Biochemistry Physiology of Pancreatic Exocrine Secretion Pancreas Secretion

Biochemistry & Physiology of Pancreatic Exocrine Secretion

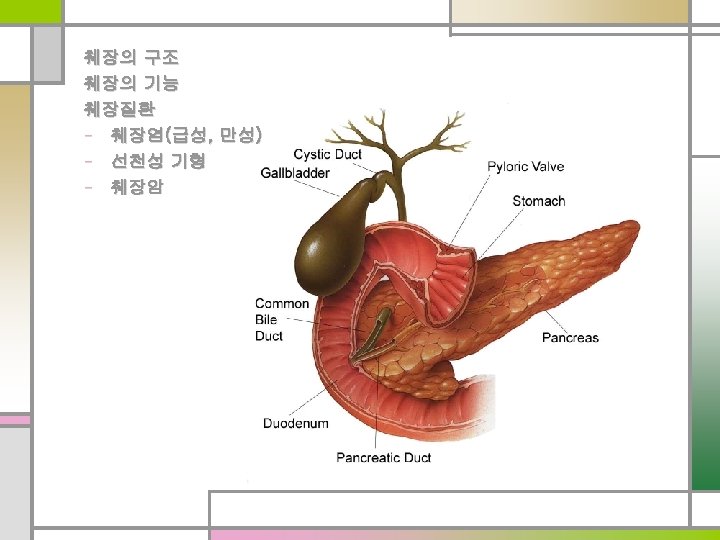
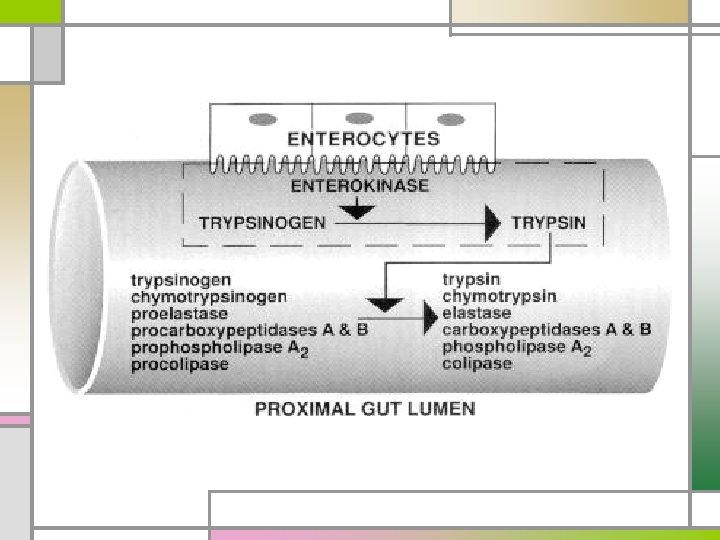
Pancreas Secretion n 1, 500 – 3, 000 ml/day n Isosmotic alkaline (p. H > 8. 0) n 20 enzymes n Zymogens (inactive precursor of proteolytic enzyme) Regulation Hormone Secretin Cholecystokin Optimal p. H for the function of digestive enzymes Autoprotection (protease inhibitor) Nervous system Parasympathetic nervous system -via vagus nerve Release of vasoactive intestinal peptide(VIP)
 Secretion of pancreatic juice n Rich in")
Gastric acid (p. H < 4. 5) Secretion of pancreatic juice n Rich in water & electrolytes n Secretin In the duodenum and jejunum Cholecystokinin • Long-chain fatty acids • Essential amino acids • Gastric acid • Gastrin (same terminal tetrapeptide as CCK ) n Enzyme-rich secretion

n Amylolytic enzymes – Amylase - starch to oligosaccharides or disaccharide Enzyme Excretion n Lipolytic enzymes - Lipase, phospholipase A, cholesterol-esterase n Proteolytic enzymes - Endopeptidase (trypsinogen, chymotrypsin) Cholecystokinin act on internal peptide bonds of proteins - Exopeptidase (carboxy or aminopeptidase) act on carboxyl-teminal and amino-terminal - Elastase Secreted as inactive precursors

Secretin Water & Electrolyte Secretion n Bicarbonate is a ion of primary importance n Good correlation btw maximal bicarbonate output (after stimulation with secretin) & pancreatic mass

Tests of Pancreatic Exocrine Function n Direct stimulation n Study of intraluminal digestion products n Measurement of fecal pancreatic enzymes

Direct Simulation of the Pancreas Secretin stimulation test n Secretin iv infusion, analysis of duodenal content n Principle: Secretory response = functional mass n Normal values - volume output >2. 0 m. L/kg per hour - bicarbonate (HCO 3 -) concentration >80 m. Eq/L - HCO 3 output >10 m. Eq/L in 1 h - most reproducible: max. bicarbonate concentration

n HCO 3 - concentration = Enzyme output ? n Result of the secretin test = Result of absorptive function tests ?

