BIRTH ASPHYXIA Dr Jacob kuruvilla INTRODUCTION Hypoxicischemic encephalopathy

BIRTH ASPHYXIA Dr. Jacob kuruvilla

INTRODUCTION
 is an important cause of brain injury in the")
– – Hypoxic-ischemic encephalopathy (HIE) is an important cause of brain injury in the newborn and can result in long-term devastating consequences. Perinatal hypoxia is a vital cause of long-term neurologic complications varying from mild behavioural deficits to severe seizure, mental retardation, and/or cerebral palsy in the newborn.

● ● ● Understanding of hypoxic ischemic injury is handicapped by the lack of generally accepted definition. Asphyxia - Impairment of placental or pulmonary gas exchange resulting in hypoxemia, hypercapnia and a mixed respiratory and metabolic acidosis Hypoxia - condition in which the body or a region of the body is deprived of adequate oxygen supply. Ischaemia - restriction in blood supply to tissues, causing a shortage of oxygen and glucose needed for cellular metabolism (to keep tissue alive) Neonatal encephalopathy - is a clinical term used to describe an abnormal neurobehavioral state that consists of a decreased level of consciousness with abnormalities in neuromotor tone.

The essence of this is a simultaneous occurrence of hypoxia and ischemia and the term hypoxic ischemic insult is now preferred.

DEFINITION
 refers to the CNS dysfunction associated with perinatal asphyxia. It is")
Hypoxic ischemic encephalopathy(HIE) refers to the CNS dysfunction associated with perinatal asphyxia. It is an abnormal neurobehavioral state in which the predominant pathogenic mechanism is impaired cerebral blood flow that may result in neonatal death or CNS dysfunction.

Etiology of HIE • Maternal: – Cardiac arrest – Asphyxiation – Severe anaphylaxis – Status epilepticus – Hypovolemic shock • Uteroplacental: – Placental abruption – Cord prolapse – Uterine rupture – Hyperstimulation with oxytocic agents • Fetal: – Fetomaternal hemorrhage – Twin to twin transfusion – Severe isoimmune hemolytic disease – Cardiac arrhythmia

TIMING OF HIE 20% Antepartum 35% Antepartum/ Intrapartum 30% Intrapartum 10% Postpartum

INCIDENCE

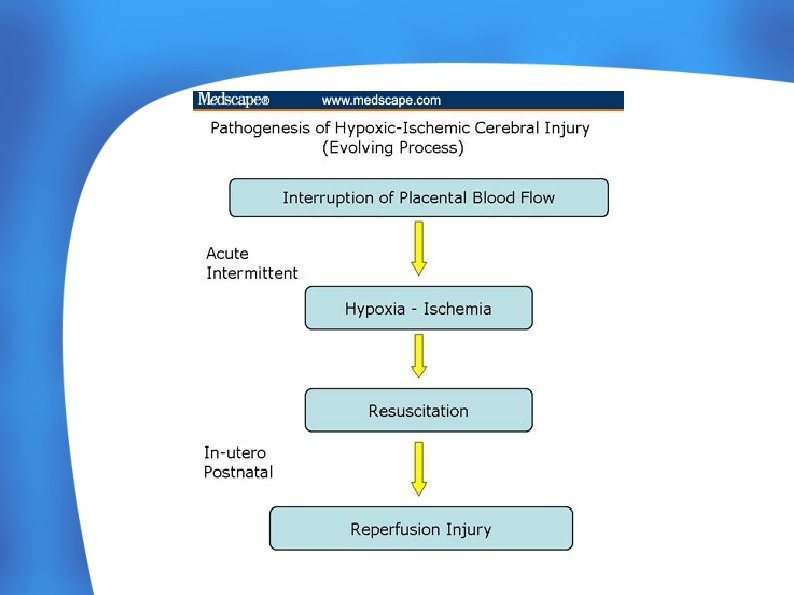
PATHOPHYSIOLOGY OF HIE

ASPHYXIA-PATHOPHYSIOLOGY

Intrapartum Asphyxia results in: – Diminished Oxygen Content in Blood – Increased Carbon dioxide – Acidosis – Decrease blood pressure ● Loss of Normal Cerebrovascular auto regulation resulting in pressure-passive Flow ● Results in decreased perfusion Of brain and hypoxic neuronal injury ● Following Resuscitation - Repurfusion Injury and IVH ●

