Bladder physiology and incontinence Bladder physiology Lower urinary

Bladder physiology and incontinence

Bladder physiology Lower urinary tract is composed of bladder and urethra and prostate in male The two function of LUT are urinary storage and urinary emptying These function depend on integrated function of CNS, PNS, urinary bladder and urethra

- filling phase requiresincreasing urine volume at low detrusor pressure, closed sphincters, absence of involuntary bladder contraction - In voiding phase: -coordinated contraction of bladder muscle with concomitant decrease of resistance at level of smooth and striated sphincters ( synergy)

• During bladder filling the pressure remains low despite increase in volume because the bladder is highly compliant organ • Compliance is the change in volume/change in pressure • The bladder is compliant due to viscoelasticity of connective tissue and muscle bundles, where there will be rearrangement of these tissue to accommodate urine at low pressure

• Low compliance may be the result of : • Change of composition (more collagen and less elastin) like what happen in chronic inflammation, BOO, neurological decentralization • Hypertrophic muscle is less compliant •

Compiance - Change in vol / change in pressue

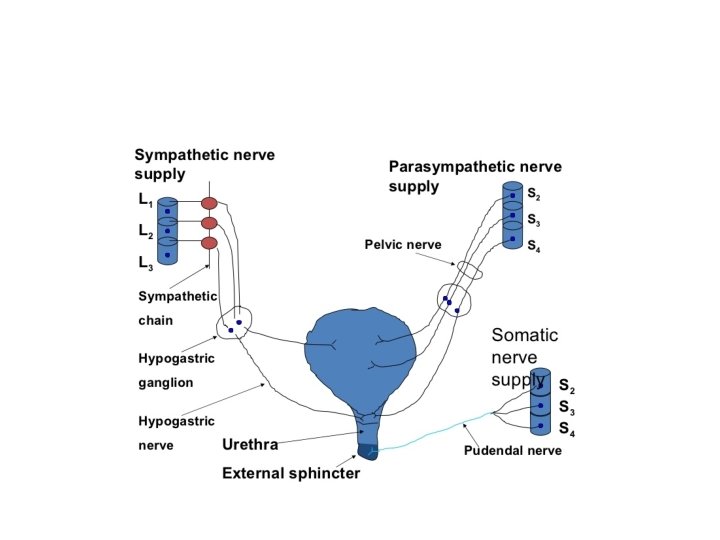
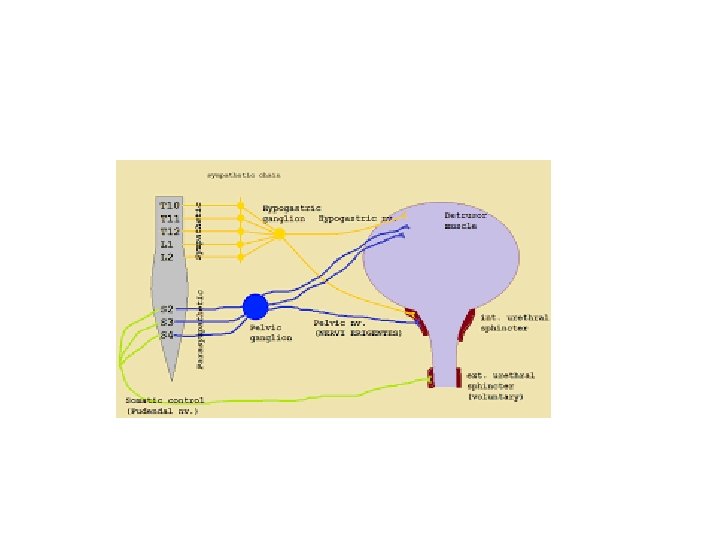
• Voiding when there is synergic contraction of bladder detrusor muscle and relaxation of the sphincter • The smooth muscle of the bladder (detrusor muscle) is innervated by parasympathetic • Afferent innervation which sense bladder filling ascend with parasympathetic to the cord and then to pontine micturition center (barringtons nucleus) • the pons center receive input from other brain area , if the time is appropriate for voiding it will stimulate voiding