Indirect Stimulation of the Pancreas n Serum trypsinogen level - radioimmunoassay - detect severe damage to the exocrine pancreas n Benzoyl-tyrosyl-p-aminobenzoic (Bentiromide) test - intraluminal chymotrypsin activity n Intraluminal digestion products - undigested muscle fibers, stool fat, fecal nitrogen

Tests Useful in the Diagnosis of Pancreatic Disease n Pancreatic Enzymes in Body Fluids • Amylase n Studies • Lipase • Trypsinogen Pertaining to Pancreatic Structure Ultrasonography CT ERCP EUS
 - normal within")
Serum amylase n Screening test n Acute pancreatitis (> 3 times) - normal within 3 to 5 days - sustained elevation extensive pancreatic necrosis incomplete ductal obstruction pseudocyst formation n Chronic pancreatitis - usually not elevated n Slivary gl, liver, small intestine, kidney, fallopian tube n Malignancy: lung, esophagus, breast, ovary

Table 303 -2. Causes of Hyperamylasemia and Hyperamylasuria PANCREATIC DISEASE NONPANCREATIC DISORDERS I. Pancreatitis I. Renal insufficiency A. Acute II. Salivary gland lesions B. Chronic: ductal obstruction A. Mumps C. Complications of pancreatitis B. Calculus 1. Pancreatic pseudocyst C. Irradiation sialadenitis 2. Pancreatogenous ascites D. Maxillofacial surgery 3. Pancreatic abscess III. "Tumor" hyperamylasemia 4. Pancreatic necrosis A. Carcinoma of the lung II. Pancreatic trauma B. Carcinoma of the esophagus III. Pancreatic carcinoma OTHER ABDOMINAL DISORDERS C. Breast CA, ovarian CA IV. Macroamylasemia I. Biliary tract disease: cholecystitis, choledocholithiasis V. Burns II. Intraabdominal disease VI. Diabetic ketoacidosis A. Perforated or penetrating peptic ulcer VII. Pregnancy B. Intestinal obstruction or infarction VIII. Renal transplantation C. Ruptured ectopic pregnancy IX. Cerebral trauma D. Peritonitis X. Drugs: morphine E. Aortic aneurysm F. Chronic liver disease G. Postoperative hyperamylasemia

Ascitic fluid amylase n Acute pancreatitis - disruption of the main pancreatic duct - leaking pseudocyst n Abdominal disorders - intestinal obstruction - intestinal infarction - perforated peptic ulcer Pleural fluid amylase n Acute pancreatitis n Chronic pancreatitis n Carcinoma of the lung n Esophageal perforation
 n Excellent specificity (99%) n Normal in")
Lipase n Good sensitivity (70 – 85%) n Excellent specificity (99%) n Normal in other cause of hyperamylasemia n Single best enzyme to measure for the diagnosis of AP Trypsinogen or trypsin like immunoreactivity n Organ specific enzyme n Acute or chronic pancreatitis n Increased in renal failure

Radiological studies n Plain films – calcification, ileus n UGI series – displacement of the structures n Ultrasonography – initial investigation of the pancreas n Computed Tomography – best imaging study n Angiography n Endoscopic retrograde cholagiopancreatography, ERCP n Magnetic resonance cholangiopancreatography, MRCP n Endoscopic ultrasonography
 q 현병력: 46 yr/male, 금일")
증 례 q 혈액검사 q 주소: Epigastric pain (today) q 현병력: 46 yr/male, 금일 새벽에 갑자기 발생한 상기 동통 CBC 9, 540(65. 2%)– 14. 6– 314 k Albumin 4. 2 g/d. L Bilirubin (T/D) 0. 5/0. 2 mg/d. L 으로 내원함. q 현병력: 음주력(-) q 동반증상: 특이 소견 없음. q 신체검사: 특이 소견 없음. GOT/GPT 165/85 IU/L ALP/r. GT 98/218 IU/L Amylase/Lipase 957/9624 IU/L Prothrombin time 1. 05 INR

