BIOMATERIALS AND ARTIFICIAL ORGAN BM 1303 S Sudha

BIOMATERIALS AND ARTIFICIAL ORGAN BM 1303 S. Sudha Lecturer Dept of Biomedical Engg

UNIT I

INTRODUCTION TO BIOMATERIALS n n During the last two decades, significant advances have been made in thedevelopment of biocompatible and biodegradable materials for medicalapplications. In the biomedical field, the goal is to develop and characterize artificial materialsor, in other words, “spare parts” for use in the human body to MEASURE, RESTORE and IMPROVE physical functions and enhance survival and qualityof life.

What’s a biomaterial? n 1980 - Passive and inert point of view Any substance or drugs, of synthetic or natural origin, which can be used for any period alone or as part of a system and that increases or replaces any tissue, organ or function of the body n 1990 – Active point of view Non-living material used in a medical device and designed to interact with biological systems

Classification of biomaterials First generation: INERT Do not trigger any reaction in the host: neither rejected nor recognition “do not bring any good result” Second generation: BIOACTIVE Ensure a more stable performance in a long time or for the period you want Third generation: BIODEGRADABLE It can be chemically degraded or decomposed by natural effectors (weather, soil bacteria, plants, animals)

What is a biocompatible material? n n n Synthetic or natural material used in intimate contact with living tissue (it canbe implanted, partially implanted or totally external). Biocompatible materials are intended to interface with biological system to. EVALUATE, TREAT, AUGMENT or REPLACE any tissue, organ or function ofthe body. A biocompatible device must be fabricated from materials that will not elicit an adverse biological response

Mechanical Properties of Metals How do metals respond to external loads? Stress and Strain n Tension n Compression n Shear n Torsion Elastic deformation Plastic Deformation n Yield Strength n Tensile Strength n Ductility n Toughness n Hardness

Stress-Strain Behavior Elastic deformation n Reversible: when the stress n is removed, the material n returns to the dimension it n had before the loading. n Usually strains are small n (except for the case ofplastics). Plastic deformation n Irreversible: when the stress n is removed, the material n does not return to its n previous dimension.

Stress-Strain Behavior: Plastic deformation: stress and strain are not proportional the deformation is not reversible deformation occurs by breaking and rearrangement of atomic bonds (in crystalline materials primarily by motion of dislocations) n

Typical mechanical properties of metals The yield strength and tensile strength vary with prior thermal and mechanical treatment, impurity levels, etc. This variability is related to the behavior of dislocations in the material. But elastic moduli are relatively insensitive to these effects. The yield and tensile strengths and modulus of elasticity decrease with increasing temperature, ductility increases with temperature.

Mechanics of Materials n n n The point up to which the stress and strain are linearly related is called the proportional limit. The largest stress in the stress strain curve is called the ultimate stress. The stress at the point of rupture is called the fracture or rupture stress. The region of the stress-strain curve in which the material returns to the undeformed state when applied forces are removed is called the elastic region. The region in which the material deforms permanently is called the plastic region. The point demarcating the elastic from the plastic region is called the yield point. The stress at yield point is called the yield stress.

Mechanics of Materials n n n n The permanent strain when stresses are zero is called the plastic strain. The off-set yield stress is a stress that would produce a plastic strain corresponding to the specified off-set strain. A material that can undergo large plastic deformation before fracture is called a ductile material. A material that exhibits little or no plastic deformation at failure is called a brittle material. Hardness is the resistance to indentation. The raising of the yield point with increasing strain is called strain hardening. The sudden decrease in the area of cross-section after ultimate stress is called necking.

Viscoelasticity Definition: time-dependent material behavior where the stress response of that material depends on both the strain applied and the strain rate at which it was applied! Examples n biological materials n polymer plastics n metals at high temperatures

Elastic versus viscoelastic behaviors For a constant applied strain n An elastic material has a unique material response n A viscoelastic material has infinite material responses depending on the strain-rate
some energy")
Viscoelastic Hysteresis Viscoelastic solid n some energy is dissipated with dashpots (as heat)some energy is stored in springs. Area in the hysteresis loop is a function of loading rate n For viscoelastic material, energy is dissipated regardless of whether strains(or stresses) are small or large n Under repetitive loading, a viscoelastic material will heat up

Wound healing n n n All wounds heal following a a specific sequence of phases which may overlap The process of wound healing depends on the type of tissue which has been damaged and the nature of tissue disruption The phases are: n n n Inflammatory phase Proliferative phase Remodelling or maturation phase