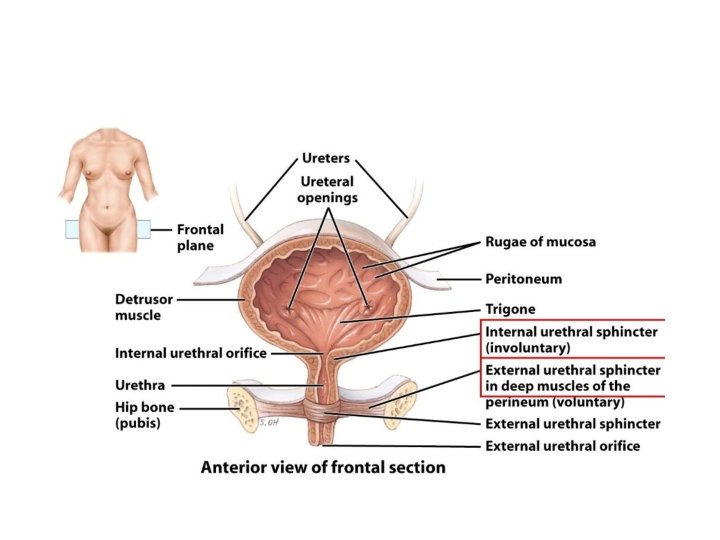
• two Sphincters: 1 - internal sphincter ( smooth muscle of bladder neck and proximal urethra) , physiologic sphincter and not under voluntary control, it is supplied by sympathetic
: the external sphincter composed of two parts the striated muscle")
2 -external sphincter (rhabdosphincter): the external sphincter composed of two parts the striated muscle of pelvic floor and striated muscle of distal urethra (intrinsic rhabdosphincter. - it is supplied by pudendal nerve , and is under voluntary control

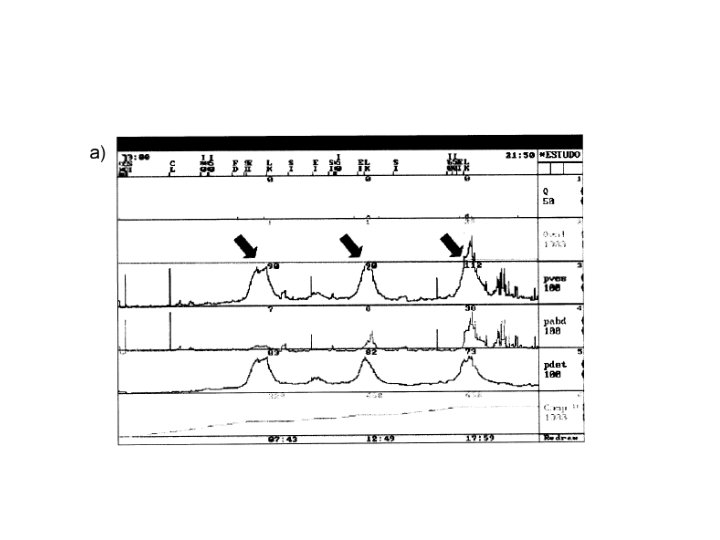
Incontinence - definition: - involuntary leakage of urine, results from failure of urine storage during filling phase - It is more common in female and increase with age - Types: 1 - urge incontinence: - involuntary leak of urine accompanied or immediately preceded by urgency it is due to bladder overactivity which - Can be due to detrusor over-activity or low compliance or both

DOA

• Detrusal overactivity may be neurogenic (due to neurological cause • Or non neurogenic like BOO, inflammatory condition , stress urinary incontinence , aging, polyuria , constipation

