Bladder Cancer Dr Abdellatif Zayed Amzayed1919yahoo com Today

Bladder Cancer Dr. Abdellatif Zayed Amzayed_1919@yahoo. com

Today Objectives Pathology: ØPredisposing Factors ØPathologic Types ØStaging ØGrading Øspread Management: • Clinical features • Investigations • treatment

Predisposing factors: 1. 2. Industrial toxins Drugs: e. g. Cyclophosphamide

Predisposing factors: Ø Bilharzial infestation

Pathologic Types: 1. Transitional cell carcinoma: The commonest 2. Squmous cell carcinoma: In Egypt 50%. 3. Adinocarcinoma: bladder extrophy 4. Undifferentiated tumor: Highly aggressive.

Layers of the bladder wall

Stages Ø Ø Ø Tis: Carcinoma in situ Ta: Nan invasive papillary T 1: Invade subepithelial T 2: Invades muscle T 3: Invades perivesical t. T 4: Invades adjacent org.

Staging Tis: Carcinoma in situ Ta: Nan invas. papillary T 1: Invade subepithelial T 2: Invade muscle T 3: Invade perivesical t. T 4: Invade adjacent org.

Staging

Clinical Features: B Hematuria B Irritative symptoms B Necroturia

Investigations F Urine analysis and urine cytology F Ultrasound F IVU examination and CT F Cystoscopy and biopsy

Ultrasound Pictures

Cystogram DD n Bladder mass n Blood clots n Prostatic enlargement n Fungus ball

CT scan The primary imaging modality in evaluation of bladder tumor.
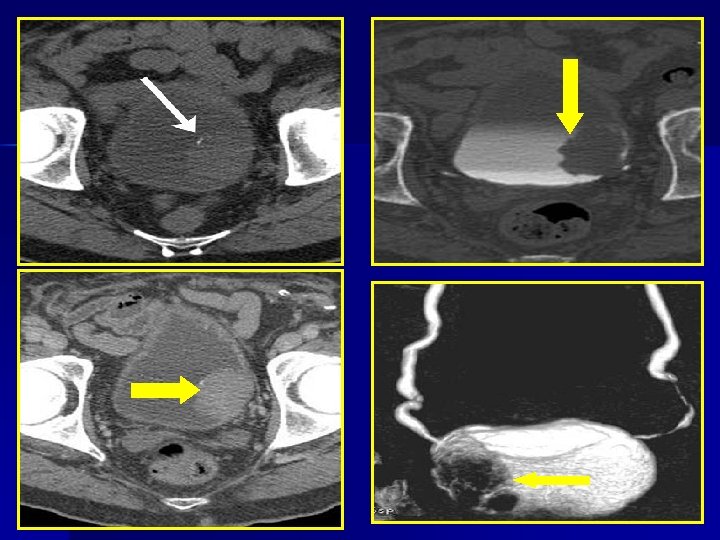