The ways in which wounds heal Three basic classifications exist: Healing by primary intention Two opposed surfaces of a clean, incised wound (no significant degree of tissue loss) are held together. Healing takes place from the internal layers outwards n Healing by secondary Intention If there is significant tissue loss in the formation of the wound, healing will begin by the production of granulation tissue wound base and walls. n Delayed primary healing If there is high infection risk – patient is given antibiotics and closure is delayed for a few days e. g. bites n

Wound assessment Signs of infection Odour or exudate Lab tests: Tc. PO 2 Size, depth & location WOUND ASSESSMENT Wound bed: • necrosis Wound edge Surrounding skin: colour, moisture, • granulation

The healing process n n n n Day 0 – 5 The healing response starts at the moment of injury – the clotting cascade is initiated This is a protective tissue response to stem blood loss The inflammatory phase is characterised by heat, swelling, redness, pain and loss of function at the wound site Early (haemostasis) Late (phagocytosis) This phase is short lived in the absence of infection or contamination

Granulation n Day 3 – 14 Characterised by the formation of granulation tissue in the wound Granulation tissue consists of a combination of cellular elements including: n Fibroblasts, inflammatory cells, new capillaries embedded in a loose extra-cellular collagen matrix, fibronectin and hyularonic acid

Moist wound healing n n Basic concept is that the presence of exudate will provide an environment that stimulates healing Exudate contains: n n Lysosomal enzymes, WBC’s, Lymphokines, growth factors……. . There are clinical studies which have shown that wounds maintained in a moist environment have lower infection rates and heal more quickly

Factors affecting healing n n n Immune status Blood glucose levels (impaired white cell function) Hydration (slows metabolism) Nutrition Blood albumin levels (‘building blocks’ for repair, colloid osmotic pressure - oedema) n n n Oxygen and vascular supply Pain (causes vasoconstriction) Corticosteroids (depress immune function)

Host Reactions to Biomaterials n Effect of the Implant on the Host n Local n Blood material interactions n n n n Protein adsorption Coagulation Fibrinolysis Platelet adhesion, activation, release Complement activation Leukocyte adhesion, activation Hemolysis Toxicity

Modification of normal healing n Encapsulation n Foreign body reaction n Pannus formation n Infection n Tumorgenesis Systemic and remote n Embolization n Hypersensitivity n Elevation of implant elements in the blood n Lymphatic particle transport n n

Effect of the Host on the Implant n Physical – mechanical effects n n n Abrasive wear Fatigue Stress corrosion, cracking Corrosion Degeneration and dissolution Biological effects n n n Absorption of substances from tissues Enzymatic degradation Calcification

Temporal Variation of Inflammatory Response

n n Activated by injury to vascularized connective tissue Series of reactions Various cells Controlled by endogenous and autocoid mediators

UNIT II

Types of Metallic Implants n n n Stainless steel Cobalt Based Alloys Titanium Alloys

Stainless Steels • Fe 60 -65 wt%, Cr 17 -19 wt %, Ni 12 -14 wt% • Carbon content reduced to 0. 03 wt% for better The most common stainless steel: 316 Lresistance to in vivo corrosion. • Why reduce carbon: Reduce carbide (Cr 23 C 6) formation at grain boundary. Carbide impairs formation of surface oxide • Why add chromium: corrosion resistance by formation of surface oxide. • Why add nickel: improve strength by increasing face centered cubic phase (austenite)
 n No ferrite (body")
Stainless Steels Good stainless steel: n Austenitic (face centered cubic) n No ferrite (body centered cubic) n No carbide n No sulfide inclusions n Grain size less then 100 mm n Uniform grain size

Cobalt Based Alloys Common types for surgical applications: n – ASTM F 75 n – ASTM F 799 n – ASTM F 790 n – ASTM F 562

Cobalt Alloys: ASTM F 75 n n n Co-Cr-Mo Surface oxide; thus corrosion resistant Wax models from molds of implants Wax model coated with ceramic and wax melted away Alloy melted at 1400 °C and cast into ceramic molds.

