biochemical persistent MTC Omid Gharooi Ahangar Clinical question

biochemical persistent MTC Omid Gharooi Ahangar

Clinical question i. what is the significance of calcitonin level after surgery? ii. What is the calcitonin level cut off for prediction of recurrence? iii. What we should be do in biochemical persistent MTC, when usual imaging can not localize recurrence? iv. What happen if we ignore the elevated calcitonin level in normal imaging patient? v. what is standard treatment & F/U of locally advance MTC?

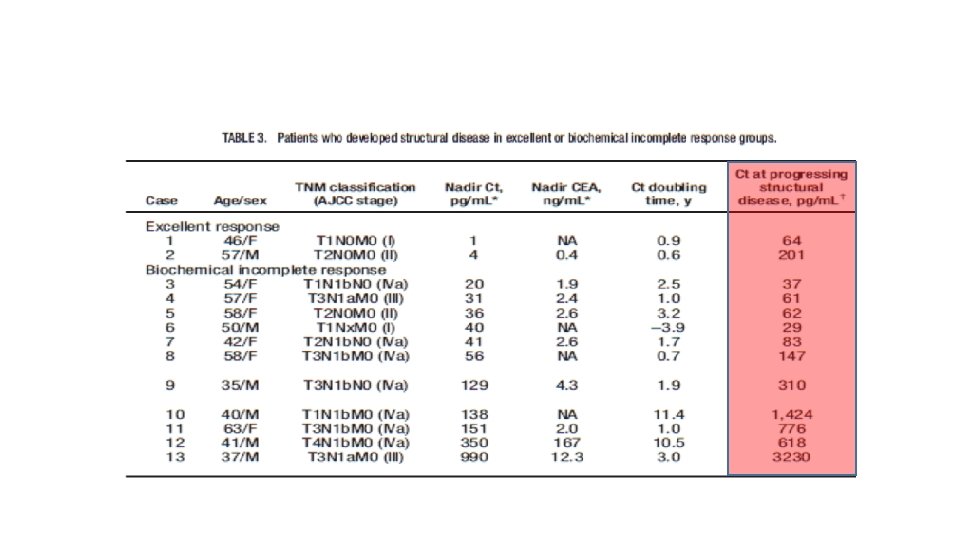
i. what is the significance of calcitonin level after surgery? ii. What is the calcitonin level cut off for prediction of recurrence?

