Billing and Coding Billing Submitting your code Coding

Billing and Coding

Billing • Submitting your code.

Coding • Giving your hard work a number

Coding Components • • HX ROS PFSH PE bullets # of diagnoses Data Risk
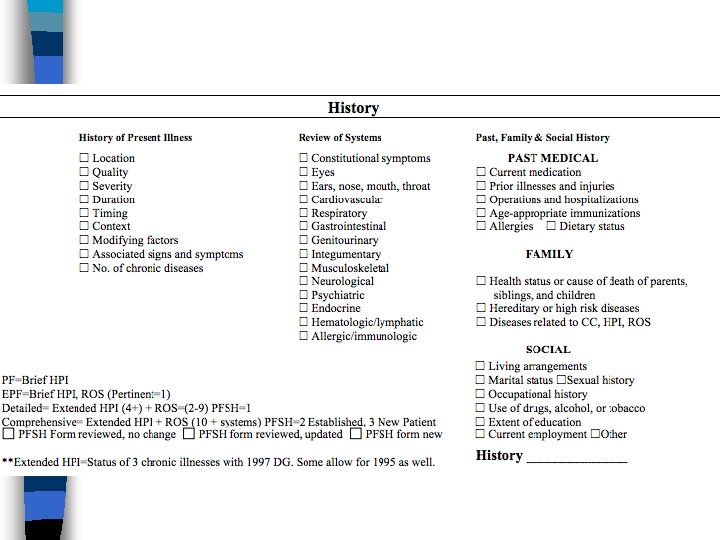

HPI • Location- Be specific • Quality- sharp, stabbing, dull • Severity- Pain scale, or overt (child was up all night crying) • Duration- Chest pain started yesterday • Timing- joint pain, worse in the morning • Context- Fever, recent travel to Mexico • Modifying-alleviating or worsening • Associated- CP with SOB

Review of Systems • One item in each system • CAN be documented in HPI • CANNOT Double dip with HPI

PFSH • Medical • Family • Social • MUST BE PERTINENT

Calculating History 3/3 HPI ROS PFSH HX <4 0 0 Problem Focused 1 >/=4 3 C Expanded Problem Focused 2 -9 1/3 Detailed >/=10 2/3 E Complex 3/3 N 3 C= Three Chief Complaints
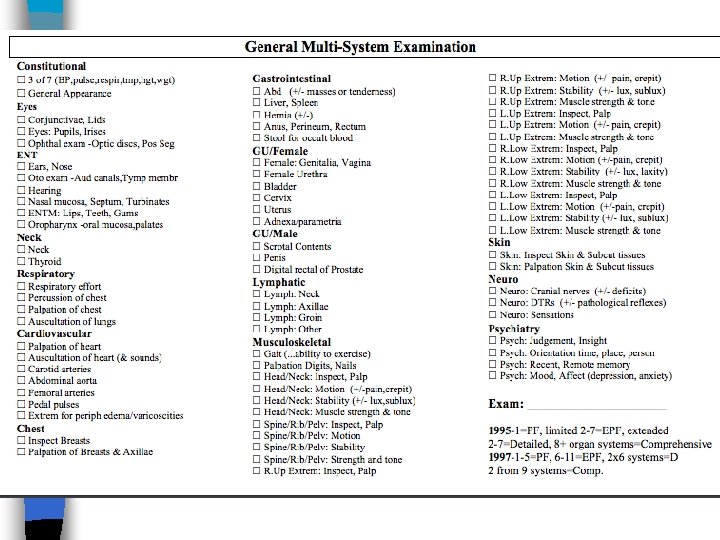

Physical Exam Level <6 Problem Focused >/=6 Expanded Problem Focused >/=12 Detailed 2 in 9 Complex

Medical Decision Making • Bringing it all together! • Best 2/3
 • Max")
Diagnosis Points • #Dx. P • Self-limited minor problem (1 pt each) • Max 2 of these • Ex. Skin tag, hangnail, dry skin • Established Problem stable(1 pt each) • Established dx to the PROVIDER • Ex well-controlled diabetes • Established Problem unstable (2 pts each) • Ex. Uncontrolled diabetes
 • ONLY ONE,")
Diagnosis points continued • New Problem- no work-up (3 pts each) • ONLY ONE, New to PROVIDER • Ex. Acute sinusitis, well-controlled HTN • New Problem- Work-up (4 pts each) • Ankle injury with x-ray • UTI with urinalysis

Diagnosis Points Each Problem Established Adequately Controlled 1 pt New Inadequately controlled 2 pts No Additional work up 3 pts Additional work up 4 pts
 • Review/order radiology (1 pt max)")
Data • Review /order tests (1 pt max) • Review/order radiology (1 pt max) • Review/order Medical test (1 pt max) • Ie sleep study, nuclear scan • Discuss results with radiology/cardiology (1 pt max) • Independent review (can’t charge if radiology is looking) (2 pt max) • Request old records (1 pt max) • Review and summarize old records (2 pt max)
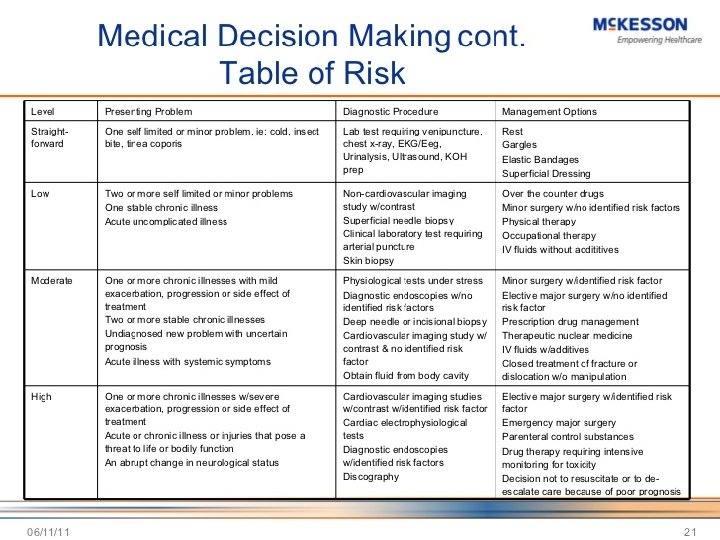

