Biochemistry of GIT GASTRIC JUICE Dr Aqsa Malik


Biochemistry of GIT GASTRIC JUICE Dr. Aqsa Malik BIOCHEMISTRY
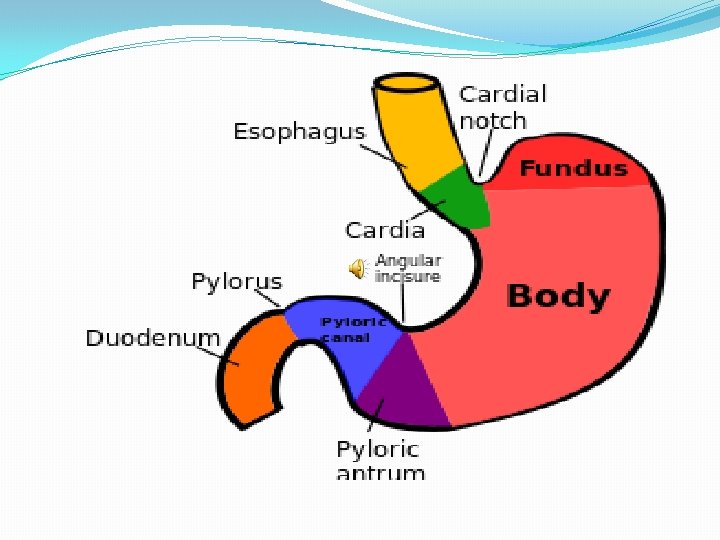

Cells and Secretory Products Cardiac: Mucous Fundus and Body: Parietal , Chief and Mucous. Pyloric: Mucous, Enterochromaffin celllike G cells, D cells.

Composition of the gastric juice �About 99% gastric juice mass is water, while the remaining consists of both organic and inorganic matter. �The organic matter consists of �Mucins, �Pepsinogens[precursors Of Pepsins] �Gastric Lipase �Intrinsic factor �A trace of lactic acid

�The most important inorganic constituent is HCl. Other inorganic constituents are �Na+ �K+ �Phosphate p. H � 1. 3 to 2. 6 Secretion /day �Two to three liters

Properties and Functions of Important Constituents of the Gastric Juice

1. Pepsin: �lt is secreted in the inactive zymogen form called pepsinogen which is initially activated to pepsin by the HCl present in the gastric juice; activation occurs rapidly at a p. H below 2. �Once some pepsin has been formed, it can itself activate more of pepsinogen by what is calledautocatalytic process.
 lt converts proteins")
Pepsin is a powerful proteinase and exerts the following actions: (i) lt converts proteins to smaller fragments, i. e. polypeptides by hydrolyzing specific peptide bonds. (ii) lt curdles milk. This occurs due to the conversion of the milk protein casein into paracasein by a partial hydrolysis. Paracasein combines with Ca 2+ ions to form calcium paracaseinate which being insoluble is responsible for curdling.

2. Gastric lipase: �Its activity is confined to the stomach as it is destroyed by trypsin. �lt is much more active against fats containing short and medium chain fatty acids, e. gr milk fats. �It is stable in acid medium.

3. Mucins: �These are carbohydrate-containing proteins that are present in the mucus, and act as lubricating agents by forming a slippery layer over the mucosa of the stomach. �This layer of mucin also acts as a barrier to the action of gastric juice on stomach wall and thus helps in preventing the digestion of the stomach itself; moreover, mucin has an anti-pepsin activity and also has a buffering action against HCL.

4. Intrinsic factor: �This factor is glycoprotein in nature and is required for the active absorption of vitamin B 12 from the ileum. �Its lack results in vitamin B 12 deficiency and produces pernicious anemia. �The formation of the intrinsic factor is the only function of the stomach that is essential for life.
 lt activates pepsinogen to pepsin. (ii) It lowers the p. H")
5. HCI: (i) lt activates pepsinogen to pepsin. (ii) It lowers the p. H of the gastric juice so that pepsin can have a favorable p. H for digestion of proteins. (iii) lt has an antiseptic action which prevents the growth of microorganisms in the stomach. When gastric juice is low in HCL (hypochlorhydria) or when HCI is totally absent (achlorhydria), there occurs microbial growth in the stomach as shown by an increased lactic acid level in the gastric juice.
 It helps in the absorption of iron as it helps in the release")
(iv) It helps in the absorption of iron as it helps in the release of iron from its bound form in food ; moreover, it has a role in converting ferric to ferrous form which is easily absorbed. (v) When the gastric contents enter the duodenum, the HCl contained in them stimulates the release of a hormone namely secretin into the blood stream.
 �Somatostatin")
HCl increase: �Acetylcholine �Histamine �Gastrin HCl decrease: �Prostaglandin (PG) �Somatostatin