MECHANISM OF INJURY

Mechanism of injury following hypoxia-ischemia Insults e. g. Asphyxia Impaired perfusion Opportunity for neuronal rescue Primary neuronal death Cytotoxic mechanisms Delayed neuronal Death /Reperfusion Injury

CLINICAL FEATURES & DIAGNOSIS : ANTEPARTUM -Fetal distress : if fetal distress detected it cannot be assumed that the insult has occurred during labor. A fetus that has sustained a hypoxic –ischemic insult before labor may not be able to mount the normal physiological coping responses during labor.

CLINICAL FEATURES & DIAGNOSIS : INTRAPARTUM Apgar scores : prolonged depression of Apgar is related to major neurological disability.

APGAR Score: Total Score = 10 score 7 -10 normal score 5 -6 mild birth asphyxia score 3 -4 mod. birth asphyxia score 0 -2 severe birth asphyxia

● The problems with using Apgar score as a marker of HIE are: ● Apgar score may be low because of causes other than birth asphyxia, e. g. prematurity, maternal sedation, neuromuscular disorder, etc. ● Apgar score has a poor correlation with the long term outcome. However, the extended Apgar score recorded 20 minutes after birth has much better specificity for the prediction of both early death and disability ● A low 1 or 5 -minute Apgar score alone does not correlate with the infant’s future outcome

CLINICAL FEATURES & DIAGNOSIS : INTRAPARTUM Acidosis : is associated with poor outcome in combination with abnormal fetal heart rate pattern, depressed apgar scores and encephalopathy

Sarnat Clinical Stages of Perinatal Hypoxic Ischemic Brain Injury

Sarnat Clinical Stages of Perinatal Hypoxic Ischemic Brain Injury
 Disturbances include increased nucleated RBCs, neutropenia or neutrophilia, thrombocytopenia, and coagulopathy.")
Hematologic (32 -54%) Disturbances include increased nucleated RBCs, neutropenia or neutrophilia, thrombocytopenia, and coagulopathy. Severely depressed respiratory and cardiac functions and signs of brainstem compression suggest a lifethreatening rupture of the vein of Galen (ie, great cerebral vein) with a hematoma in the posterior cranial fossa.

● Infants who survive severe hypoxic-ischemic encephalopathy ● ● The level of alertness improves by days 4 -5 of life. Hypotonia and feeding difficulties persist, requiring tube feeding for weeks to months.

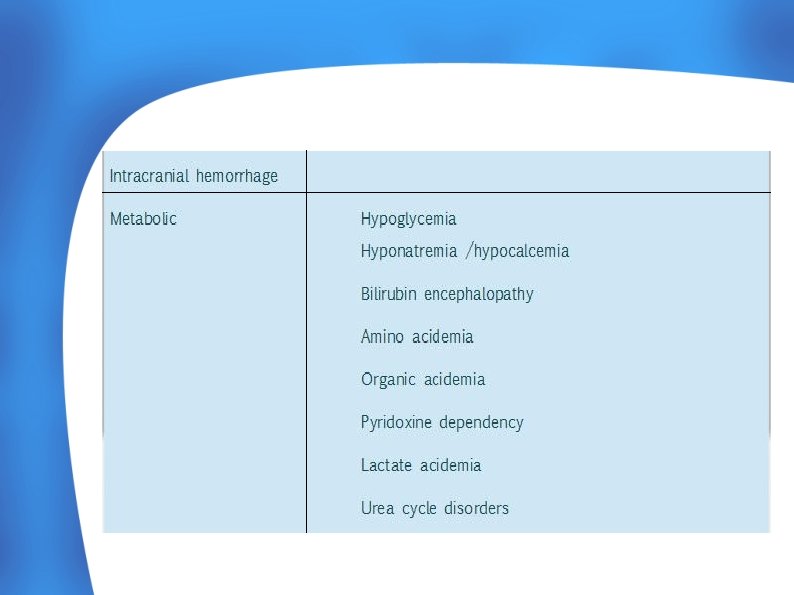
Exclusion of alternative causes of Neonatal Encephalopathy

