced haemostasis

Management • • MAST Pelvic binder or sheet wrapping External fixation C-clamps Pelvic packing Angiography & embolization Medical Therapy

MAST

Pelvic Binder

Pelvic Binder

External fixation • In 1897, Parkhill - initial concept of EX-FIX Slatis and • Karharjuin 1973 - a simple trapezoidal frame. • the anterior external fixator - stabilize anterior disruption but intact posterior elements • Fracture patterns - Tile type B - Young and Burgess APC-2 and LC-1, -2, -3 • ‘Open book’ - external fixator (provides rotational stability)

External fixation • Hemodynamically unstable with an unstable pelvic fracture polytraumatized patient, unless another measure external fixator immediately • Negative DPL with hemodynamic instability with unstable pelvic fracture • Vertically unstable fracture - add skeletal traction <Techniques in Orthopaedics®, Vol. 17, No. 02, 2002>

External fixation

C-Clamp • A form of external fixation. • Quickly placement without fluoroscopic control • One advantage - posteriorly for direct reduction of vertically and rotationally unstable fractures • By inserting a wide pin bilaterally in the region of the sacroiliac joints

Bilateral iliac arteries ligation • 1964 yr • 28 underwent damage control iliac artery ligation and pelvic packing. The mortality rate 64% <Dubose J, Inaba K, Barmparas G, et al. J Trauma 2010>

Pelvic packing • Direct surgical management • Direct retroperitoneal packing via transabdominal approach • 1979 y • Relatively invasive, blood loss significant

Preperitoneal pelvic packing • rapid method for controlling pelvic fracture-related hemorrhage • Easy to perform • Less invasive • Minimal blood loss • supplant the need for emergent angiography. • significant reduction of transfusion

Preperitoneal pelvic packing • Relative invasive, compare to angio • Infection risk ↑ • Abdominal compartment sysdrome↑

Angiography & Embolization • Initially described as early as 1972 • Effective means on arterial hemorrhage • patients who remain haemodynamically unstable after appropriate fluid resuscitation, transfusion and mechanical stabilization of the pelvis • Extravasation of contrast medium on arterial phase of CT the pelvic angiography

Drug therapy for acute bleeding - the usage of recombinant factor VII

Consumptive Coagulopathy Massive Transfusion Metabolic Acidosis Hypothermia Electrolyte imbalance Dilutional Coagulopathy

Drug therapies for traumatic bleeding control in Korea • tranexamic acid • ε-aminocaproic acid – not available in Korea • aprotinin - Korean FDA cancelled the approval with 2008 June 10 th

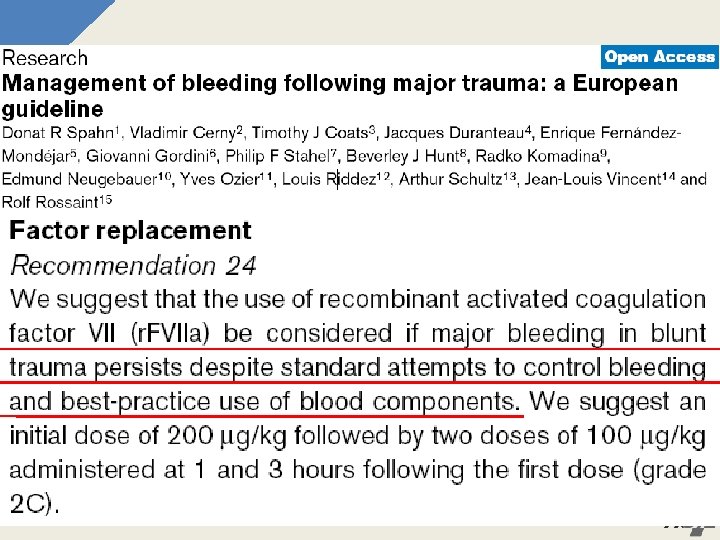
Drug therapies for traumatic bleeding control in Korea • recombinant activated factor VII - ? ? (r. FVIIa; Novo. Seven, Nordisk, Denmark) • r. FVIIa is coming into spotlight in the management of trauma patients.