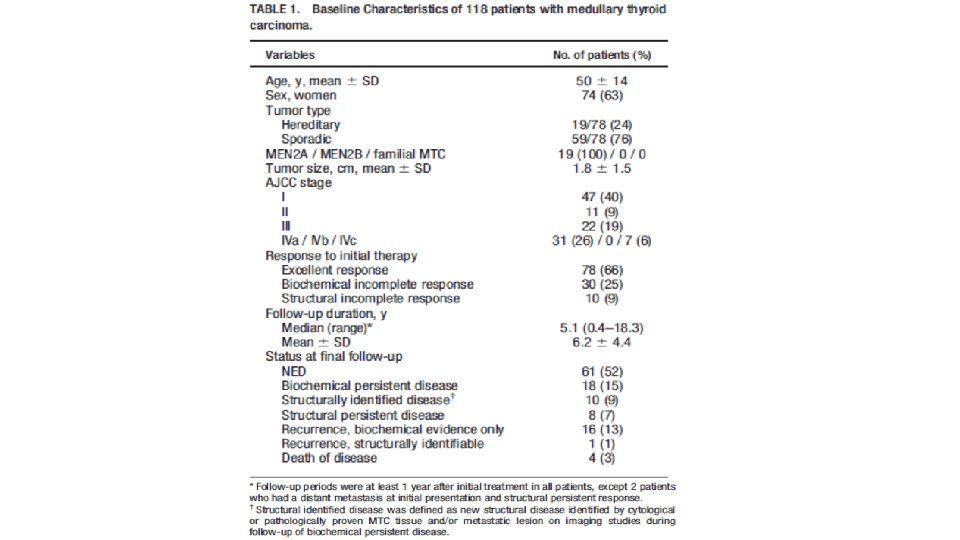
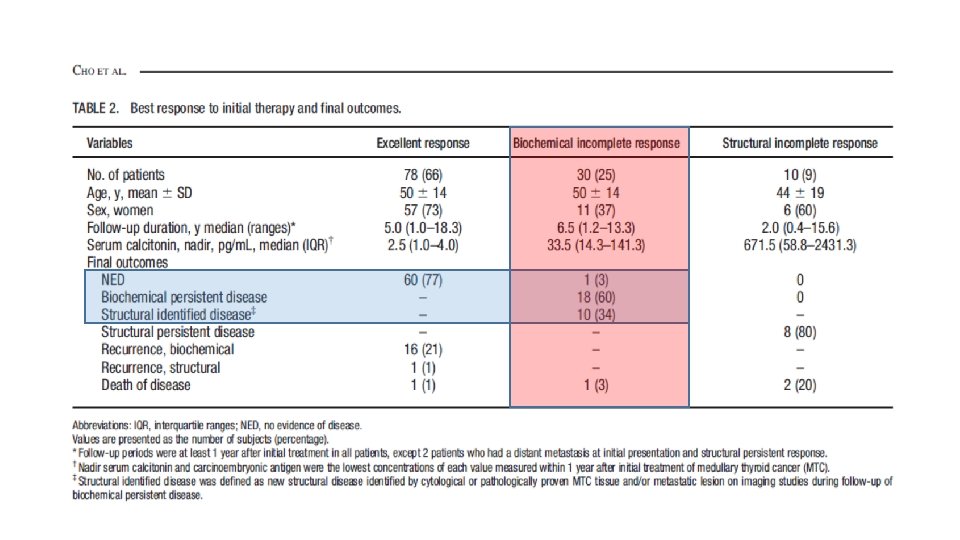
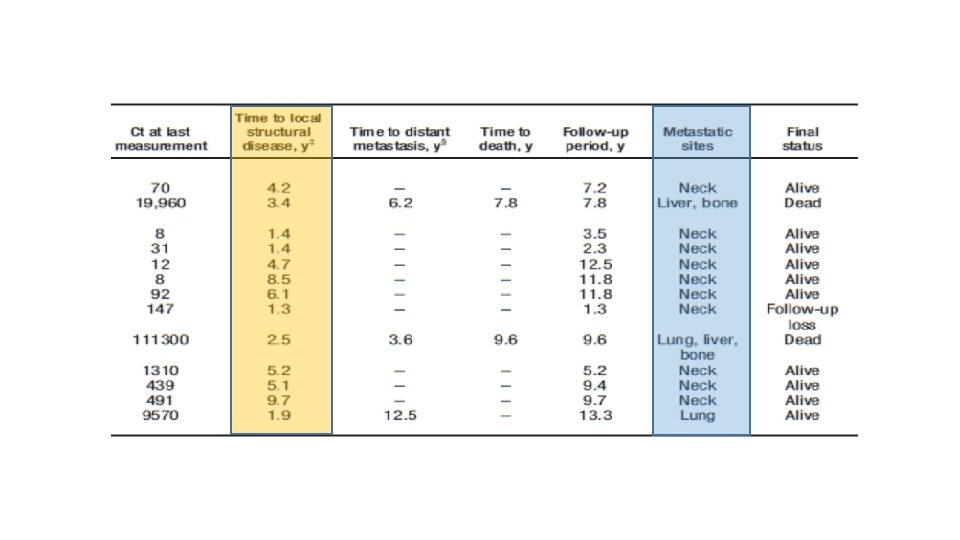
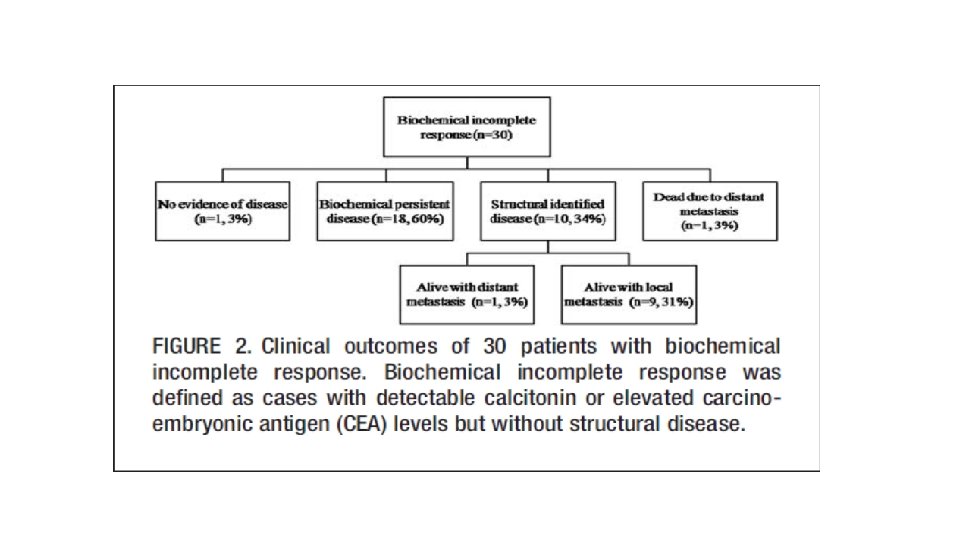
MATERIALS AND METHODS • We retrospectively reviewed patients who underwent thyroid surgery for MTC at Samsung Medical Center between May 1996 and May 2015 (n=140). • After exclusion, a total of 118 patients were eligible for the analysis. • Patients were classified as follows: (1) excellent response, undetectable calcitonin, and normal CEA levels without structural disease; (2) biochemical incomplete response, detectable calcitonin, or elevated CEA levels without structural disease; or (3) structural incomplete response, persistent structural disease regardless of serum calcitonin, and CEA levels.