Cobalt Alloys: ASTM F 75 Three caveats: n – Carbide formation ® corrosion. Solution: annealing at 1225 °C for one hour. n – Large grain size ® reduced mechanical strength n – Casting defects ® stress concentration, propensity to fatigue failure

Cobalt Alloys: ASTM F 799, ASTM F 90 Cobalt Alloys: ASTM F 799 n Modified form of F 75: hot forged after casting n Mechanical deformation induces a shear induced transformation of FCC structure to HCP. n Fatigue, yield and ultimate properties are twice of F 75. Cobalt Alloys ASTM F 90 : • W and Ni are added to improve machinability and fabrication • Mechanical properties similar to F 75 • Mechanical properties double F 75 if cold worked

Titanium Based Alloys n n n Lighter Good mechanical properties Good corrosion resistance due to Ti. O 2 solid oxide layer Ti-6% wt Al-4% wt V (ASTM F 136) is widely used Contains impurities such as N, O, Fe, H, C Impurities increase strength reduce ductility

Titanium Alloys: ASTM F 136 n n n HCP structure transforms to BCP for temperatures greater than 882 °C. Addition of Al stabilizes HCP phase by increasing transformation temperature V has the inverse effect.

ceramic Any of various hard, brittle, heat-resistant and corrosionresistant materials made by shaping and then firing a nonmetallic mineral, such as clay, at a high temperature n Clinical success requires: Achievement of a stable interface with connective tissue Functional match of the mechanical behavior of the implant with the tissue to be replaced n Critical Issues: Integrity of bioceramic Interaction with the tissue n
 n n n Chemically similar to mineral component of bones It will")
Hydroxyapatites (HA) n n n Chemically similar to mineral component of bones It will support bone ingrowth and osseointegration when used in orthopaedic, dental and maxillofacial applications Chemical formula: Ca 5(PO 4)3 OH Hexagonal Bravais lattice The chemical nature of hydroxyapatite lends itself to substitution; common substitutions involve carbonate, fluoride and chloride substitutions for hydroxyl groups

Uses for HA Facial augmentation with hydroxyapatite has been used for the following corrections: Cheek, Chin, Jaw, Nose, Browbone. n Skeletal repair biomaterials n Ocular prosthesis n Hydroxyapatite from coral n The eye muscles can be attacheddirectly to this implant, allowing it to move within the orbit-just like the natural eye. n

Calcium Phosphate Bioceramics n n n There are several calcium phosphate ceramics that are consideredbiocompatible; most are resorbable and will dissolve when exposed tophysiological environments. Hydroxyapatite is thermodynamically stable at physiological p. H values; actively takes part in bone bonding, forming strong chemical bonds with surrounding bone Mechanical properties unsuitable for load-bearing applications such as orthopaedics Used as a coating on materials such as titanium and titanium alloys, where it can contribute its 'bioactive' properties, while the metallic component bears the load Coatings applied by plasma spraying

UNIT III

Polymeric Biomaterials What is a polymer? Long chain molecules that consist of a number of repeating units (mers) Fabricated from monomers which change somehow in polymerization Loss of H 20, HCl or other molecule n Polymer properties are more complex than for simpler materials Types of polymers Biological polymers n DNA, cellulose, starch, proteins, rubber, etc n Often reconstituted to form usable polymer n Mainly collected from animals Synthetic polymers n Fabricated from petroleum products (generally) n May be also a modified biological polymer n Most plastics and similar materials n

Classification Polymers Thermoplastics examples Thermosets Elastomers or Rubbers examples
 • Thermoplastic polymers: – Long chains with very limited or")
Classes of Polymers (I) • Thermoplastic polymers: – Long chains with very limited or no cross-linking – They behave in a plastic, ductile manner (above Tg) – Melt when heated and are thus easily remolded and recycled • Thermoset polymers: – Highly cross-linked, 3 D network structures – Generally brittle (at most temperatures) – Decompose when heated and can’t easily be reshaped or recycled
 n Elastomers and rubbers n n elastomer Large amounts of")
Classes of Polymers (II) n Elastomers and rubbers n n elastomer Large amounts of elastic deformation Some (light) cross-linking Typically, about 1 in 100 molecules are crosslinked on average n Average number of cross-links around 1 in 30 thermoset yields a more rigid and brittle material (closer to a thermoset) n n Crosslinks allows material to return to original shape without plastic deformation
 n Degree of polymerization, P=")
Definitions Oligomer- molecules with n<10 (less than ten monomers) n Degree of polymerization, P= number of monomer residues per chain n Functionality: number of bonding sites per monomer. A monomer must possess at least two bonding sites n Homopolymer A-A-A-A-A n Copolymer Random : A-B-A-A-A-B-B-B-A-B-B Alternating : A-B-A-B-A-B Block : A-A-A-B-B-B Graft A’s with B’s on branches n Linear polymer- no branches n Branched polymer - multiple branches n Crosslinked polymer- links between branches n