Intrinsic Pathway Extrinsic Pathway factor XII HMK factor XIa factor IXa factor VIIIa factor X factor VIIa Tissue Factor factor Xa factor Va prothrombin fibrinogen factor X thrombin fibrin
 • Platelet adhesion (within")
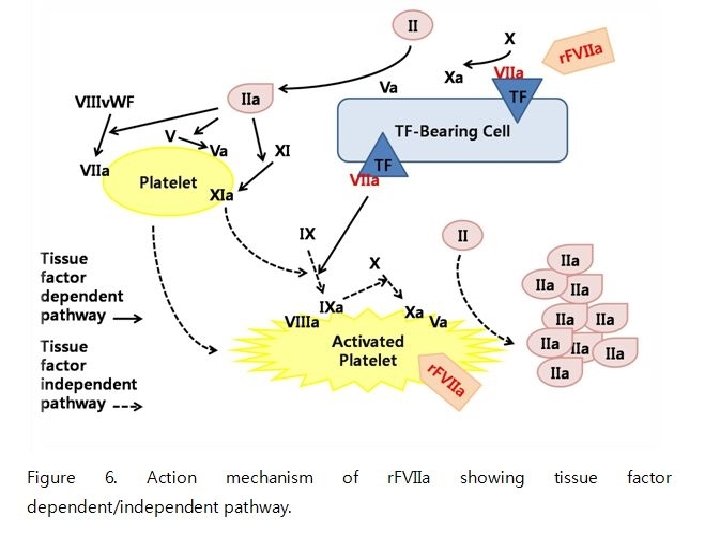
The haemostatic system: three phases Primary haemostasis: • Vasoconstriction (immediate) • Platelet adhesion (within seconds) • Platelet aggregation and contraction (within minutes) Secondary haemostasis: • Activation of coagulation factors (within seconds) • Formation of fibrin (within minutes) Fibrinolysis: • Activation of fibrinolysis (within minutes) • Lysis of the plug (within hours) Haemostasis and r. FVIIa mode of action; Feb 2006
 dependent pathway of hemostasis")
Recombinant Factor Vlla • Enhancing the normal FVIIa –Tissue factor(TF) dependent pathway of hemostasis

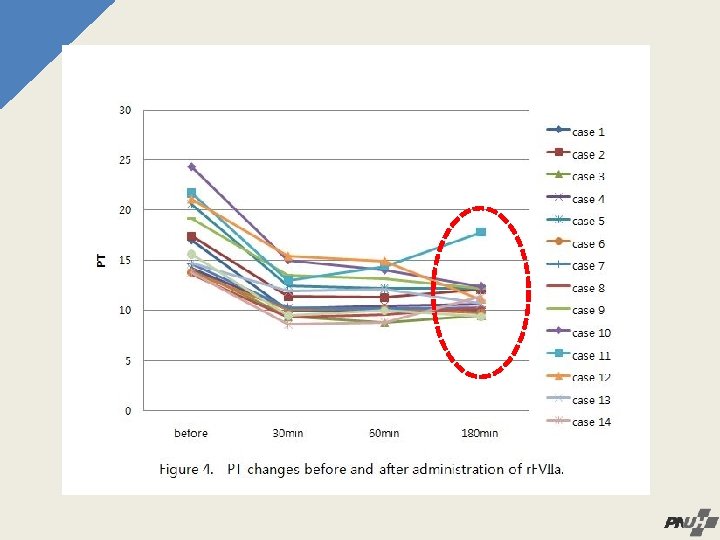
15 trauma cases received r. FVIIa in Korea • 2007. 03 - 2010. 01 • Hypovolemic shock due to trauma • Administration of a single dose of recombinant activated factor VII, 4. 8 mg, 240 KIU(r. FVIIa; Novo. Seven, Nordisk, Denmark) • No surgical or interventional management except for just 2 cases