What we should be do in biochemical persistent MTC, when usual imaging can not localize recurrence?

• Fifty-five consecutive MTC patients were enrolled in the study from January 2005 until August 2006. • There were 21 women and 34 men, with a median age of 56 yr (range 14– 83 yr). • Five patients had a multiple endocrine neoplasia 2 a syndrome, three had a multiple endocrine neoplasia 2 b syndrome, four had a familial MTC, and finally 43 had a sporadic MTC. • Median follow-up after initial surgery was 79 months (range 3– 309 months). • At the time of the study, plasma calcitonin level ranged from 21 to 247, 000 pg/ml (median 1250), and CEA level ranged from 1 to 5845 ng/ml (median 37).

Imaging results • The standardized imaging work-up led to the diagnosis of local recurrence or metastases in 45 of 55 (82%) patients with a median calcitonin level at 1534 pg/ml (range 21– 247, 000 pg/ml) but found no lesion in the remaining 10 (18%) patients with a median calcitonin level at 196 pg/ml (range 39– 816).
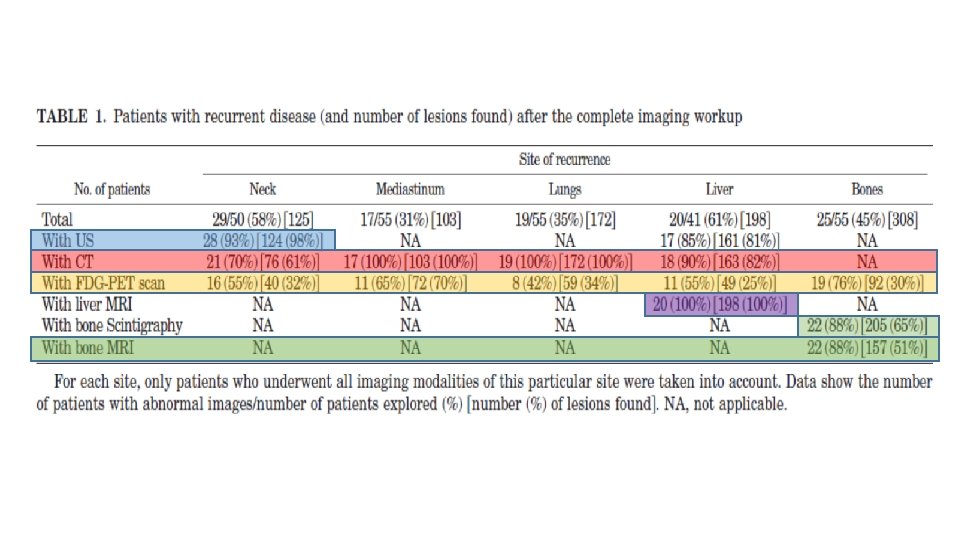
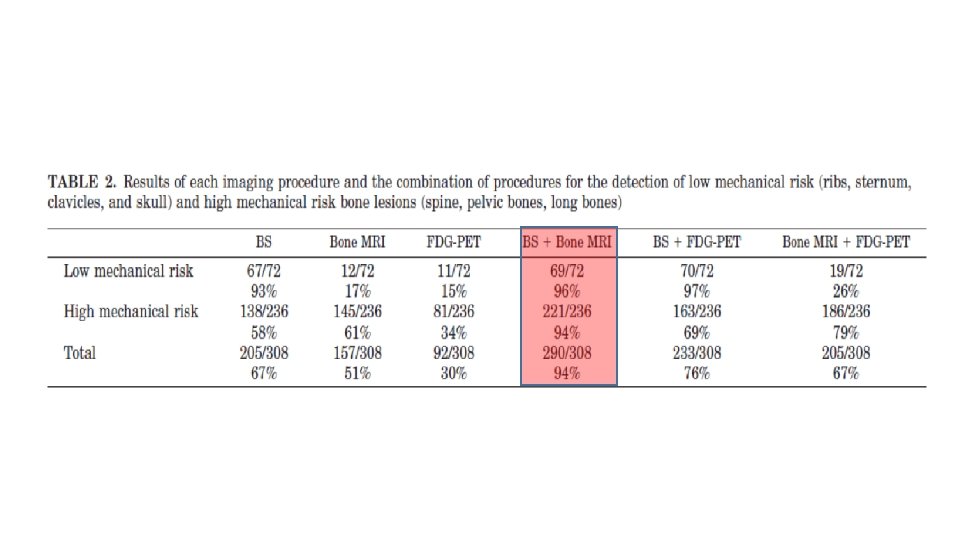
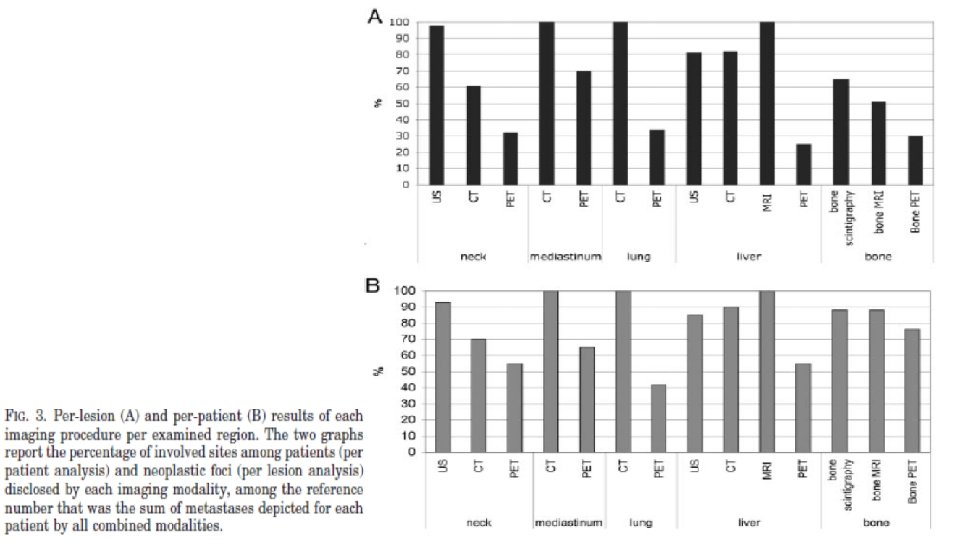