Role of gastric juice hypotonicity �The hypotonicity of the gastric juice helps in decreasing the tonicity of the hypertonic ingested food towards isotonicity with plasma. � ln patients whose stomach has been removed, this function is lost and the entry of hyperosmotic food into the small intestine results in severe symptoms collectively termed the dumping syndromes
 �The secretion of HCl is an active process")
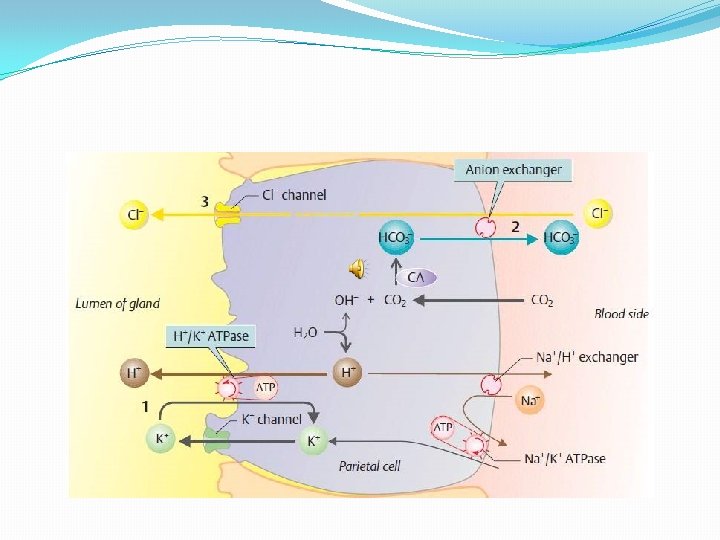
Mechanism of HCl Secretion (Proton Pump) �The secretion of HCl is an active process needing ATP. �The parietal cell has a basolaterel portion and an apical portion. �There is an intracellular canaliculus into which ions like H+, Cl- and K+ and water make entry; from here HCl and water enter into the glandular lumen and thereafter into the gastric lumen.

1. The enzyme carbonic anhydrase catalyzes the reaction CO 2 + H 2 O —> H 2 CO 3. 2. H 2 CO 3 splits into H+ and HCO 3. The importance of this enzyme action in HCl production is shown by the fact that administration of its inhibitor acetazolamide, decreases HCI formation. 3. The H+ ion is actively secreted into the canaliculus of the parietal cell by H+ K+ ATPase also called the gastric proton pump. This enzyme is inhibited by omeprazole which very effective. In decreasing the HCI secretion in Patients of peptic ulcer disease.

4. The intracellular HCO 3 is exchanged across the basolateral membrane for extracellular Cl- by the HCO 3 -/Cl- exchanger. �As Cl- concentration within the cell increases, these ions are driven across the apical membrane into the canaliculus, where along with H+ they form HCl. The HCO 3 - enters the interstitial fluid from where it passes on into the blood. �lt is obvious that for each H+ secreted into the gastric juice, one HCO 3 - enters the blood. �Thus during periods when HCl production is rapid, the plasma p. H rises somewhat; this is called the postprandial (after taking a meal) alkaline tide.

5. The intracellular K+ is kept at high level by Na+K+ ATPase at the basolateral membrane. �Potassium ions move into the lumen of the canaliculus and are used to drive H+K+ ATPase. Some K+ ions also diffuse into the intracellular canaliculus. �The overall reaction can be summarized by the equation, �CO 2+ H 20 + Cl- ----> HCl + HCO 3 -

Regulation of the Secretion of Gastric HCl 1. Basal or resting secretion: � Basal secretion of HCI is more during night and is least in the morning.

II. Stimulated secretion, i. e. secretion of gastric juice in response to a meal: This can be divided into three phases which are termed cephalic, gastric and intestinal phases. 1. Cephalic or neural phase: � This results from the stimulation of gastric secretion produced by sight, smell, taste or even thought of food.

2. Gastric phase: �This phase is seen when food enters the stomach and stimulates the secretion of the gastric juice. �Distension by the stomach stimulates HCI secretion by stimulating stretch receptors in the wall and mucosa of the stomach. 3. Intestinal phase: �The intestinal influences on gastric secretion are exerted through reflex and hormonal feedback mechanisms. �The hormone through which this secretion is mediated: �Gastrin �CCK

Stimulants of Gastric HCI Secretion � 1. Parasympathetic nerves: �Vagal stimulation produces its effects by releasing acetylcholine as well as by releasing gastrin and by decreasing release of somatostatin. �Cholinergic drugs, e. g. �pilocarpine are strong stimulants of gastric glands.