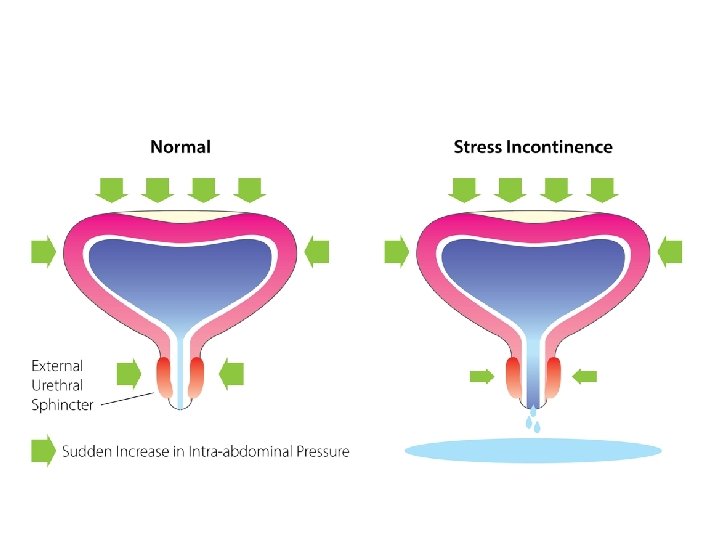
2 - stress incontinence: - involuntary leak of urine on effort or exertion or coughing or sneezing - Can be due to hypermobility of the bladder neck and urethra which rotate out of pelvis and so the abdominal pressure will be transmitted only to the bladder - Or due to intrinsic sphincter deficiency

• Cause of stress incontinence in female include multiple pregnancy and child birth • Obesity and smoking is promoting factors • Cause of stress incontinence in male include post prostate surgery or radiotherapy

3 - overflow incontinence: - Mainly in male with bladder outflow obstruction - Treatment is by relief of obstruction

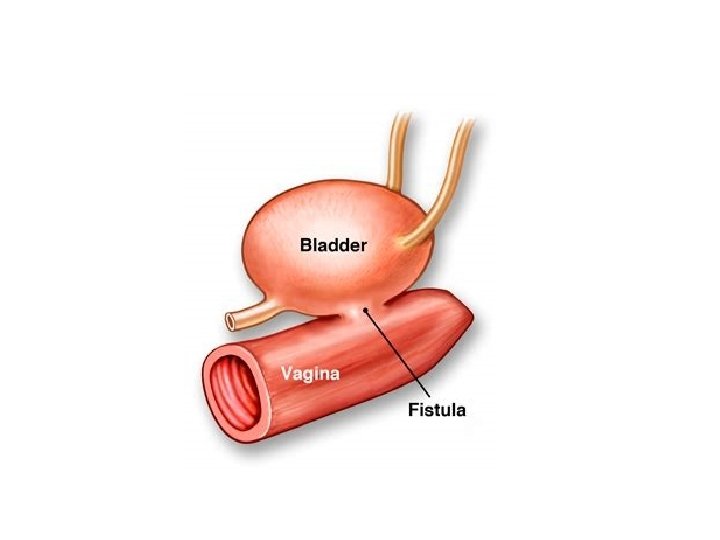
4 - continuous incontinence: - Leaking of urine continuously ( without aggravating factor and all the times) - Caused by fistula VVF ( extravesical incontinence)

5 - mixed incontinence: - More than one type in the same patient

assessment • History : the type of incontinence and if mixed if one component is more common or cause more bother • The leakage should be quantified( the nuber of pads, the frequency of leakage • The LUTS • Neurological symptom or bowl function • Female asked about prolapse symptom • Past medical and surgical history

• Complete physical examination is performed with emphasis on a neurologic assessment and the abdominal, pelvic and rectal examination • Examination of vaginal epithelium • Documentation of urethral leakage with cough

• Voiding diaries: which is measurement of frequency and voided volume, episode of incontinence, and fluid intake in 24 hours • It should be completed for at least 3 days • Urine analysis: UTI may cause urinary incontinence or the existing UI may worsens with UTI • PVR volume : the volume of urine that remains in bladder after voiding, measured by catheter or U/S • PVR volume should be assessed in PTN with voiding symptom or before surgery for stress incontinence