conclusion • In conclusion, imaging MTC would consist in the combination of neck ultrasonography, chest spiral CT, liver MRI with standardized procedures, and both bone scintigraphy and axial bone MRI. • Using these imaging modalities we were able to detect 98% of neck recurrences; 100% of mediastinal lymph nodes, lungs, and liver metastases; and 94% of bone metastases. • FDG PET has no place in routine imaging of medullary thyroid cancer, and its prognostic value is low.
![Materials and Methods • This is a prospective study of [18 F]FDG-PET/CT scans performed](http://slidetodoc.com/presentation_image_h/bddae184b96c368a405599d1e99850df/image-23.jpg "Materials and Methods • This is a prospective study of [18 F]FDG-PET/CT scans performed")
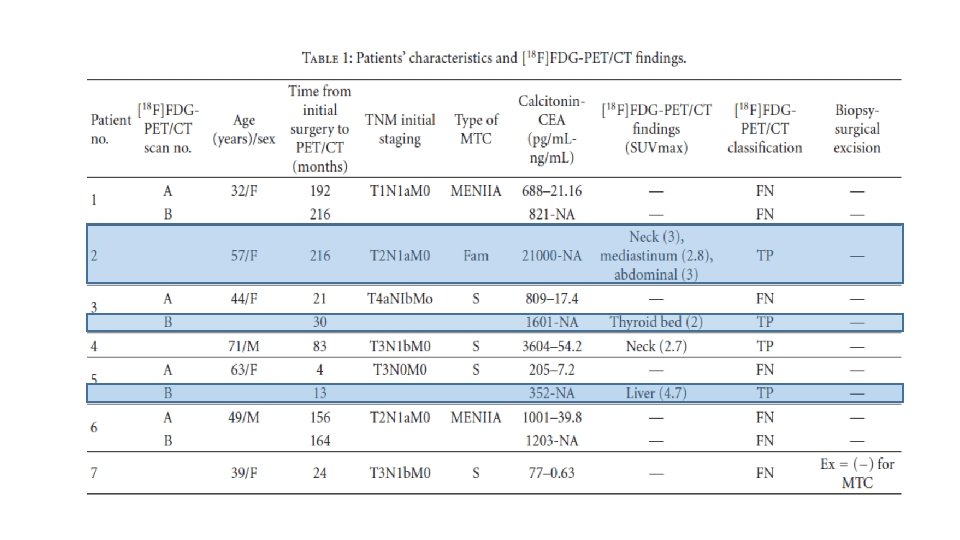
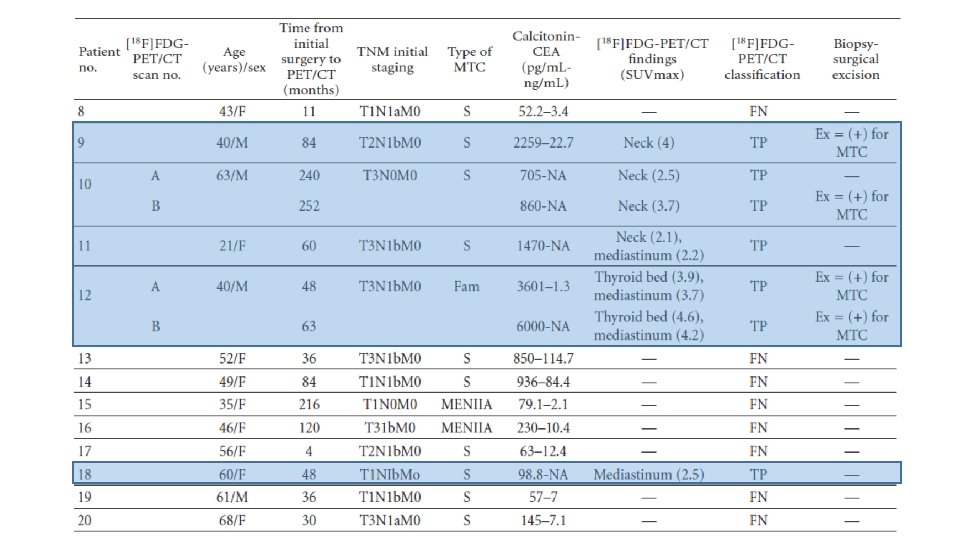
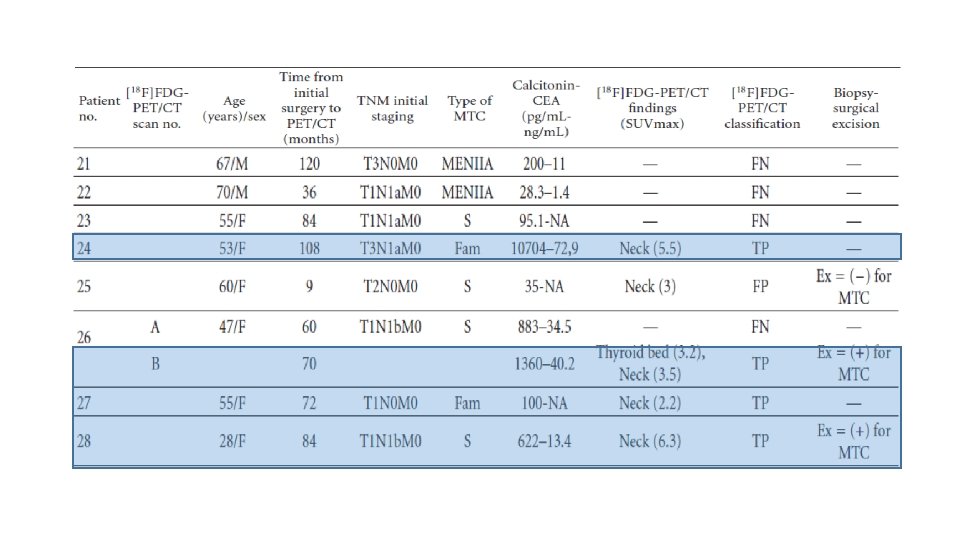
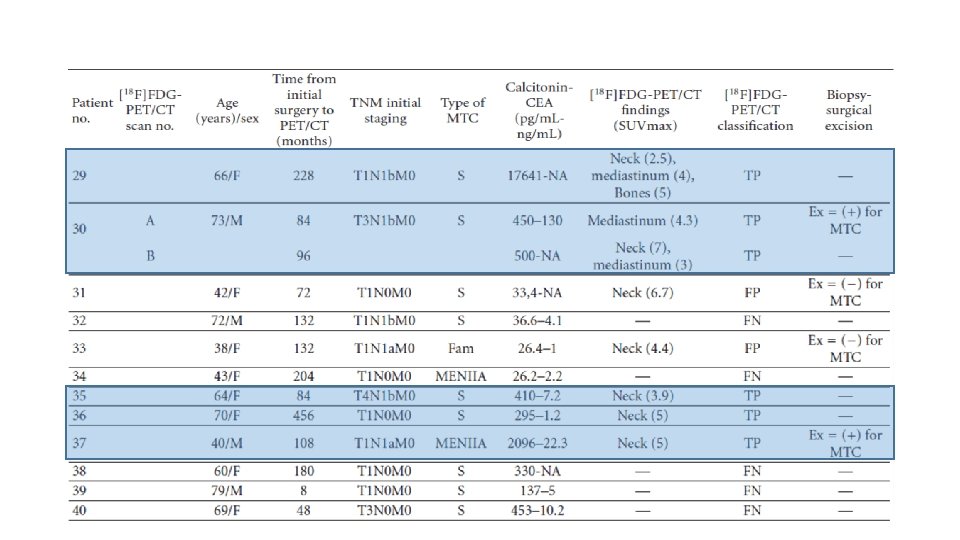
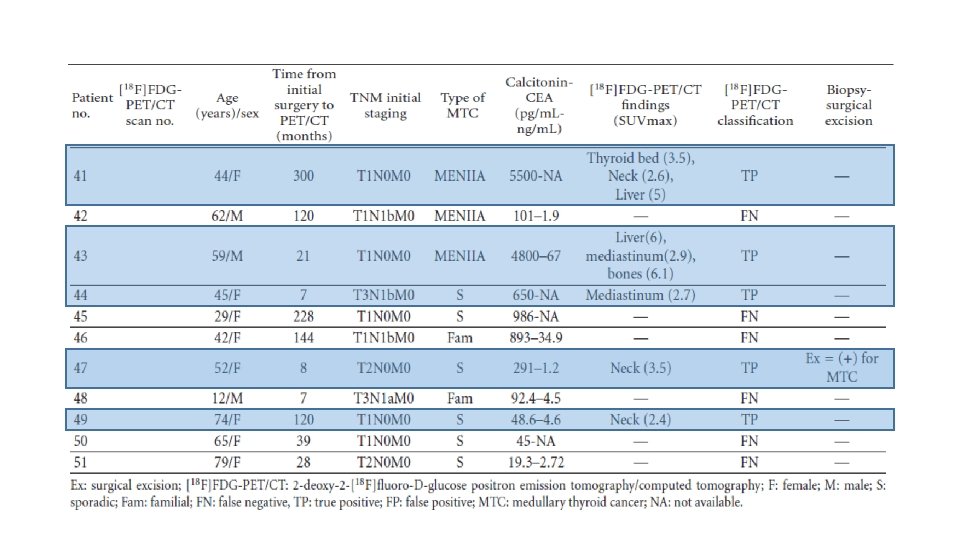
Materials and Methods • This is a prospective study of [18 F]FDG-PET/CT scans performed for localization of recurrent disease on patients with histologically proven MTC, elevated calcitonin levels, and negative or equivocal conventional imaging findings. • From February 2007 to February 2011, 59 scans were performed on 51 patients with MTC. • The group included 15 men and 36 women, 12– 79 years old (mean: 53± 15. 