INVESTIGATIONS

Study Serum electrolyte Markedly low serum sodium, potassium, and chloride levels in the presence of reduced urine flow and excessive weight gain may indicate acute tubular damage or (SIADH) secretion, particularly during the initial 2 -3 days of life. Renal function Serum creatinine levels, creatinine clearance, and BUN levels Cardiac & liver enzymes Assess the degree of hypoxic-ischemic injury to other organs Coagulation system Prothrombin time, partial thromboplastin time, and fibrinogen levels. ABG Assess acid-base status and to avoid hyperoxia and hypoxia as well as hypercapnia and hypocapnia. To correct acidosis Others Screen for infection (± lumbar puncture), Tests for congenital infection , Investigation for metabolic or genetic disorders, lactate, pyruvate

Imaging studies: - Cranial USG -Convenient, noninvasive, relatively low-cost and non – radiation screening examination of the hemodynamically unstable neonate at the bedside. -Doppler study and resistive index (RI) provide additional information on cerebral perfusion. -Sustained asphyxia & ICH or diffuse cerebral edema results in increased RI and is indicative of a poor outcome.

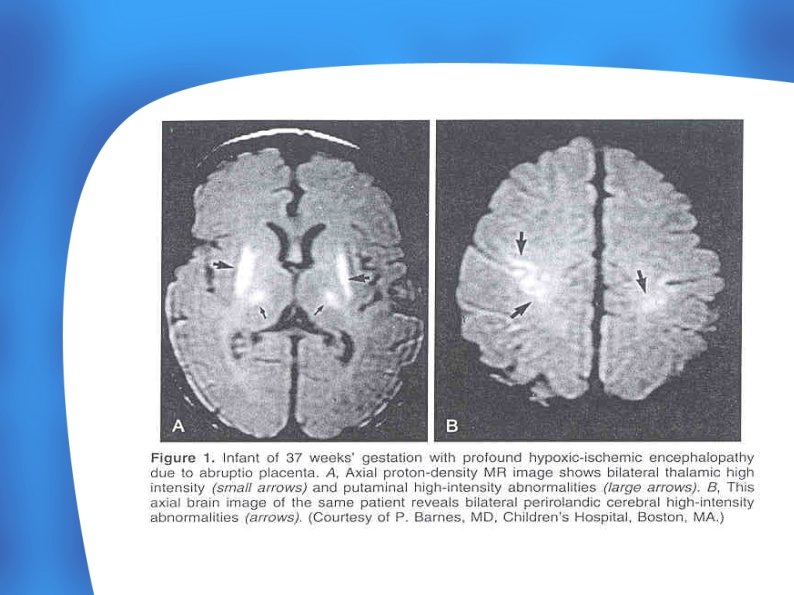
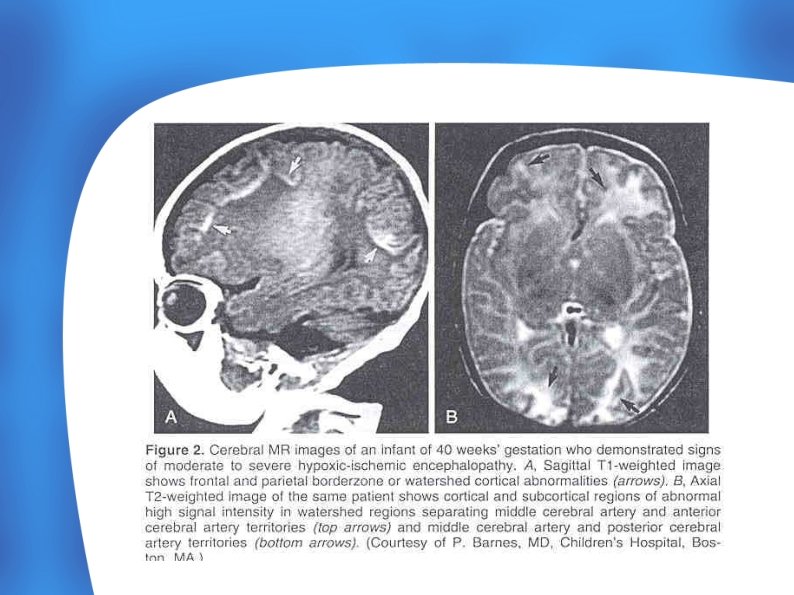
Cranial MRI - The most sensitive and specific imaging technique for examining infants with suspected hypoxic-ischemic brain injury. - Hypoxic-ischemic injury (deep grey matter, cortex)demonstrates characteristic T 1 hyperintensity and variable T 2 intensity. - Ischemic injury generally results in T 1 hypointensity &T 2 hyperintensity (white matter)due to ischemia-induced edema.