Determining level of decision making 2/3 x #Dx. P Data Risk MDM 0 -1 Minimum Straight forward 2 2 Low Complexity 3 3 Moderate complexity 4 4 High complexity

New and Established Patient • New: A patient who has not received any professional services from the physician or another physician of the same specialty who belongs to the same group practice, within the past three years. • Established: A patient who has been seen within the past three years. New > Three Years

Practice 1 • Office visit • Follow-up HTN, DM • 75 year old male with a history of DM, HTN here for six month follow up. Doing well and taking medication. Denies chest pain, SOB. BS has been running 110 -120. Watching diet • PMH- Medications and allergies reviewed • Exam- NAD, VS: Pulse, HR, RR normal, CV: RRR, Lungs: CTAB, Ext: warm dry, no clubbing, cyanosis, edema • Assessment- 1. HTN Controlled 2. DM at goal • Plan: Continue current meds, return in 6 months

Practice 2 • 45 year old male with HTN, c/o right knee pain for 2 weeks. Denies injury. Tried Aleve with some improvement. Denies fever, other joint pain. States taking lisinopril without problems. No chest pain, no SOB. Just moved from Indiana • PMH: HTN, S/P appendectomy • Med: Lisinopril, NKDA • Fam hx. Osteoarthritis • Exam: BP 120/60, HR 73, RR 18, NAD, No JVD, Thyroid normal. CV RRR, no murmurs, no rubs. Lungs CTAB. Ext: no clubbing cyanosis or edema, R. Knee: minimal swelling no redness Full ROM • X-ray obtained- Degenerative changes • Assessment: HTN controlled, Knee pain (probably DJD) • Plan: Continue lisinopril, start celebrex. Return 1 mth recheck

Practice 3 • CC: Follow up HTN • HPI: 40 year old taking meds without complaint. No CP, had headache 3 days ago, but is now gone. No neuro symptoms. Headache was “tightness” that got better after patient left work. Has same kind of headaches about every couple of months when stressed. • Meds/Allergies: reviewed per HER • Exam: HR 90, BP 150/80, RR 18, NAD. PERRLA, EOMI, neck supple, CV RRR, Lungs CTAB, Neuro: oriented x 3, DTRs normal, sensation intact • Assessment: HTN, not controlled • Plan: Increase HCTZ

Practice 4 • Abdominal pain • 58 year old female c/o abdominal pain and dysuria for 4 days. It has gotten worse today and she feels she has to urinate every 30 min. Also had fever and nausea. She denies flank pain and vaginal d/c. Has tried cranberry juice • PMH: NIDDM • Meds: Metformin; PCN allergy • Social hx: sexually active with husband • VS: 130/80, 12, T 100 F • NAD, CV: RRR no murmurs, Pulm: CTAB, Abdomen: soft, BS+, mild suprapubic tenderness, no rebound, masses, guarding. CVA: mild right CVAT • UA: + WBC, + nitrites, +bacteria, +glucose • BS: 180 • Assessment: UTI, DM, Hyperglycemia • Plan: Bactrim, Urine C+S, increase fluids

Practice 5 • Abdominal pain • 58 year old female c/o abdominal pain and dysuria for 4 days. It has gotten worse today and she feels she has to urinate every 30 min. Also had fever and nausea. She denies flank pain and vaginal d/c. Has tried cranberry juice • PMH: NIDDM • Meds: Metformin; PCN allergy • Social hx: sexually active with husband • VS: 130/80, 12, T 100 F • NAD, CV: RRR no murmurs, no edema, Pulm: CTAB, Abdomen: soft, BS+, mild suprapubic tenderness, no rebound, masses, guarding. mild right CVAT, GYN: Cervix normal, adnexa nontender, external vagina normal, Psy: normal judgement, orientedx 3, appropriate mood. • UA: + WBC, + nitrites, +bacteria, +glucose • BS: 180 • Assessment: UTI, DM, Hyperglycemia • Plan: Bactrim, Urine C+S, increase fluids

Diagnosis Codes ICD-10 • A 00 -B 99=Certain infectious and parasitic diseases • C 00 -D 44=Neoplasms • D 50 -D 89= Diseases of the blood • E 00 -E 90= Endrocrine, nutritional

Diagnosis Codes ICD-10 • http: //www. icd 10 data. com/ • https: //itunes. apple. com/us/app/icd 10 consult-2016 -free/id 358845668? mt=8 • http: //www. imedicalapps. com/2015/10/b est-free-icd-10 -apps/2/#

Diagnosis Codes ICD-10 • Problem codes • V, Y, Z, U

CPT codes • BILL AWAY- Not just 99213, 99214, etc • 69210= cerumen removal • 10060= Incision and Drainage
- Slides: 28