17 years). • 18 patients had hereditary MTC and 33 sporadic MTC. • Median follow up after initial surgery until performing [18 F]FDG-PET/CT was 8. 4 years. • All patients were asymptomatic and all had elevated serum calcitonin levels (19. 3– 21000 pg/m. L). 22 patients also had elevated CEA levels (7. 2– 130 ng/m. L).
![Conclusions • It seems that the sensitivity of [18 F]FDG-PET/CT scan for the detection](http://slidetodoc.com/presentation_image_h/bddae184b96c368a405599d1e99850df/image-29.jpg "Conclusions • It seems that the sensitivity of [18 F]FDG-PET/CT scan for the detection")
Conclusions • It seems that the sensitivity of [18 F]FDG-PET/CT scan for the detection of MTC recurrence, in patients with elevated calcitonin levels and negative or equivocal conventional imaging findings, is determined by the level of serum calcitonin. • The results from this cohort of patients suggest that [18 F]FDG-PET/CT provides additional information in almost half of all cases (44. 1%) detecting occult sites of calcitonin production or confirming equivocal findings of other imaging modalities • However, when the calcitonin levels were greater than 1000 pg/m. L, this rate increased to 86. 7%. • It also seems that the sensitivity of this method is better in patients with sporadic or familial MTC than in those with MTC as part of MEN IIA syndrome.