Standard EEG - Generalized depression of the background rhythm and voltage, with varying degrees of superimposed seizures, are early findings.

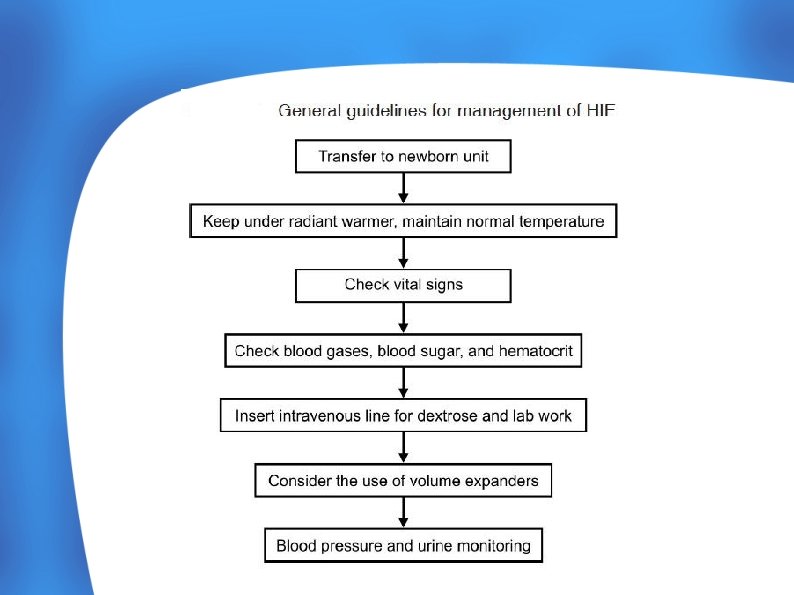
MANAGEMENT

Clinical management is primarily supportive and is dependent on the extent of organ compromise. High level evidence supports the use of therapeutic hypothermia for the treatment of moderate to severe cases of HIE; Each baby’s management should be individualised, with close monitoring of cardiorespiratory status and early identification and treatment of multi-organ system complications where appropriate
 Vitals parameters 2) Accurate record of the urine output 3)")
Monitoring : 1) Vitals parameters 2) Accurate record of the urine output 3) If required blood gases analysis can be done. 4) Periodic blood biochemistry such as: 5) Blood sugar charting (2 hourly x 2 , then 4 hrly on the 1 st day and 6 hrly thereafter. 6) Hematocrit – (6 to 8 hrly for the first 2 days , the once a day) 7) Serum sodium, potssium and calcium (once a day). 8) Assessment of the of sensorium, tone, seizures autonomic disturbances and reflexes should be done every 4 to 6 hours

MANAGEMENT-LABOUR ROOM Resuscitation Appropriate and timely resuscitation is required to prevent hypoxia, hypercarbia and acidosis. This may prevent or reduce the clinical severity of HIE. ● Cord blood gases should be measured if possible in every resuscitated newborn baby as the most objective way to assess the baby’s condition just before birth. ● Collect umbilical cord arterial blood gases from a clamped cord as soon as possible after delivery (preferably before 30 minutes, arterial p. H and base excess become unstable in a clamped cord at room temperature after 30 minutes) ● Blood samples taken for acid base status remain stable in a plastic syringe for up to 30 minutes before analysis ●

MANAGEMENT-NICU CARDIORESPIRATORY Monitor for hypoxia, acidosis and hypercarbia. Respiratory distress may have multiple causes including: – Acidosis – meconium aspiration sepsis – Persistent pulmonary hypertension of the newborn (PPHN) – Hyaline membrane disease (HMD) Babies with respiratory depression should be intubated and ventilated particularly if: – There is severe encephalopathy – There is severe acidosis – The baby is having frequent seizures – The baby requires large or frequent doses of anticonvulsant medication.