Polymer Basics n n Polymerization process: Initiation: I → 2 R • (the active center which acts as a chain carrier is created) Propagation: RM 1 • + M → RM 2 • (growth of macromolecular chain) Termination: kinetic chain is brought to halt

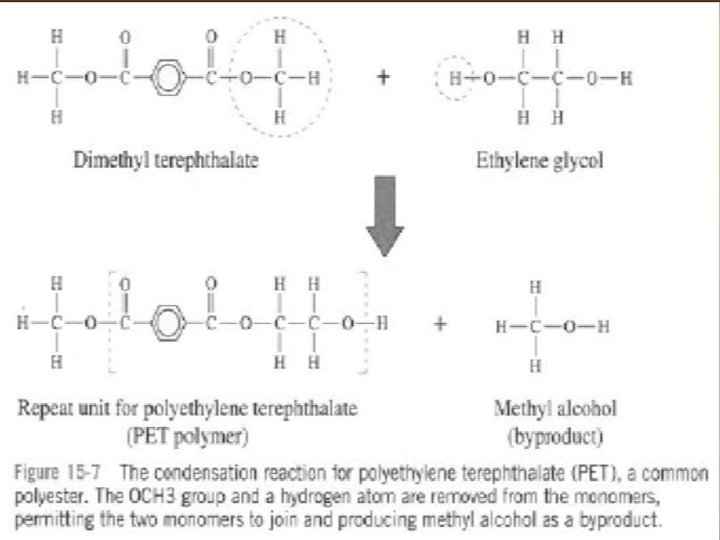
n n Synthesis Reactions: Addition polymerization Condensation polymerization Source: Askeland & Phule p 677
 PP (Polypropylene) n n Used in high density form astubing for drains")
PE (Polyethylene) PP (Polypropylene) n n Used in high density form astubing for drains and catheters Ultra high molecular weight form used as acetabul component in artificial hips and other prosthetic joints Has good toughness and wear resistance Resistant to lipid absorption n n High rigidity Good chemical resistance Good tensile strength Excellent stress cracking resistance Used for sutures and hernia repair
 PVC(Polyvinylchloride) n n n Aka Teflon Very hydrophobic Good lubricity Low wear")
PTFE (Polytetrafluoroethylene) PVC(Polyvinylchloride) n n n Aka Teflon Very hydrophobic Good lubricity Low wear resistance Used for catheters and vascular grafts (Gore. Tex) n n n Made flexible and soft bythe addition of plasticizers Not suitable for long term use because plasticizers can be extracted by thebody Used as tubing for blood transfusions, feeding anddialysis, and blood storagebags

Elastomers - Entropy If you stretch it far enough the chains will line up straight enough to crystallize

Elastomer vs. Thermoplastic Elastomers • Some amorphous polymer exhibit elastomeric behavior, yet have no chemical crosslinks – Usually block copolymers possessing both rubbery regions and stiff regions in the chain – Physical interactions between stiff chain regions act a Styrene butadiene styrene (SBS) physical “crosslinks” – Rubbery regions allow large deformations – Thermoplastic in nature; can be melted since there are no chemical crosslinks

Thermosets n Disadvantage n n Advantages in engineering design applications 1. 2. 3. 4. n Thermosets are difficult to re-form High thermal stability and insulating properties High rigidity and dimensional stability Resistance to creep and deformation under load Light-weight Crosslinking of thermosets n n n 10 -50% of the ‘mers’ in a chain are crosslinked Heat treatment, vulcanization processes link existing chains Two part chemistries (resin and curing agent) are mixed and react at room temp or elevated temperatures – multi -functional end groups

Polymers as Biomaterials n Hydrogels n n n Piezoelectric materials n n swellable materials, usually acrylic copolymers, e. g. poly(2 hydroxyethyl methacrylate): PHEMA More in lecture 10 materials that generate transient electrical charges on their surfaces upon mechanical deformation, e. g. polyvinylidene fluoride, collagen Resorbable materials n n Resorbed with time, e. g. polyglycolic and polylactic acid More in lecture 11