2. Histamine: �It is a very powerful stimulant of parietal cells and therefore the juice produced is rich in HCl. �Conditions in which histamine is liberated in the body such as burns lead to a greater secretion of the gastric HCI; this explains the occurrence of peptic ulcers as a complication of extensive burns (Curling’s ulcers). �An analog of histamine, histalog, stimulates gastric secretion, but does not produce the undesirable side effects seen with histamine; it is used for testing the gastric secretory activity.

3. Gastrin: �its role has been already described. Gatrin release from the G cells is increased by vagal stimulation through release of gastrin releasing peptide. �Gastrin acts through gastrin receptors of the parietal cells but its main action is via stimulating the release of histamine from the enterochromaffin-like (ECL) cells. �A commercially available preparation is pentagastrin which consists of the terminal tetrapeptide part of the natural gastrin and in addition contains a derivative of β-alanine.

� 4: Ca 2+ ions: These ions increase gastric HCl Secretion. Peptic ulcer may occur in hypercalcemia states, e. g. hyperparathyroidism. � 5. Caffeine: It is present in tea, coffee and cola beverages. � 6. Alcohol: It stimulates the secretion of a juice rich in HCl by a direct action of the gastric glands. � 7. Nicotine: In small doses it stimulates gastric glands.

8. Proteins: Food rich in proteins increases the liberation of gastrin, whose effects have already been described. 9. Food flavors: These include chillies, condiments, etc. These act by adding flavor to the food which stimulates, the cephalic phase of gastric secretion. 10. Alkalies: Na. HCO 3 in small doses increases HCI secretion because alkaline p. H in the pyloric antrum stimulates the release of gastrin.

11. Psychological factors: �Chronic anger, resentment , chronic anxiety and fear increase the secretion of gastric juice which is rich in HCl. �Peptic ulceration may be seen when a person is faced with excessive stress (stress ulcers). 12. Medication: �Drugs that inhibit prostaglandin formation, e. g. nonsteroid anti-inflammatory drugs (NSAID) that include acetylsalicylic acid (aspirin) and many commonly used "pain-killers" increase gastric acidity. �This is because prostaglandin decreases gastric acidity.

13. Hormones: By producing hypoglycemia insulin increases secretion rich HCl through vagal center in the brain; Glucocorticoids when given in large doses over a long time also increase gastric acidity; the effect is probably due to interference with formation of antibodies against H. pylori.

Depressants of HCl secretion 1. Fats: � The ingestion of fats decreases the secretion of HCl and also decreases the motility of the stomach. � Both of these effects delay the emptying of the stomach after a fatty meal. � Fat acts through releasing a hormone called enterogastrone from the small intestine. 2. Acids �These depress gastric secretion because an acid p. H in the pyloric antrum inhibits the release of gastrin.

3. Alkalies in large doses 4. Parasympatholytic drugs �Atropinc and synthetic anticholinergic Agents. 5. Sympathetic stimulation �This inhibits gastric secretion through α-2 adrenergic receptors. 6. Anti-histamine drugs: �Those anti-histamine drugs that block histamine actions through H 2 receptors greatly decrease HCI secretion; these drugs are cimetidine and ranitidine.

7. Anti gastrin substances: �a compound named proglumide which act as strong anti gastrin. 8. Proton pump inhibiting drugs: �omeprazole 9. Secretin: �It decreases HCI secretion; however , it stimulates pepsinogen. 10. Prostaglandins �These substances inhibit HCI secretion by inhibiting activation of adenylyl cyclasé. PGs also increase the mucus and HCO 3.

�Analogs of PGE 2 are used in the treatment of peptic ulcer disease. Non-steroidal anti-inflammatory drugs (NSAIDs) which inhibit cycloxygenase i. e. COX-1 activity decrease the Formation of PGE 2 and increase HCI formation. COX-2 inhibitors do not show this action on the stomach. 11. Psychic factors: �Sudden fear, pain and mental depression decrease the secretion of gastric juice.

Peptic ulcer disease �This disease affects both the stomach and the duodenum producing gastric and duodenal ulcers. �A peptic ulcer is defined as a break in the mucosal surface more than 5 mm in size and extending deep into the submucosa. �Both HCl and pepsin can damage the gastro-duodenal mucosa, but the role of pepsin in the pathogenesis of peptic ulcers is not established.

�Two important factors in the production of this disease are therapeutic use of COX-1 -inhibiting. NSAIDs that inhibit the production of PGs whose protective roles have been already described and infection by H. pylori. � Eradication of H-pylori has greatly decreased the incidence of this disease.

�COX-2 - inhibiting NSAIDs have been used in place of COX-1 inhibiting NSAIDs; these drugs decrease the incidences of peptic ulcer. � H. pylori resides in the stomach and duodenum and produces ulceration by several mechanism that include increased gastric secretion, release of cytokines that injure the mucosa and a decreased secretion of mucosal HCO 3 -.
- Slides: 39