What happen if we ignore the elevated calcitonin level in normal imaging patient?

• What is standard treatment & F/U of locally advance MTC?

What we do Before surgery?

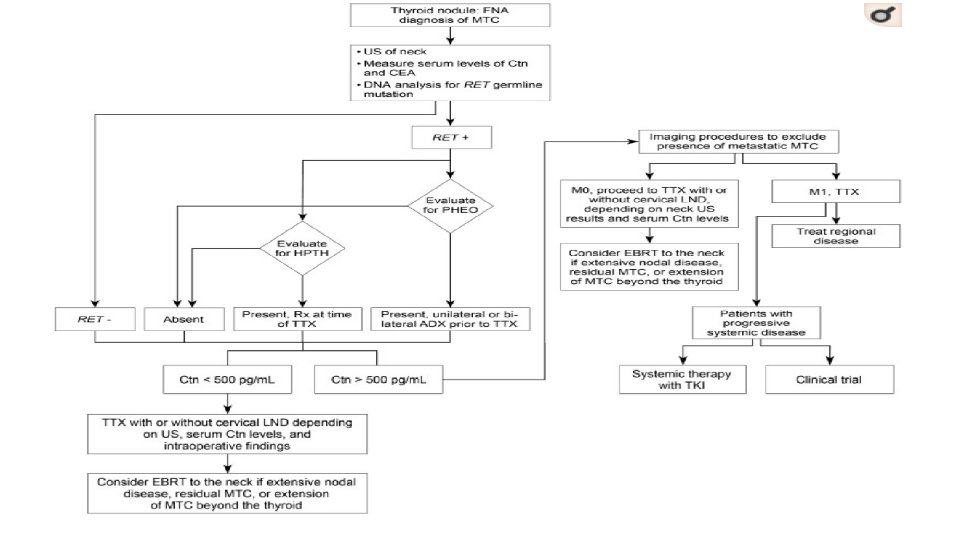
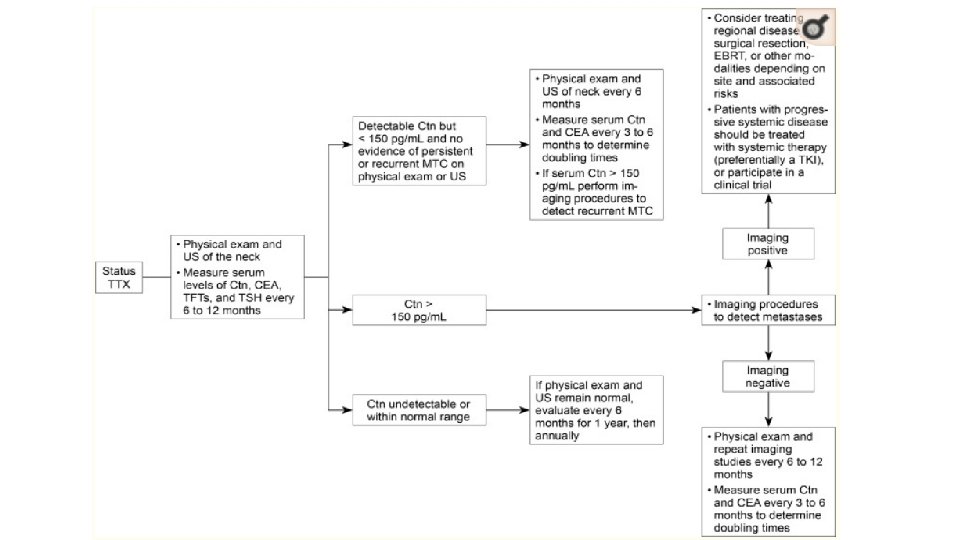
Management of Patients with Locally Advanced or Metastatic MTC