진단은: 급성 췌장염 원인 Gallstones **자세한 문진** • 담석증 과거력, 담도성 동통 • 음주 여부 및 시점 등 Alcohol consumption 초음파 CT ERCP Hyperlipidemia Hereditary pancreatitis Immunosuppressive medications Hyperparathyroidism and hypercalcemia (6 -mercaptopurine, azathioprine) Structural abnormalities Sulfonamide (sulfasalazine, Bactrim) Duodenum/ampullary region Oral 5 -ASA (mesalamine) Bile ducts, pancreatic duct Antibiotics (metronidazole, TC, nitrofurantoin) Sphincter of Oddi dysfunction Medications Infectious agents and toxins Vascular disease Valproic acid Corticosteroids Furosemide Estrogens Mumps, Viral hepatitis, Aldomet coxsackievirus, echovirus, CMV Pentamidine Ascariasis Cystic fibrosis Octreotide Mycoplasma, Campylobacter, Pregnancy Didanosine Mycobacterium avium complex ERCP Postoperative pancreatitis Pancreatic trauma
 Normal finding EUS stones sludges")
ERCP 방사선 검사 (CT) Normal finding EUS stones sludges
 pancreatitis GB stones Treatment ERCP 꼭 해야 하나? ERCP with EST")
Diagnosis Acute (biliary) pancreatitis GB stones Treatment ERCP 꼭 해야 하나? ERCP with EST (Endoscopic sphincterotomy) Cholecystectomy C-duct P-duct

 Alcohol q 복통 (췌장성) q 혈액검사 경과 및")
진단: 급성 췌장 염 원인: 음주력(+) Alcohol q 복통 (췌장성) q 혈액검사 경과 및 치료 n usually within 3 to 7 days after CBC 9, 540(65. 2%)– 14. 6– 314 k Albumin 4. 2 g/d. L Self-limited & spontaneously subside, treatment is instituted (85%-90%). n Treatment: Conventional measures Bilirubin (T/D) 0. 5/0. 2 mg/d. L - analgesics for pain GOT/GPT 165/85 IU/L - iv fluids & colloids ALP/r. GT 98/218 IU/L - no oral alimentation - nasogastric suction in severe case Amylase/Lipase 957/9624 IU/L Prothrombin time 1. 05 INR 방사선 검사: 초음파, CT, ?

방사선 검사 n Conventional x-rays - exclude other diagnoses, esp. perforated viscus n Computed Tomography (CT) - confirm diagnosis, even normal serum amylase - severity, risk of morbidity and mortality n Ultrasonography, Endoscopic Ultrasonograppy (EUS) - evaluate the gallbladder & biliary tree Acute Pancreatitis

CT Grading System of Balthazar & Ranson Grade of acute pancreatitis Points A. Normal pancreas 0 B. Pancreatic enlargement alone 1 C. Peripancreatic Inflammation 2 D. One peripancreatic fluid collection 3 E. Two or more fluid collections 4 Degree of pancreatic necrosis A. No necrosis 0 B. Necrosis of one-third of pancreas 2 C. Necrosis of one-half of pancreas 4 D. Necrosis of more than one-half of pancreas 6 Acute Pancreatitis

Course of the Disease and Complications * Identifying patients with acute pancreatitis who have an increased risk of dying Acute Pancreatitis
 - multiple prognostic criteria -")
Multiple-factor scoring systems n Ranson and Imrie (Ranson’s criteria) - multiple prognostic criteria - increased mortality rate when three or more risk factors n Acute physiology and chronic health evaluation scoring system (APACHE II) - 12 physiologic measurements + age & previous health status - good description of illness severity - score correlates with outcome Acute Pancreatitis

Ranson's Criteria of Severity At Admission Age >55 years Five of the 11 -- intensity of local inflammation Six -- development of systemic complications White blood cells >16, 000/mm 3 Glucose >200 mg/d. L Lactate dehydrogenase >350 IU/L Aspartate transaminase >250 U/L During Initial 48 Hours Hematocrit decrease of >10 mg/d. L Blood urea nitrogen increase of >5 mg/d. L Calcium <8 mg/d. L v Mean Ranson score 1. 6 - mild 2. 4 - severe 5. 6 - lethal v Mortality Pa O 2 <60 mm Hg < 2 : less than 5% Base deficit >4 m. Eq/L 3 -5 : 10% Fluid sequestration >6 L >6 : >60% Acute Pancreatitis