Information of 15 cases No. Case Sex Age ICISS Mechanism Major bleeding sources 1 M 48 0. 793 10 m. FD Thorax, retroperitoneum, long bone 2 M 24 0. 735 5 th floor Thorax, peritoneum, retroperitoneum, long bone 3 M 33 0. 869 7 m. FD Retroperitoneum 4 M 56 0. 665 6 th floor FD Thorax, peritoneum, retroperitoneum, long bone 5 F 48 0. 863 3 th floor FD Thorax, retroperitoneum, long bone 6 M 26 0. 796 4 th floor FD Long bone, face 7 M 53 0. 864 Crash Retroperitoneum 8 M 32 0. 812 Driver, FD Thorax, peritoneum 9 M 63 0. 736 Pedestrian Thorax, peritoneum, retroperitoneum, long bone 10 F 69 0. 723 Pedestrian Thorax, peritoneum, retroperitoneum, long bone 11 M 61 0. 788 Pedestrian Thorax, peritoneum, long bone 12 M 50 0. 891 Crash Peritoneum, retroperitoneum 13 F 43 0. 842 5 m. FD Thorax, peritoneum, retroperitoneum, long bone 14 F 28 4 th floor FD Peritoneum, retroperitoneum 15 F 69 0. 841 0. 720 Pedestrian Retroperitoneum Abbreviations: FD, fall down

Case 1

Case 2 2

Case 44 4

Case 6 6

Case 8

Case 1210

Transfusion rates No. Case Time to rⅦa Pre p. RBC* Pre p. RBC rate Post p. RBC† Post (hour) (Unit/hour) (Unit) 1 18. 33 12 0. 65 0 2 7. 22 5 0. 69 0 3 2. 33 3 1. 29 0 4 3. 00 8 2. 67 3 5 11. 83 8 0. 68 3 6 2. 00 9 4. 50 0 7 6. 50 6 0. 92 0 8 18. 66 3 0. 16 3 9 1. 00 6 6. 00 0 10 3. 50 8 2. 29 0 11 5. 42 12 2. 21 10 12 1. 20 6 5. 00 0 13 2. 40 3 1. 25 0 14 3. 75 3 0. 80 0 15 4. 00 3 0. 75 2 *Units of p. RBC transfused before administration of rⅦa †Units of p. RBC transfused during six hours after administration of rⅦa p. RBC rate 0. 00 0. 50 0. 00 1. 67 0. 00 0. 33

Transfused blood volume/hour

r. FVIIa controls life threatening bleeding in nonhaemophiliac patient in 1999: Rationale for moving into trauma