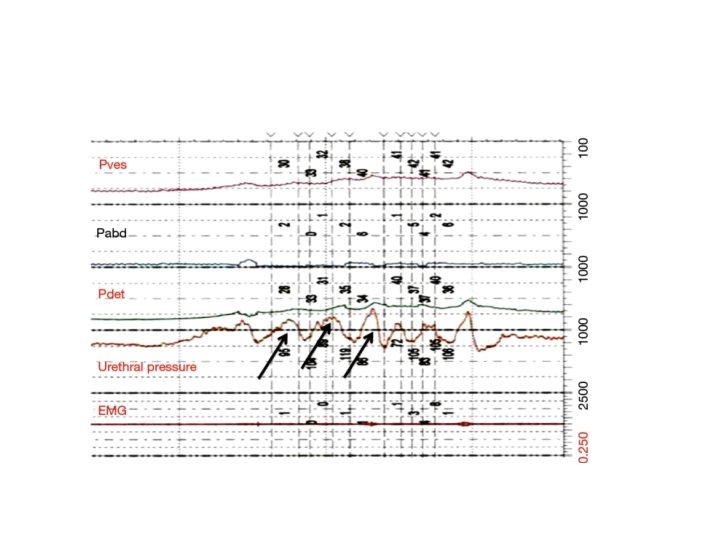
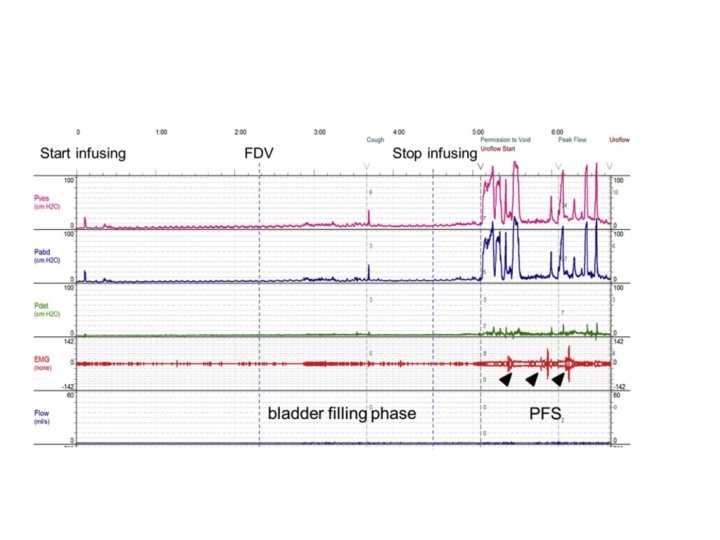
• Urodynamic study: test that asses how the bladder and urethra performing their jobs • is used to accurately diagnose the etiology of patient's incontinence • it is used in patient with urge predominant UI, and urinary incontinence with unclear type, history of previous surgery for SUI, symptom suggestive of voiding dysfunction

Treatment of UUI • Lifestyle change: decrease fluid intake, caffien reduction, lose weight if BMI more than 30 • Timed voiding: void every one to two hours during the day • Bladder training: e where the patient attempts to consciously delay voiding and to increase the interval between voids, last for minimum of 6 weeks

• Anticholinergic-antimuscarinics are the mainstay of medical therapy for urgency incontinence. • Side effect include urinary retention, dry mouth, constipation, blurred vision , confusion • Additional pharmaceutical options include beta 3 adrenergic receptor agonists
 has also been")
• Injection of the detrusor muscle with botulinum toxin (Botox) has also been successfully utilized for idiopathic, medication refractory OAB • Neuromodulation • Augmentation cystoplasty

Treatment of SUI • Pelvic floor muscle training : at least 8 contractions , 3 times per day for 3 monthes • Alpha-agonists such as pseudoephedrine may be used for the treatment of stress incontinence • Surgical therapy : which include retropubic suspension, sling procedure, artificial sphincter