Fluorinated Polymers n PTFE n n n Fluorocarbons n n n Plain or expanded (Gore-Tex) Vascular grafts, sutures, middle ear prostheses High affinity for oxygen Blood substitutes Vinylidene Fluoride (PVDF) n n Piezoelectric Actuators, nerve guidance PTFE unsuccessful in joint replacements

Polymethyl methacrylate n n n PMMA A hydrophobic linear chain polymer that is transparent, amorphous and glassy at room temperature (also known as plexiglass or lucite) Good light transmittance, toughness, and stability A good material for intraocular lenses and hard contact lenses Also used as a bone cement
 n n High molecular weight form")
Polyethylene n n PE High density form (HDPE) n n High molecular weight form (UHMWPE) n n Used for tubing in catheters and drains Contact surface in artificial hips, knees Good toughness, resistance to fat and oils, and low cost

Polyethylene Glycol n n n PEG Short chain neutral hydrophilic polymer Shown to repel cells due to surface energy n n n Used for coatings – non-thrombogenic Wound healing: polymerization on the wound Microencapsulation and drug delivery

Biological Polymers n Many cellular and extracellular materials are polymers n Polysaccharides (made from monosaccharides) n n n Proteins (made from amino acids) n n Collagen Actin Fibrin Nucleic Acids (made from nucleotides) n n n Cellulose Alginate DNA RNA More in lecture 12
 No carbon backbone –")
Silicones n Silicone polymers n n e. g. Polydimethylsinoxane (PDMS) No carbon backbone – silicone and oxygen instead Elastomers (with crosslinks) Silicones as biomaterials n n Very low Tg Excellent flexibility and stability Used in catheters, pacemaker leads, vascular grafts, and breast and facial implants High oxygen permeability - membrane oxygenators

Common clinical applications and types of polymers used in medicine

application Polymers In Specific Applications properties and design requirements polymers used dental • stability and corrosion resistance, plasticity • strength and fatigue resistance, coating activity • good adhesion/integration with tissue • low allergenicity PMMA-based resins for fillings/prosthesis polyamides poly(Zn acrylates) ophthalmic • gel or film forming ability, hydrophilicity • oxygen permeability polyacrylamide gels PHEMA and copolymers orthopedic • cardiovascular • strength and resistance to mechanical PE, PMMA restraints and fatigue PL, PG, PLG • good integration with bones and muscles fatigue resistance, lubricity, sterilizability silicones, Teflon, 65 poly(urethanes),

UNIT IV

Soft Tissue Implants n Attempts have been made to replace or augment most of the soft tissues in the body n n n Most soft tissue implants are constructed from synthetic polymers n n n Connective tissues: skin, ligament, tendon, cartilage Vascular tissue: blood vessels, heart valves Organs: heart, pancreas, kidney Other: eye, ear, breast Possible to choose and control the physical and mechanical properties Flexibility in manufacturing "Soft tissue implants" can also be designed for soft tissue repair

Sutures Used to repair incisions and lacerations Important characteristics for sutures: : n Tensile strength n Flexibility n Non-irritating

Tissue Adhesives n Used for repair of fragile, non-suturable tissues n n Examples: Liver, kidney, lung The bond strength for adhesive closed tissues is not as strong after 14 days as for suture closed tissues

Percutaneous Implants n n Refers to implants that cross the skin barrier n In contact with both the outside environment and the biological environment Used for connection of the vascular system to external "organs" n Dialysis n Artifical heart n Cardiac bypass Also used for long term delivery of medication or nutrition (IV) Main Problems: n Attachment of skin (dermis) to implant difficult to maintain through ingrowth due to rapid turnover of cells n Implant can be extruded or invaginated due to growth of skin around the implant n Openings can also allow for the entrance of bacteria, which may lead to infection

Artifical Skin n Is actually a percutaneous implant -- contacts both external and biological environments No current materials available for permanent skin replacement Design ideas: n n Graft should be flexible enough to conform to wound bed and move with body Should not be so fluid-permeable as to allow the underlying tissue to become dehydrated but should not retain so much moisture that edema (fluid accumulation) develops under the graft

Artificial Skin - Possibilities n Polymeric or collagen-based membrane n n n Fabrics and sponges designed to promote tissue ingrowth n n n Some are too brittle and toxic for use in burn victims Flexibility, moisture flux rate, and porosity can be controlled Have not been successful Immersion of patients in fluid bath or silicone fluid to prevent early fluid loss, minimize breakdown of remaining skin, and reduce pain Culturing cells in vitro and using these to create a living skin graft n Does not require removal of significant portions of skin