Assessment should include: • Assessment of peripheral perfusion • Establishment of whether hypotension is symptomatic of another problem including -Sepsis -Hypovolaemia or blood loss. -High mean airway pressure on mechanical ventilation The need for intravenous crystalloid boluses (10 m. L/kg of 0. 9% Sodium Chloride) if: – Perfusion is poor (capillary refill greater than 3 seconds) – Blood gas lactate is not improving – Mean blood pressure is less than 35 - 40 mm. Hg ●
 which may identify hypovolaemia, poor myocardial contractility and low")
The need for echocardiography (ECHO) which may identify hypovolaemia, poor myocardial contractility and low flow states and should be considered in ventilated babies after a significant hypoxic -ischaemic insult. ● If hypotension persists or low flow states are identified on ECHO consider inotropic therapy including: ● – Dopamine or Dobutamine – Inotropes should preferably be administered via an appropriately positioned catheter in a central vein (e. g. umbilical venous catheter positioned above the ductus venosus). – A dedicated intravenous line is preferred. Never give inotropes into an arterial line

INFECTION Perinatal infection may co-exist with HIE. All babies should have: ● A full blood count (FBC) ● Blood cultures Intravenous antibiotics (Penicillin (Benzylpenicillin, Ampicillin or Amoxicillin)) and Gentamicin) as soon as possible after birth. ●

Fluid, electrolyte and acid base Management Hypoglycaemia ●Perform an early blood glucose level and correct hypoglycaemia. Babies with Stage 2 to 3 HIE will require intravenous glucose administration ●Acidosis ● Perform early arterial blood gas and correct ● Respiratory acidosis (hypercarbia and acidosis) with appropriate ventilatory support ● It is possible to correct persistent severe metabolic acidosis in a baby who is appropriately ventilated with intravenous Sodium Bicarbonate given at a rate of no more than 0. 5 mmol/kg per minute. 19 ● Do not give Sodium Bicarbonate to a baby who is not effectively ventilating (either spontaneously or mechanically) as it causes hypercarbia and worsens respiratory acidosis. ● There is no convincing evidence that administration of Sodium Bicarbonate produces long term benefits in this situation.

VOLUME Many restrict maintenance fluids to 40 – 50 m. L/kg/day until a urine output equal to 1 m. L/kg/hr has been established. ● Fluid restriction is recommended to avoid fluid overload and cerebral oedema, however no RCTs address the use of fluid restriction following perinatal asphyxia. ● There is concern that fluid restriction may cause dehydration and hypotension decreasing cerebral perfusion and causing further brain damage. ● Monitor serum sodium trends to gauge whether more or less fluids are needed. ●

Administer intravenous 10% Glucose in the first 24 hours. Once renal function is stable, sodium and potassium additives can be commenced if required • If the baby has oliguria/anuria consider: ● o urinary catheterisation especially if there is a palpable bladder and/or baby is not voiding spontaneously o Dopamine (4 microgram/kg/minute or less) if not already receiving inotropic therapy o withholding second or subsequent dose of aminoglycoside (Gentamicin) antibiotics if prescribed. Be guided by serum aminoglycoside levels if considering further doses - Assess the fluid balance regularly and check urea, electrolytes and creatinine (there is a risk of fluid overload and hyperkalaemia)
 following a hypoxic-ischaemic insult can benefit certain babies")
TEMPERATURE MANAGEMENT • Therapeutic hypothermia (cooling) following a hypoxic-ischaemic insult can benefit certain babies and is now considered standard care • For cooling to provide benefit: • It must be commenced within 6 hours of birth before secondary reperfusion injury begins.