§ In blunt trauma, r. FVIIa: - Significantly reduced the number of RBC transfusions - Significantly reduced the need for >20 units of RBC § In the penetrating trauma population: - No statistically significant RBC reduction - A trend towards reduction in massive transfusion Boffard KD et al. J Trauma 2005; 59(1): 8 -18
 F/28 yrs CC Decreased Mentality VS 측정 안됨")
Postpartum hemorrhage in Korea (3 cases) F/28 yrs CC Decreased Mentality VS 측정 안됨 – 155 – 30 – 35. 5 P I Uncontrolled bleeding after C-sec 18: 00 Initial transfusion PC/FFP – 6/6 60/6? -144 after 1 hr Checked Abdominal CT
 in angio room 22: 40 Emergency Angiography & embolization")
progress 22: 00 Transfused PC/FFP/PLT(6/6/16) in angio room 22: 40 Emergency Angiography & embolization Transfused PC/FFP/PLT (6/6/8) Admitted to ICU 23: 50 massive vaginal Bleeding 1000 ml/hr Transfused PC/FFP (8/11) HD#2 00: 50 Recombinant activated FVII 4. 8 mg IV ~02: 00 Decreased vaginal bleeding 100 ml/hr ~06: 00 Transfued PC/FFP (2/4)
 19: 30 10: 40 (Post. Angio) 00: 50 (ICU)")
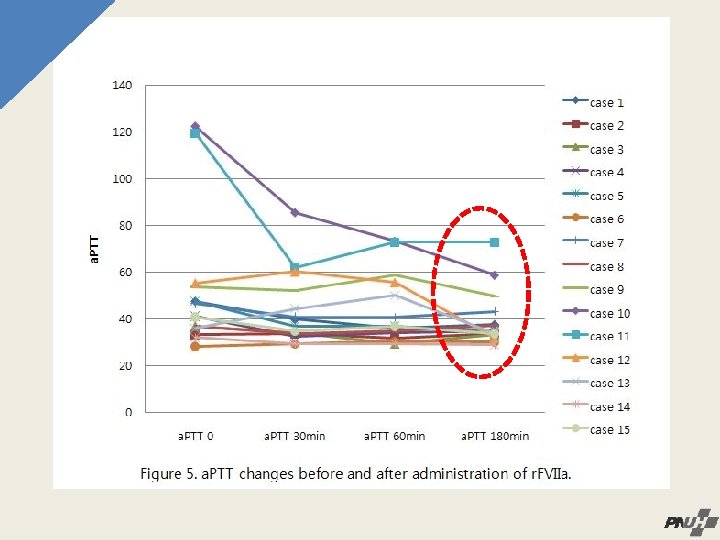
Time 18: 00 (Admit ) 19: 30 10: 40 (Post. Angio) 00: 50 (ICU) r. FVIIa ↓ 01: 50 04: 30 Hemoglobin (g/d. L) 8. 4 9. 1 8. 5 7. 3 9. 4 9. 1 Platelet (109/L) 18 36 151 89 96 97 PT (sec) 14. 6 19. 1 16. 3 16. 0 4. 8 mg, (240 KI U) iv at 00: 50 9. 3 9. 6 INR 1. 29 1. 73 1. 48 1. 45 0. 87 a. PTT (sec) 50. 0 108. 0 68. 9 71. 9 44. 9 42. 7 Resuscitation 26 PRBC, 29 FFP, 26 PLT 2 PRBC, 4 FFP

• Recombinant factor Ⅶa is effective for control of trauma induced hemorrhage, postpartum hemorrhage. • Reducing transfusion volume • Improving the coagulation status • Rapid decision on administration of the drug is important for maximizing the effectiveness.

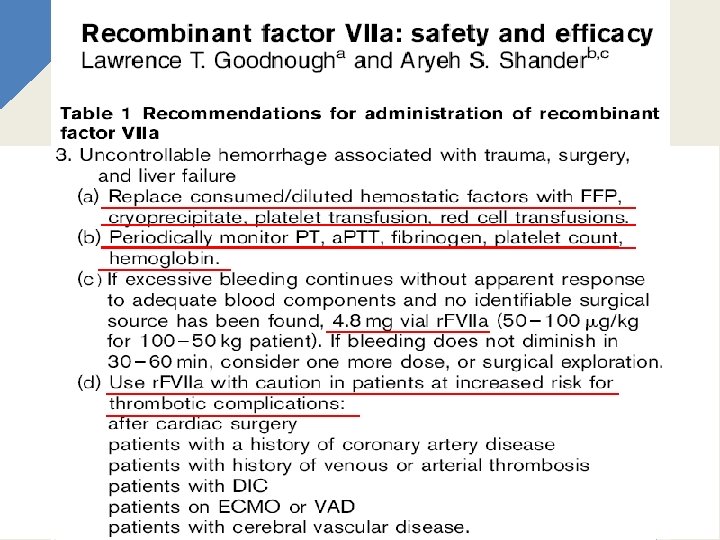
• High cost, Cost-effectiveness • Off-labeled indication • Thromboembolic complication • In the future, the good therapeutics on the management of critical bleeding in the trauma patient in korea.

Thank you! *^^*
- Slides: 55