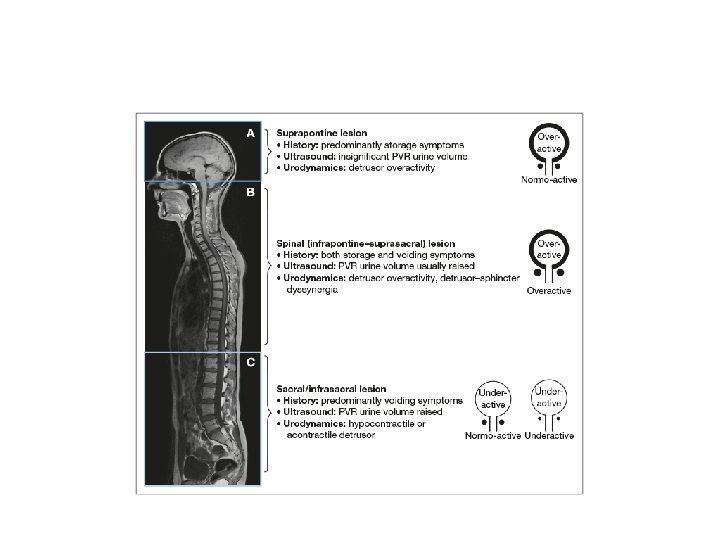
Voiding dysfunction according to spinal cord injury level 1 - suprapontine ( injury above brain stem) : - results in bladder overactivity with coordinated sphincter ( synergy) - Sensation usually preserved but it may be deficient - So patient usually presents with urinary incontinence

- Treatment by anticholinergic, botox injection or surgical.

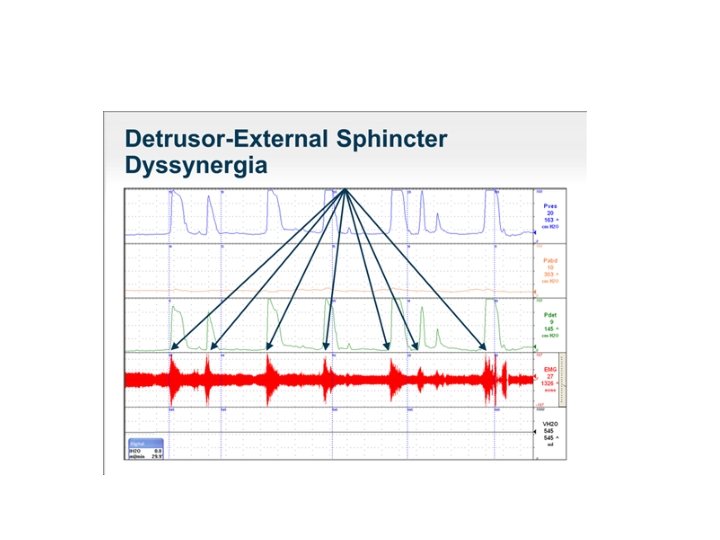
2 - spinal cord injury infrapontine but above spinal cord level T 6 : - Detrusal overactivity - Smooth and striated sphincter dyssynergy - Autonomic hyperreflexia (dysreflexia) - Impaired sensation - So patient presents with incontinence or retention

-Treatment: - to decrease outlet resistance by using baclofen and botox injection - Or use ISC to drain bladder regularly

Autonomic Dusreflexia - Usually in spinal cord injury between brainstem and spinal cord level T 6, so imbalanced reflex sympathetic discharge - Triggered by: - pelvic autonomic afferent activity ( as bladder or bowel distension , erection and ejaculation)

-Patient will develop hypertension, bradycardia , headache , sweating and flushing above spinal cord injury -treatment: -It is considered a medical emergency, If left untreated can cause seizures, retinal hemorrhage, myocardial infarction, cerebral hemorrhage, and, ultimately, death
 are mainstays in")
-Proper bladder and bowel care (ie, preventing fecal impaction, bladder distention) are mainstays in preventing episodes of autonomic dysreflexia.

-if patient becomes hypertensive , should place the patient in an upright position immediately, this takes advantage of an orthostatic response and helps with the pooling of blood in the lower extremities. -most commonly used agents for hypertension are nifedipine and nitrates

3 - spinal cord injury between spinal cord level T 6 and S 2 : -DOA -smooth sphincter synergy but striated sphincter dyssynergy -impaired sensation -patient presents with incontinence or obstructive symptoms and rarely retention

4 - injury below spinal cord level S 2: - detrusor areflexia with open smooth sphincter and striated sphincter retains a residual resting sphincter tone and is not under voluntary control. - Patient presents with retention

• Treatment • The primary aims and their prioritisation when treating neuro-urological disorders are: • 1. protection of the upper urinary tract; • 2. improvement of urinary continence; • 3. restoration of (parts of) the LUT function; • 4. improvement of the patient’s Qo. L. •
- Slides: 46