Soft Tissue Augmentation n n Generally used for reconstructive or cosmetic enhancement Functions include one or more of the following n n Space filler Mechanical support Fluid carrier or storer Common applications for soft tissue augmentation are: n n Maxillofacial implants Eye and ear implants Fluid transfer implants Breast implants

Maxillofacial implants n n n n Designed to replace or enhance hard or soft tissue in the jaw and face Intraoral prosthetics (implanted) are used to reconstruct areas that are missing or defective due to surgical intervention, trauma, or congenital condition Must meet all biocompatibility requirements Metals such as tantalum, titanium, and Co-Cr alloys can be used to replace bony defects Polymers are generally used for soft tissue augmentation n Gums, chin, cheeks, lips, etc. Injectable silicone had been examined for use in correcting facial deformities; however, it has been found to cause severe tissue reactions in some patients and can migrate Extraoral prosthetics (external attachment) should: n Match the patients skin in color and texture n Be chemically and mechanically stable n Not creep, change colors, or irritate skin n Be easily fabricated

Fluid Transfer Implants n n May be designed as permanent implants to treat chronic problems Hydrocephalus n n n Ear Infections n n n Build up of cerebrospinal fluid in the brain Can result in brain damage if pressure becomes too high Treated by draining the fluid to the vascular system or abdominal cavity Uses a permanent shunt from the ventricles of the brain, under the skin, to the receiving tissue Tubing is made of silicone rubber made radiopaque to allow for observation with x-rays "Tubes" in the ears are drainage tubes designed to remove fluid from the middle ear Constructed from teflon or other inert materials Not permanent implants (removed after several years)

Orthopaedic Soft Tissue n n Replacement of cartilage, ligaments, and tendons Difficult to obtain fixation with bone n n In many cases autographs are used - may be patellar tendon for ACL reconstruction Allographs - cryo-preserved, fresh-frozen, or freeze dried specimens taken from cadavers n n n Screws or pins involve stress concentrations and the possibility of corrosion Strength of anchorage depends on thickness of cortical bone at attachment site Often attached to treated bony insertion sites which can be used as bone grafts (See Figure 6) Preservation and cold sterilization procedures may adversely affect properties of implants Available from tissue banks
 n n Artificial materials used")
Artificial Orthopaedic Soft Tissues n Ligament Augmentation Devices (LAD's) n n Artificial materials used to take some of the stress normally applied to a ligament while healing occurs May or may not be resorbable n n Contradictory results exist in the literature as to the effectiveness of LAD's Ligament scaffolds n n Gore-Tex: non-resorbable PDS: resorbable plastic Made of polyester or other polymers Used to induce tissue ingrowth May be implanted alone or with a section of tissue (fat pat, fascia lata, piece of tendon) to increase rate of ingrowth Region of fixation for artifical ligaments or reconstructions with LAD's for the ACL deviates from normal more than for reconstructions with patellar tendon alone n Fibrous tissue instead of normal transition from ligament to bone

Total Hip Replacement n n n A prosthetic hip that is implanted in a similar fashion as is done in people. It replaces the painful arthritic joint. The modular prosthetic hip replacement system used today has three components – the femoral stem, the femoral head, and the acetabulum. Each component has multiple sizes which allow for a custom fit. The components are made of cobalt chrome stainless steel and ultra high molecular weight polyethylene. Cementless and cemented prosthesis systems are available.

Common Causes of Hip Pain and Loss of Hip Mobility Osteoarthritis n Usually occurs after age 50 and often in an individual with a family history of arthritis. In this form of the disease, the articular cartilage cushioning the bones of the hip wears away. The bones then rub against each other, causing hip pain and stiffness.

Operation Removing the Femoral Head n n Once the hip joint is entered, the femoral head is dislocated from the acetabulum. Then the femoral head is removed by cutting through the femoral neck with a power saw.

Reaming the Acetabulum n n After the femoral head is removed, the cartilage is removed from the acetabulum using a power drill and a special reamer. The reamer forms the bone in a hemispherical shape to exactly fit the metal shell of the acetabular component.

Inserting the Acetabular Component n n A trial component, which is an exact duplicate of your hip prosthesis, is used to ensure that the joint will be the right size and fit for the client. Once the right size and shape is determined for the acetabulum, the acetabular component is inserted into place.

