BLADDER CANCER Bladder cancer hematurea It is the

BLADDER CANCER Bladder cancer

hematurea • It is the presence of blood in urine • Microscopic hematurea: more than 3 RBC /high power microscopy • Gross hematuria(macroscopic hematuria): when the patient can see the blood in urine • Hematuria in adult is symptom of malignancy until proven otherwise

• In evaluating hematuria several question should be asked • 1 -gross or microscopic • 2 -at what time during urination it happens • 3 -is hematuria associate with pain • 4 -presence of clot • 5 -intermittent or continuous

• The chance of identifying significant pathology increase with increase the degree of hematuria • Timing of hematuria during urination indicates the site of origin, initial hematuria from urethra, total hematuria from bladder and upper tract, terminal hematuria from bladder neck and prostatic urethra • Painful hematuria is the hematuria associated with flank pain , lower abdominal pain or dysuria

• Presence of clot usually indicate more significant degree of hematuria( more probability of identifying significant pathology), presence of vermiform clot usually indicate upper tract pathology • Hematuria due to malignancy is usually intermittent

• GH shoud be differntiated from pigmenturia such as bilirubin, myoglobin, beets, phenazopyridin, dehydration • Distinction is easy by urine analysis • GH also should be differentiated from vaginal bleeding

• Differential diagnosis of hematuria include: • Malignancy, stones, infection, BPH, medical kidney disease, trauma, bleeding tendency or PTN on anticoagulant

Pathology, grading , staging • Benign tumor of the bladder are uncommon • The magority of bladder tumors are malignant and epithelial in origin • 90% are transitional cell carcinoma (TCC) • 5% are squamous cell carcinoma • 2% are adenocarcinoma • Bladder cancer is the second most common urological malignancy

• Tumor grade: is the degree of differentiation, the extent to which the cancerous cell are similar in appearance and fuction to normal cells • 1973 WHO grading system: grade 1( well differentiated, grade 2(moderatley differentiated), grade 3( poorly differentiated) • 2004 WHO classification: PUNLMP, low grade, hige grade

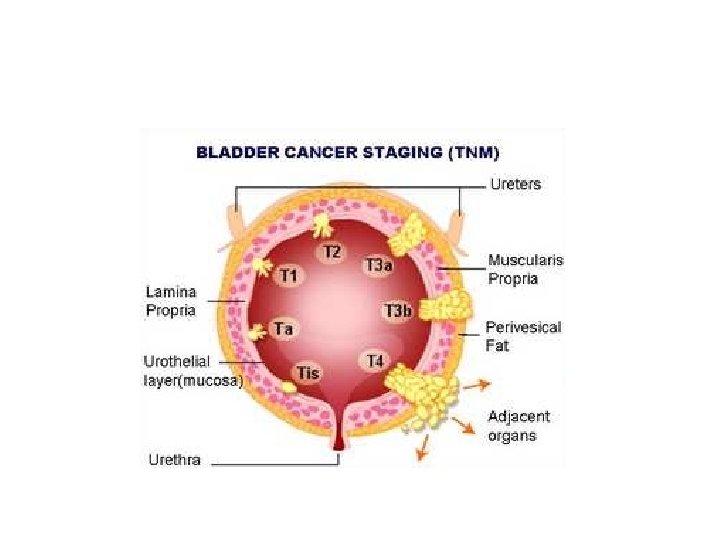
• Tumor stage : usually describes the size of tumour and how far it has spread from it, s origin • Staging of bladder cancer is by TNM classification

2 -staging: -

Bladder tumors 1 Gender: men are 3 to 4 times more likely to develop bladder cancer, because increased prevalence of smoking and exposure to environmental factor 2 Age: The incidence increase with increasing age , , most commonly diagnosed at eighth decade and rare before the age of 40 3 Race: Black people have lower incidence 4 Heredity: first degree relatives have two fold increase the risk of bladder cancer

Risk factors • Smoking: it is major cause of bladder cancer, recurrences , and mortality, smokers have 2 -6 higher risk of developing bladder cancers, the intensity and duration of smpking are linearly related to the increased risk, smoking stopping decrease the risk and mortality rate of bladder cancer
")
• Occupational exposure: like rubber or gas manufacture, painters, hairdressers • Drugs: phenacitin(acetaminophen) commonly used antipyretic and analgesic, cyclophosphamide( chemotherapy) • Pelvic radiotherapy • Chronic inflammation: longstanding catheter, bladder stone , schistosoma hematobium are associated with SCC of bladder

presentation • The commonest presentation is painless gross hematurea, . • Asymptomatic microscopic hematuria • Irritative voiding symptom especially in ptn with CIS.