APACHE scoring system

Risk Factors That Adversely Affect Survival in Acute Pancreatitis 1. Organ failure a. Cardiovascular: SBP <90 mm. Hg or tachycardia >130 beats/min b. Renal: oliguria (<50 m. L/h) or increasing BUN or creatinine c. Pulmonary: PO 2 <60 mm. Hg d. Gastrointestinal bleeding 2. Pancreatic necrosis 3. Obesity (BMI > 29); age > 70 4. Hemoconcentration (hematocrit > 44%) 5. C-Reactive protein > 150 mg/L 6. Trypsinogen activating peptide a. > 3 Ranson criteria (not fully utilizable until 48 h) b. Apache II score > 8 (cumbersome) Most useful; Often cited, but less useful Acute Pancreatitis

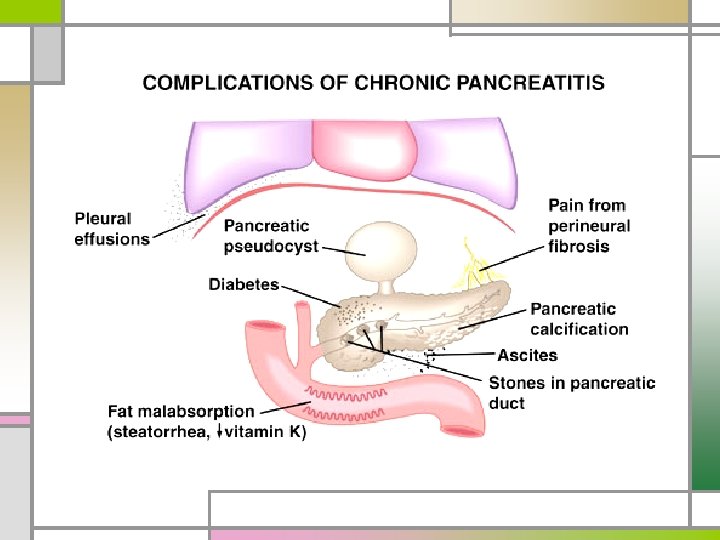
임상 경과 q 통증 지속 q 고열 지속 q 복부 팽만 q 혈청 아밀라제 상승 지속 q 기타 합병증 가능성 확인? infected pancreatic necrosis pancreatic pseudocyst pancreatic abscess Pancreatic ascites

Infected pancreatic necrosis n First 1 to 2 weeks after the onset of pancreatitis n Tx: Surgical debridement - solid component of the infected pancreas - not effective percutaneous evacuation n Secondarily infected in 40 to 60% of patients, Gram (-) bacteria of alimentary origin Acute Pancreatitis

Pseudocyst of the pancreas n Collections of tissue, fluid, debris, enzymes, blood n Over a period of 1 to 4 weeks, 15% of patients

n No epithelial lining n Commonly disrupted pancreatic ductal system n Body or tail area >> head n Serum amylase: elevated in 75%, may fluctuate n Treatment - more than 5 cm in diameter, > 6 weeks - expectant management: best course in selected Pt - size is not an absolute indication for therapy Acute Pancreatitis
 Pain by expansion & pressure on other viscera 2) Rupture")
n Serious complications 1) Pain by expansion & pressure on other viscera 2) Rupture 3) Hemorrhage 4) Abscess n Rupture & hemorrhage - prime causes of death - triad: increase in the size of the mass localized bruit over the mass sudden decrease in hemoglobin & hematocrit Acute Pancreatitis

Pancreatic abscess n Often 4 to 6 weeks later n Less life-threatening, lower rate of surgical mortality n Tx: Surgically or percutaneous drainage n Predisposing factors - severe pancreatitis - postop. pancreatitis, early oral feeding, early laparotomy - injudicious use of antibiotics - communication between a pseudocyst & the colon - inadequate surgical drainage of a pseudocyst - needling of a pseudocyst Acute Pancreatitis

Pancreatic Ascites n Disruption of the main pancreatic duct, Fistula btw the duct & peritoneal cavity or leaking pseudocyst n In ascites, albumin (>3. 0 g/d. L), amylase (>20, 000 U/L) n 15% with pseudocysts, concurrent pancreatic ascites n DDx: intraperitoneal carcinomatosis, TBC peritonitis, constrictive pericarditis, Budd-Chiari syndrome n Treatment - parenteral alimentation to decrease pancreatic secretion - paracentesis - long-acting somatostatin analogue, octreotide - Operation or pancreatic stenting Acute Pancreatitis