Preparing the Femoral Canal n n To begin replacing the femoral head, special rasps are used to shape and scrape out femur to the exact shape of the metal stem of the femoral component. Once again, a trial component is used to ensure the correct size and shape. The surgeon will also test the movement of the hip joint.

Inserting Femoral Stem n Once the size and shape of the canal exactly fit the femoral component, the stem is inserted into the femoral canal.

Attaching the Femoral Head n The metal ball that replaces the femoral head is attached to the femoral stem.

The Completed Hip Replacement • • Client now has a new weight bearing surface to replace the affected hip. Before the incision is closed, an x-ray is made to ensure new prosthesis is in the correct position.

Treatment by Kinesiologist n n n -Early Postoperative Exercises. Regular exercises to restore your normal hip motion and strength and a gradual return to everyday activties. Exercise 20 to 30 minutes a day divided into 3 sections. Increase circulation to the legs and feet to prevent blood clots Strengthen muscles Improve hip movement

UNIT V

Artificial heart valve n An artificial heart valve is a device implanted in the heart of a patient with heart valvular disease. When one of the four heart valves malfunctions, the medical choice may be to replace the natural valve with an artificial valve. This requires open-heart surgery.

Types of heart valve prostheses n n There are two main types of artificial heart valves: the mechanical and the biological valves. Mechanical heart valves n Percutaneous implantation n Sternotomy/Thoracotomy implantation n n Stent framed Not framed Ball and cage Tilting disk Bi-leaflet Tri-leaflet Biological heart valves n n Allograft/isograft Xenograft

Types of mechanical heart valves

Design challenges of heart valve prostheses n n A replaceable model of Cardiac Biological Valve Prosthesis. Thrombogenesis / haemocompatibility n Mechanisms: n n n n n Forward and backward flow shear Static leakage shear Presence of foreign material (i. e. intrinsic coagulation cascade) Cellular maceration Valve-tissue interaction Wear Blockage Getting stuck Dynamic responsiveness n n n Failure safety Valve orifice to anatomical orifice ratio Trans-valvular pressure gradient Minimal leakages Replaceable Models of Biological Valves

Artificial limb n An artificial limb is a type of prosthesis that replaces a missing extremity, such as arms or legs. The type of artificial limb used is determined largely by the extent of an amputation or loss and location of the missing extremity. Artificial limbs may be needed for a variety of reasons, including disease, accidents, and congenital defects.

Lower Limb Prosthesis n n n Components of the Prosthesis Socket- Forms the connection between the residual limb and the prosthesis. Sleeve- Provides suction suspension for prosthesis. Shank (pylon)- Transfers weight from socket to the foot-ankle. Foot-ankle- Absorbs shock and impact and provides stability.

Dental implant n A dental implant is an artificial tooth root replacement and is used in prosthetic dentistry to support restorations that resemble a tooth or group of teeth. There are several types of dental implants. The major classifications are divided into osseointegrated implant and the fibrointegrated implant. Earlier implants, such as the subperiosteal implant and the blade implant were usually fibrointegrated

WHAT IS A DENTAL IMPLANT? Ø Dental implant is an artificial titanium fixture (similar to those used in orthopedics) which is placed surgically into the jaw bone to substitute for a missing tooth and its root(s).

Surgical Procedure STEP 1: INITIAL SURGERY STEP 2: OSSEOINTEGRATION PERIOD STEP 3: ABUTMENT CONNECTION STEP 4: FINAL PROSTHETIC RESTORATION Success Rates lower jaw, front – 90 – 95% lower jaw, back – 85 – 90% upper jaw, front – 85 – 95% upper jaw, back – 65 – 85%

First Implant Design by Branemark All the implant designs are obtained by the modification of existing designs. John Brunski

Comparison of Implant Systems Astra Tech. ITI Bicon

Perfectly elastic large displacement non-linear contact finite element analysis for different insertion depths. ü Contact pressure increases linearly with insertion depth.

Elastic-plastic large displacement non-linear contact finite element analysis for different insertion depths Bilinear Isotropic Hardening Model Stress (MPA) % Strain

Contact Pressure Distribution for Different Insertion Depths ü Contact pressure increases non-linearly with larger insertion depths.

FUTURE WORK ü Comparison of different implant designs in terms of stress distribution in the bone due to occlusal loads. ü Modeling non-homogenous bone material properties by incorporating with CT scan data. ü Comparison of different implant-abutment interfaces
- Slides: 103