What we do after surgery?
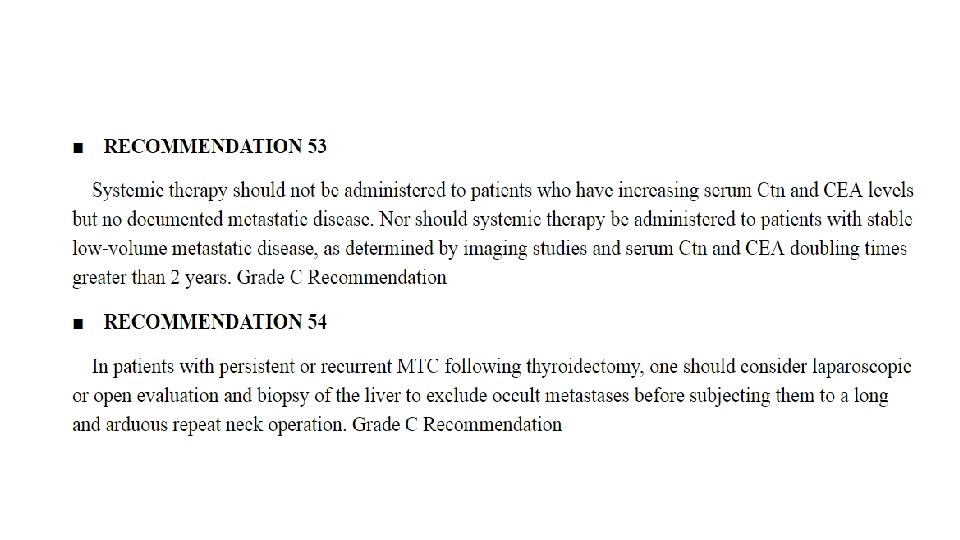
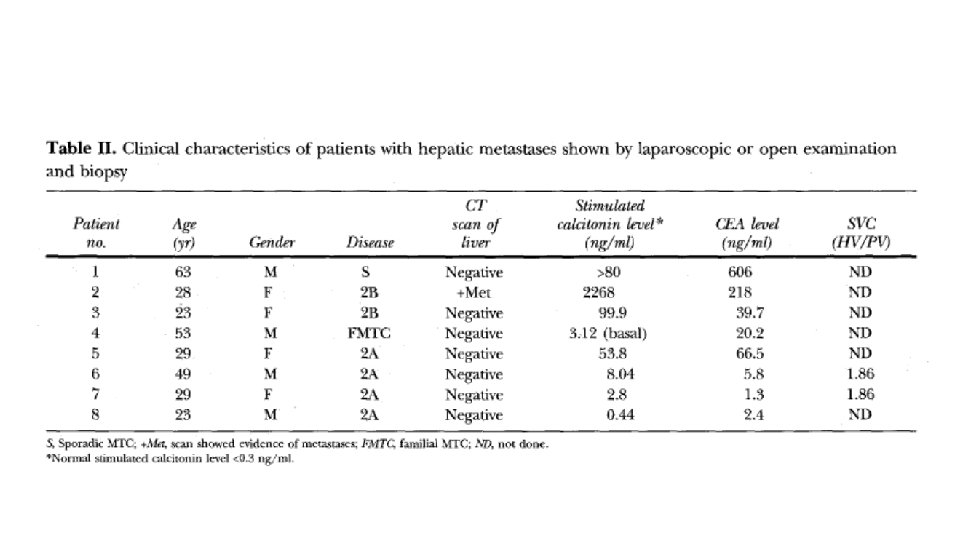

It is important to remember • Most asymptomatic patients with elevated serum Ctn levels and occult metastatic disease are not surgical candidates because natural history studies indicate that many of them have a relatively good prognosis, especially if the Ctn and CEA doubling times exceed 2 years.

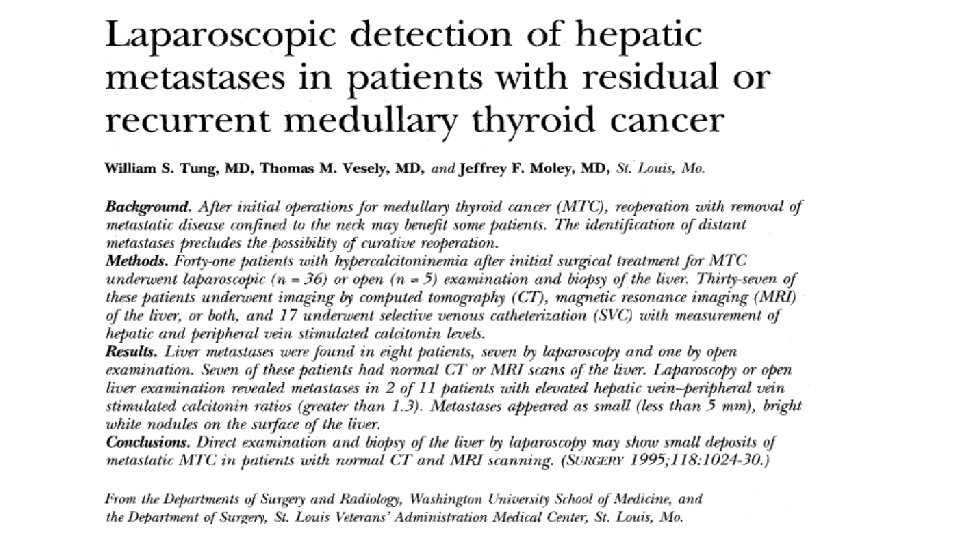
What we should be do in our patient? ØMRI of liver ØMRI of axial bone and pelvic if feasible ØRepeated PET if calcitonin rise above 1000 ØLaparoscopic evaluation of liver? ?
- Slides: 47