Pathogenesis Acute Pancreatitis

Autodigestion n Activated proteolytic enzymes within the pancreas - digest pancreatic & peripancreatic tissues - activate other enzymes (elastase, phospholipase) n Trigger factors: factors Endotoxins, exotoxins, viral infections, ischemia, anoxia, direct trauma Acute Pancreatitis

Activation of pancreatic enzymes Initial phase - intrapancreatic enzyme activation & acinar cell injury - zymogen activation lysosomal hydrolases (cathepsin B) n Second phase - activation, chemoattraction, sequestration of neutrophils in the pancreas n n Third phase - effect of activated enzymes & mediators on distant organs Acute Pancreatitis

Clinical Features Acute Pancreatitis

n Abdominal pain n Nausea, vomiting, abdominal distention n Low-grade fever, tachycardia, hypotension, shock n Jaundice n Erythematous skin nodules n Pulmonary findings (atelectasis, pleural effusion) n Abdominal tenderness and muscle rigidity n Diminished or absent bowel sounds n Pseudocyst n Blue discoloration Acute Pancreatitis

n Abdominal pain n Nausea, vomiting, distention v abdominal Major symptom of acute pancreatitis n Low-grade fever, -tachycardia, hypotension, steady and boring in charactershock n Jaundice n - often radiates to the back, chest, flanks, lower abdomen Erythematous skin nodules n - more intense whenatelectasis, the patient is pleural supine effusion) Pulmonary findings (basilar rales, n Abdominal tenderness and muscle rigidity n Diminished or absent bowel sounds n Pseudocyst n Blue discoloration - epigastrium and periumbilical region Acute Pancreatitis

n Abdominal pain n Nausea, vomiting, abdominal distention n Low-grade fever, tachycardia, GI hypomotility hypotension, shock Chemical peritonitis n Jaundice n Diminished or absent bowel sounds n Pseudocyst n Blue discoloration v Hypovolemia ("retroperitoneal burn") v Kinin peptides n Erythematous skin nodules - vasodilation n Pulmonary findings- increased (basilar rales, vascularatelectasis, permeability pleural effusion) v Systemic of proteolytic n Abdominal tenderness andeffects muscle rigidity & lipolytic enzymes released into the circulation Acute Pancreatitis

ssed e r p m o ead, c h s a e r duct. nc a e l i p b e n h t n Abdominal pain of ommo c c i t Edema a ancre p a r t n i n Nausea, vomiting, theabdominal distention osis r c e fat n s n Low-grade fever, tachycardia, hypotension, shock u o ne a t u c Sub n Jaundice n Erythematous skin nodules n Pulmonary findings n Abdominal tenderness and muscle rigidity n Diminished or n Pseudocyst n Blue discoloration ed w r a p m ith , co e v i s res p m i ain effusion) n (atelectasis, pleural p U e s ten the in nk) a l f , n g r's si bin. e o l n g r o u T f hem us) ( o c i l i absent bowelgsounds m b s i l m n, u tabo a i c s s e ' u n s , tis (Culle m u e n o erit hemop Acute Pancreatitis

Laboratory Data Acute Pancreatitis

n Amylase n Lipase or§ Threefold trypsin or more above normal n - r/o salivary gland disease, gut perforation or infarction Leukocytosis, hemoconcentration with hematocrit - after 48 to 72 h, tend to return to normal n Hyperglycemia - pancreatic isoamylase & lipase, remain elevated for 7 -14 days n § No correlation between severity of pancreatitis & Hypocalcemia n Hyperbilirubinemia degree of s-amylase elevation § Acidemia may have spurious elevations in serum amylase. n Lactic dehydrogenase n Hypoalbuminemia § Normal level - delay (of 2 to 5 days) samples n Hypertriglyceridemia n Hypoxemia - chronic pancreatitis - hypertriglyceridemia Acute Pancreatitis

n Amylase n Lipase or trypsin n Leukocytosis and hemoconcentration with hematocrit helpful in nonpancreatic causes of hyperamylasemia n Hyperglycemia - decreased insulin, increased glucagon release - increased glucocorticoids & catecholamines n Hypocalcemia Intraperitoneal saponification of calcium by fatty acids n Hyperbilirubinemia n Lactic dehydrogenase n Hypoalbuminemia n Hypertriglyceridemia n Hypoxemia - often spuriously normal serum amylase levels - underlying derangement in lipid metabolism Acute Pancreatitis