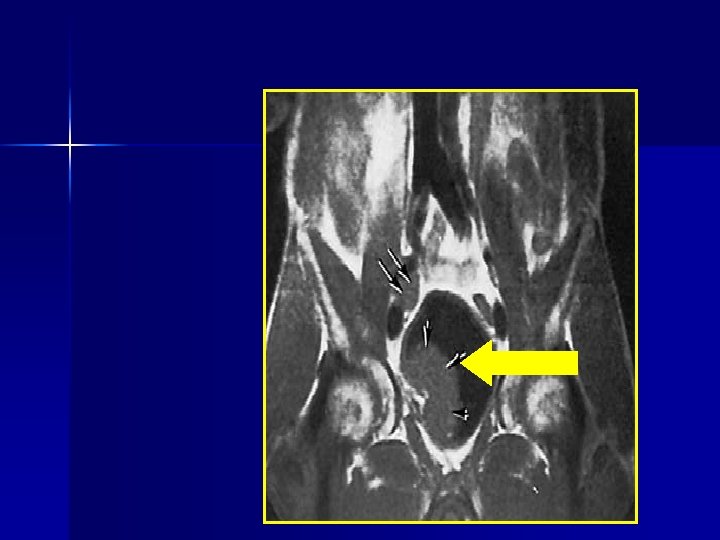
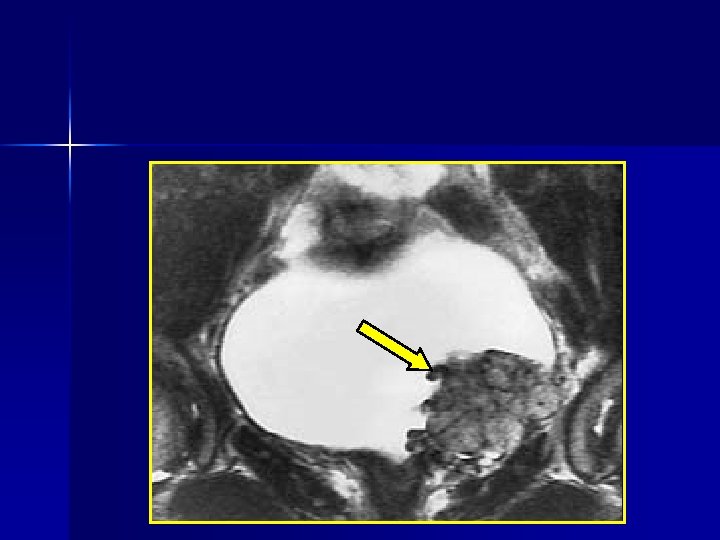
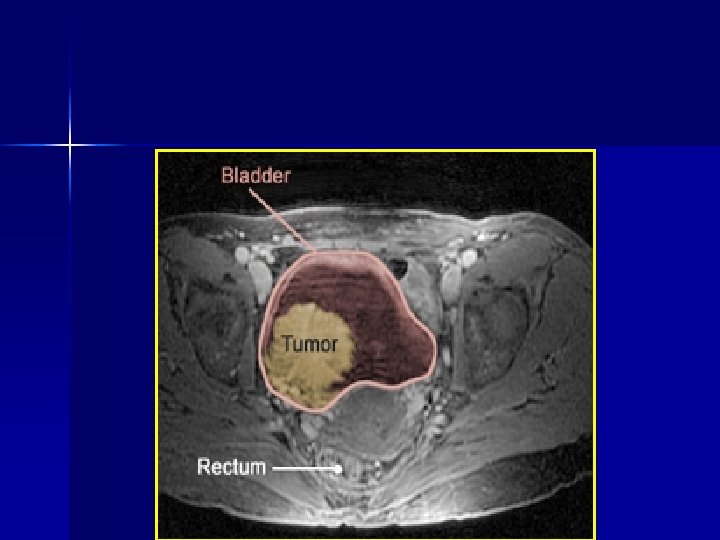
MRI n MRI has higher soft-tissue contrast than CT

Ta: Cystoscopic View of Papillary T

Tis: Carcinoma in situ

Treatment of superficial bladder CA Ø Complete TUR-T and immediate single intravesical instillation chemotherapy Ø Adjuvant intravesical immunotherapy: BCG Ø Radical cystectomy for certain cases.

Follow up is essential

Treatment of invasive tumor Operable: Radical cystectomy and urine diversion

Inoperable: palliative radiotherapy

Urine Diversion Continent: – Orthotopic bladder substitution – Continent reservoir for CIC – Ureterosigmoidostomy n Non Continent: - Uretero- cutaneous diversion - Ileal conduit n

Orthotopic Neobladder n depends on the intact urethra and sphincter to carry urine to the urethral meatus. n In case the urethra is involved by cancer, a continent reservoir with self catheterizable stoma.

Orthotopic Ileal neobladder

Ileal orthotopic neobladder Voiding cystourethrogram
")
3 Dimensions CT (Ilial neobladder)

Complications B Hyper continence B Stone B Metabolic acidosis

Ureterosigmoidostomy

Complications B Ascending infection B Hypercholorimic acidosis B Adenocarcinoma

Ilial Conduit
")
3 D. CT (Ilial Conduit)
 stomal : B Necrosis B Stenosis B Hernia (2) peristomal: B Fungal")
Complications (1) stomal : B Necrosis B Stenosis B Hernia (2) peristomal: B Fungal dermatitis B Contact dermatitis. B Trauma

Uretero Cutaneous Diversions Rarely done because of complications: B Urine leakage. B Infections. B Stenosis.

Regarding bladder tumors, all are true except: a. 90% are squamous carcinomas b. Painless haematuria is the commonest presentation c. Cigarette smoking is an important etiological factor d. Superficial tumors are often well controlled by TUR

Smoking increases the risk of : a. b. c. d. Oro-pharyngeal carcinoma Lung cancer Carcinoma of bladder All of the above

Pathology of schistosomiasis may include a. b. c. d. ”Swimmers itch” caused by skin penetration by cercariae Portal hypertension due to fibrosis Pre-disposition to bladder cancer All of the above

Female Anatomy

Male Anatomy

Thank you Amzayed_1919@yahoo. com 0101953318
- Slides: 43