Birth by forceps Characteristics of the obstetric forceps

Birth by forceps Characteristics of the obstetric forceps

• l obstetric forceps are composed of two separate blades right and left • insertion around the fetal head within the maternal vagina • two shanks (shahs) of varying length and two handles. • Forceps are two type • *non- rotational * rotational.

• The blades have a cephalic curve to accommodate the form of the baby's head and are fenestrated (and not solid) to minimize the trauma to the baby's head during both placement and birth. • They also have a pelvic curve to reduce the risks of trauma to the maternal tissues during the birth process. • the blades are correctly positioned around the fetal skull • Will be noted to ‘lock with ease’. • Forceps that do not lock are most commonly incorrectly placed.

Classification of obstetric forceps -Forceps into two categories: * mid-cavity *and low-cavity. • Mid-cavity forceps are used when the leading part of the fetal head has reached below the level of the Ischial spines; • low-cavity forceps are used when the head has descended to the level of the pelvic floor. • High-cavity forceps (with the leading part of the fetal head above the level of the ischial spines) are now considered unsafe and a CS will be the preferred method of birth in nearly all cases.

Types of obstetric forceps • Wrigley's forceps • -used when the head is on the perineum or to assist the birth of the fetal head at caesarean section. • They have a short shank, fenestrated blades with both pelvic and cephalic curves, and an English lock


Neville–Barnes or Simpson's forceps • used for a low- or mid-cavity forceps birth when the sagifal suture is in the anteroposterior diameter of the cavity of the pelvis. • they have cephalic and pelvic curves to the fenestrated blades • the handles are longer and heavier than those of the Wrigley's.

Kielland's forceps • designed to deliver the fetal head at a station at, or above, the pelvic brim. • They are now more commonly used for the rotation and extraction of a baby whose head is in the deep transverse or occipitoposterior Malposition. • It allow for the safe rotation of the fetus),

Procedure • explain & Rationale • consent • urinary bladder catheterization, • FHR monitoring • position of the woman's legs • Consideration to the location of the birth( labor room , or theater ) • inhalational analgesia or a pudendal nerve block with perineal infiltration is unlikely to be sufficient for a forceps birth. • an epidural, if already in situ, may be topped up, or a spinal anaesthetic should be administered, is given to using Kielland's forceps.
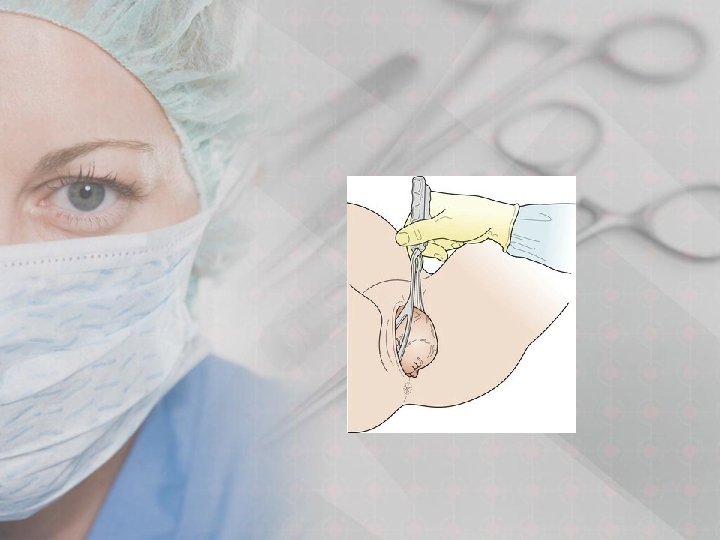
 and placed around the fetal head. •")
• will be inserted per vagina) and placed around the fetal head. • The left blade is inserted before the right blade, with the other hand protecting the vaginal wall from direct trauma. • The forceps blades come to lie parallel to the axis of the fetal head, and between the fetal head and the pelvic wall. • then articulates and locks the blades, checking their application before applying traction. • Traction should be applied in concert with uterine contractions and maternal expulsive efforts.




Complications of instrumental vaginal birth • forceps are less likely than the ventouse to fail to achieve a vaginal birth, likely to be associated with • third- or fourth-degree tears (with or without the concurrent use of an episiotomy) • vaginal trauma • use of general anesthesia • flatal, faecal and urinary continence

Maternal complications • Trauma or soft tissue damage – occurring to the cervix, vagina or perineum. • Dysuria or urinary retention, which may result from bruising or edema to the tissues around the urethra. • Perineal discomfort. • Hemorrhage (both from tissue trauma and also uterine atony – the risk of which is always increased following an assisted vaginal birth).

Neonatal complications • Marks on the baby's face and bruising (commonly caused by the pressure from the forceps blades and around the caput succedaneum/chignon from the ventouse , all of which resolve within 48– 72 hours after birth • Facial palsy, which may result from pressure from a blade compressing a facial nerve (a transient problem in most instances). • Prolonged traction during a birth with a ventouse will increase the likelihood of scalp abrasions, cephalohaematoma or sub-aponeurotic bleeding

Failure With the ventouse • Failure to select the correct cup type • inappropriate use of the silastic cup , especially in the presence of: • @ deflexion of the fetal head • @ excess caput • @‘dense’ epidural block • @ fetal macrosomia (true CPD). • @Failure of the equipment to provide adequate traction • @Incorrect cup placement – too anterior or lateral,

Failure With any instrument • Inadequate case assessment • high head • misdiagnosis of the position and attitude of the head. • along Traction • Poor maternal effort with inadequate use of syntocinon

Thank You. . !!
- Slides: 20