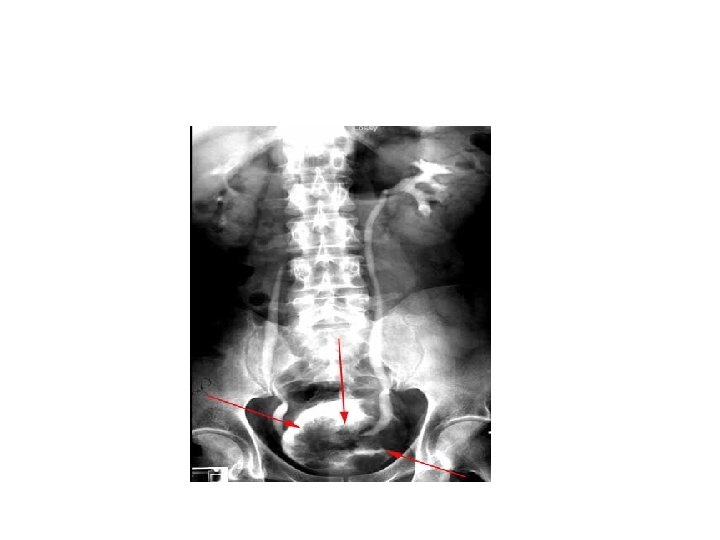
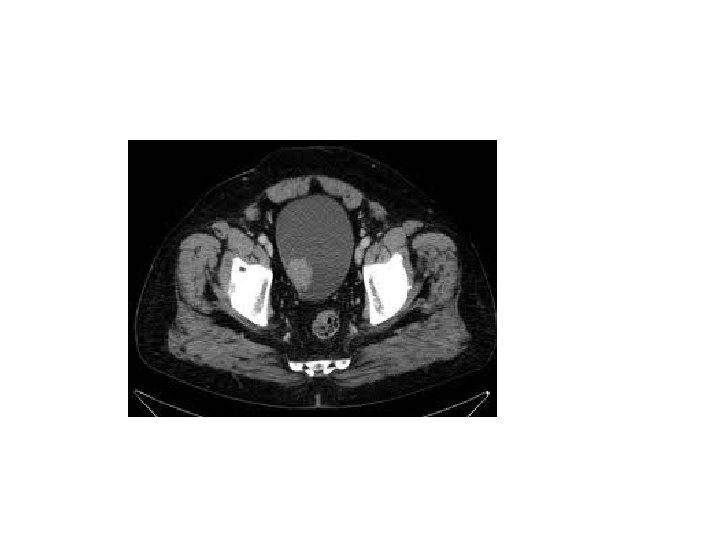
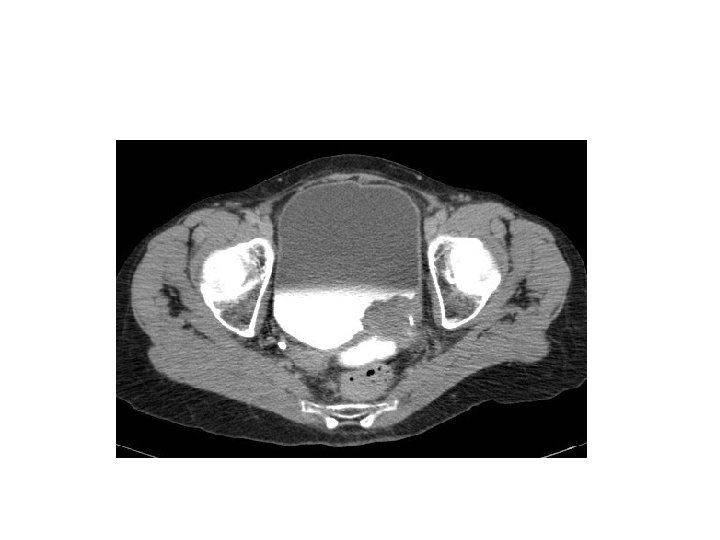
Hematuria work up 1 - flexible cystoscopy 2 - upper tract imaging ( CT urogram) 3 - others like urine cytology

Flexible cystoscopy

Rigid cystoscopy
")
• Difference between rigid and flexible cystoscopies ( advantages and disadvantages)

Bladder CA on cystoscopy

ultrasound

 which")
Traetement • TURBT then: 1 - if superficial ( Ta, T 1, CIS) which represent 70% of bladder CA do flexible cystoscopy for follow up+- intravesical treatement 2 - muscle invasive. . Radical cystectomy and conduit +-

• Patients with tumors at low risk of recurrence and progression should have a cystoscopy at 3 month. If negative, the following cystoscopy is advised at 9 month and consequently yearly for 5 yr.

• Patients with tumors at high risk of progression should have a cystoscopy at 3 month. If negative, the following cystoscopies should be repeated every 3 month for a period of 2 yr, every 4 month in the third year, every 6 month thereafter until 5 yr, and yearly thereafter. • A yearly exploration of the upper tract is recommended

Intravesical treatement 1 - Intravesical chemotherapy: like mitomycin , it is administered through folleys catheter and held for one hours , should not be given if there is ongoing hematurea or suspected bladder perforation, it may given as single dose within 24 hours of resection or 6 doses starting 2 weeks post resection 2 -intravesical BCG: attenuated strain of mycobacteria, induce immune response against the tumor, it reduce the recurrence and progression, should be used after two weeks of resection, less expensive and more effective but with more side effect
- Slides: 30