Diagnosis & Differential diagnosis n Any severe acute pain in the abdomen or back should suggest acute pancreatitis n n n n n Elevated serum amylase and/or lipase Perforated viscus, especially peptic ulcer Acute cholecystitis and biliary colic Acute intestinal obstruction Mesenteric vascular occlusion Renal colic Myocardial infarction Dissecting aortic aneurysm Connective tissue disorders with vasculitis Pneumonia, Diabetic ketoacidosis Acute Pancreatitis

Treatment Acute Pancreatitis

n Self-limited & spontaneously subside, usually within 3 to 7 days after treatment is instituted (85%90%). n Conventional measures - analgesics for pain - iv fluids & colloids - no oral alimentation - nasogastric suction in severe case

n “Rest the pancreas" by inhibiting pancreatic secretion have not changed the course of the disease. - nasogastric suction & anticholinergic drugs - glucagon, H 2 blockers, protease inhibitors, glucocorticoids, calcitonin, NSAIDs, lexiplafant, PAF inhibitor - ineffective n Somatostatin, gabexate methylate – reduced mortality & pancreatic damage n Prophylactic antibiotics – not benefit in mild to moderate Acute Pancreatitis

n Earlier use of fungicides - some benefit in acute necrotizing pancreatitis n Surgical pancreatic debridement (necrosectomy) - infected necrosis n Enteral feeding via nasojejunal tube - decreased rate of complication n Papillotomy - gallstone pancreatitis

n Mild to moderate pancreatitis - fluids, fasting, nasogastric suction for 2 to 4 days - clear liquid diet, start on the third to sixth day - regular diet by the fifth to seventh day n Decision to reintroduce oral intake - decrease in or resolution of abdominal pain - feel hungry - improved organ dysfunction Acute Pancreatitis


Chronic Pancreatitis calcification Pancreatic duct dilatation and stones
, cystic fibrosis (children) n Idiopathic - up to 25%")
n M/C cause: Alcohol (adult), cystic fibrosis (children) n Idiopathic - up to 25% - mutations of the cystic fibrosis transmembrane conductance regulator (CFTR) gene n Persistent abdominal pain, some (~15%) present with steatorrhea & no pain Chronic Pancreatitis

n Autoimmune pancreatitis - Japan and Italy - Characteristics autoantibody in the blood elevated levels of serum Ig. G ass. with other autoimmune dis. (PBC, IBD) diffuse enlargement of the pancreas irregular narrowing of main pancreatic duct - good response to glucocorticoids

Table 304 -5: Causes of Pancreatic Exocrine Insufficiency Alcohol, chronic alcoholism Idiopathic pancreatitis Cystic fibrosis Hypertriglyceridemia Severe protein-calorie malnutrition with hypoalbuminemia Tropical pancreatitis (Africa, Asia) Pancreatic and duodenal neoplasm Pancreatic resection Gastric surgery Gastrinoma (Zollinger-Ellison syndrome) Hereditary pancreatitis Traumatic pancreatitis Abdominal radiotherapy Hemochromatosis Shwachman's syndrome (pancreatic insufficiency and bone marrow dysfunction) Trypsinogen deficiency Enterokinase deficiency Isolated deficiencies of amylase, lipase, or proteases Alpha 1 -Antitrypsin deficiency Chronic Pancreatitis

Pathophysiology n Not well understood n Alcohol-induced pancreatitis n Precipitation of protein in the ducts, resulting ductal obstruction n Direct toxic effects on the pancreas n Extensive pancreatic fibrosis in patients who died during their first attack of alcoholic pancreatitis: already have chronic pancreatitis Chronic Pancreatitis

Clinical Features n Relapsing chronic pancreatitis - pain identical to those of acute pancreatitis - continuous, intermittent, or absent n Abdominal pain - persistent, deep-seated, & unresponsive to antacids - worsened by ingestion of alcohol or a heavy meal - pathogenesis: poorly understood. n Weight loss, abnormal stools, signs or symptoms of malabsorption Chronic Pancreatitis