SEIZURE MANAGEMENT HIE is the most common cause of early onset neonatal seizures. Approximately 30% of babies with HIE have seizures which usually occur in the first 24 hours after birth and may be difficult to control. The early onset of seizures may predict a poorer neurodevelopmental outcome independent of the severity of hypoxi -ischaemic brain injury • Electrolyte abnormalities and multi system complications may coexist. Localised ischaemic events may result in focal clonic seizures. It is important to exclude other causes of seizures which include: o intracranial haemorrhage (approximately 15%) o neonatal stroke o intracranial infections o metabolic abnormalities o central nervous system malformations o drug withdrawal o hypoglycaemia

• 30 -90% of seizures are subclinical and up to 50% of clinical seizures may not be detected • 66% of electrographic seizures do not have overt clinical signs • Anticonvulsants may not treat electroencephalographic seizures even if effective for clinical seizure activity • Seizures should be treated to reduce the risk of additional injury, however little consensus exists regarding the optimal treatment protocol. 38 Ensure that ventilation and cardiovascular status are stable and monitored before giving anticonvulsant therapy • Anticonvulsant therapy should be given intravenously to achieve a rapid onset of action and predictable blood levels. Recommended anticonvulsant therapy includes: o Phenobarbitone (first line treatment) o Phenytoin o Midazolam o Clonazepam

GIT SYMPTOMS MANAGEMENT Do not feed during therapeutic hypothermia and only recommence feeds after rewarming. Commence feeding after assessment of the severity of asphyxia and associated system complications including: - Whether the baby is being cooled - Respiratory distress - Encephalopathy - Hypotension - Renal impairment Feed intolerance is common as gut circulation may have been compromised, this may increase the risk for necrotising enterocolitis: Breast milk is preferable Feeds should be introduced gradually

PHOTOTHERAPY Most often the babies will present with hyperbilirubinemia so Phototherapy will be required. Hyper-bilirubinemia due to: -Lack of feeding -Liver injury -Increased hemolysis -hypotension

- Supportive Care in Patients with Hypoxic-ischemic Encephalopathy - Most infants with severe hypoxic-ischemic encephalopathy need ventilatory support during first days of life. - The role of mechanical ventilation is to maintain the blood gases and acid-base status in the physiological ranges and prevent hypoxia, hyperoxia, hypercapnia, and hypocapnia. Important point in ventilator seting is to avoid hyperoxia (inc o 2 free radicals) and hypocapnia (dec. Cerebral perfusion) - Infants with hypoxic-ischemic encephalopathy are also at risk for pulmonary hypertension and should be monitored. Nitric oxide (NO) may be used according to published guidelines.

Cerebral Palsy & HIE ● ● ● There has been considerable debate regarding the contribution of HIE to the prevalence of Cerebral Palsy Incidence of cerebral palsy is largely unchanged despite increasing obstertric intervention and better obstetric care. It has been suggested that the brain have been significantly impaired by the events during pregnancy and birth asphyxia is just a final insult making a relatively small contribution to the burden of damage

- Intrapartum asphyxia may be first presentation of cerebral palsy if this prenatal insult impairs the ability of the fetus to cope with physiological stress of labor - It is postulated that If the asphyxia is severe enough to cause brain injury, it often causes multi organ failure leading to neonatal death.

PREDICTORS OF OUTCOME The presence of one or more of the following features has been found to be a predictor of poor neurodevelopmental outcome in the long term. 1. Failure to establish respiration by 5 minutes of life 2. Apgar score of 3 or less at 5 minutes 3. Onset of seizures with in 12 hours 4. Refractory seizures 5. Stage III HIE 6. Persistent oliguria ( <1 ml/kg/hr) for the first 36 hrs of life 7. Inability to establish oral feeds by 1 wk 8. Abnormal EEG & failure to normalize by D 7 9. Abnormal CT, MRI, MRS in neonatal period

REFERENCES ● Roberton’s textbook of Neonatology 4 th edition ● Avery Disease of Newborn ● Manual of newborn Care Cloherty et al seventh Edition ● NNF guidelines ● AIIMS WHO Neonatology protocols ● Care of newborn : Meharban Singh ● Queensland Maternity and Neonatal Clinical Guideline. Hypoxic ischaemic encephalopathy (2010)

- Slides: 58