Diagnostic Evaluation n Serum amylase & lipase - usually not elevated n Abnormal liver function tests n Impaired glucose tolerance, excretion of fecal fat n Triad : calcification, steatorrhea, diabetes mellitus - less than one-third - established the diagnosis of chronic pancreatitis - secretin stimulation test (+) Chronic Pancreatitis

n Pancreas calcification n Alcohol n Severe protein-calorie malnutrition n Hereditary pancreatitis n Post-traumatic pancreatitis n Hyperparathyroidism n Islet cell tumors n Idiopathic chronic pancreatitis Decrease or disappear spontaneously in 1/3 case (dynamic process) Chronic Pancreatitis
 - excessive binding of cobalamin by cobalaminbinding proteins other")
n Cobalamin (vitamin B 12) - excessive binding of cobalamin by cobalaminbinding proteins other than IF - Tx: pancreatic enzyme (proteases) n Impaired glucose tolerance - uncommon DKA, coma, end organ failure n Nondiabetic retinopathy - vitamin A, zinc deficiency Chronic Pancreatitis

n Gastrointestinal bleeding - peptic ulceration, gastritis - pseudocyst eroding into the duodenum - ruptured varices secondary to splenic vein thrombosis n Icterus - edema of the head of the pancreas, compressing the CBD - chronic cholestasis (inflammation around intrapancreatic bile duct) n Pancreatic carcinoma n Addiction to narcotics - most common and troublesome complication Chronic Pancreatitis

Treatment n Two major problems - pain and malabsorption n Intermittent pain - treat essentially like those with acute pancreatitis n Malabsorption (diarrhea and steatorrhea) - pancreatic enzyme replacement therapy n Diet restriction - moderate fat (30%), high protein (24%), low carbohydrate (40%) - restriction of long-chain triglyceride intake - medium-chain fatty acids (not require lipase) Chronic Pancreatitis

Severe and persistent pain n Avoid alcohol & avoid large meals rich in fat n Narcotics n Administration of pancreatic enzymes (75% effect) - effective in mild to moderate exocrine dysfunction - H 2 RA, proton pump inhibitors are effective n Octreotide n Endoscopic treatment n Splanchnicectomy, celiac ganglionectomy n Surgical procedures Chronic Pancreatitis

Hereditary Pancreatitis n Early age of onset & evidence of hereditary factors n Hereditary pancreatitis gene on chromosome 7 - mutation in trypsinogen gene - hydrolysis-resistant trypsin: autodigestion n Frequently pancreatic calcification, diabetes mellitus, steatorrhea, increased pancreatic carcinoma (40% by age 70)
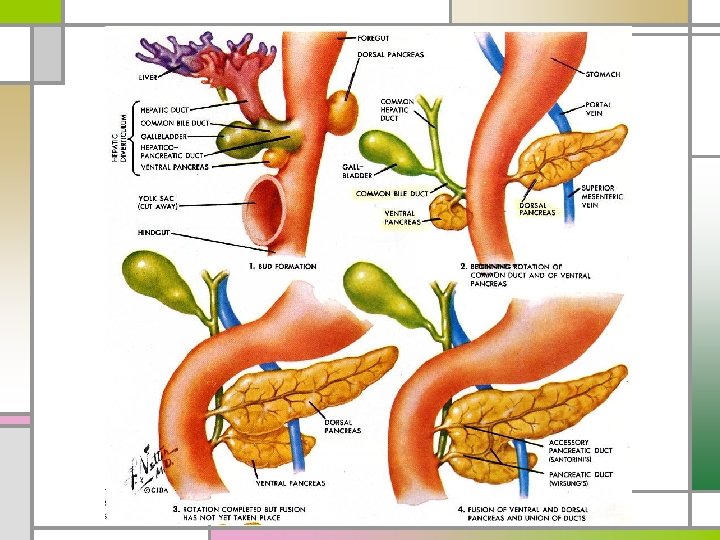

Annular Pancreas n Incorrect migration of the ventral anlage ring of pancreatic tissue encircling the duodenum n Intestinal obstruction in the neonate or the adult n Increased incidence of pancreatitis & peptic ulcer

Pancreas Divisum n Embryologic ventral & dorsal pancreatic anlagen fail to fuse pancreatic drainage through the accessory papilla n M/C congenital anatomic variant of the human pancreas n Combination of pancreas divisum & small accessory orifice dorsal duct obstruction pancreatitis
- Slides: 75