Biliary intervention sedation and analgesia Is it good

Biliary intervention; sedation and analgesia. Is it good enough? Dr CKL Cook Interventional Radiologist Weston General Hospital and Bristol Royal Infirmary No conflicts of interest

Overview • Background of patients and pathology, and imaging • The procedure • The risks • Survey of IR across SW UK • Conclusions

Overview • Background of patients and pathology, and imaging • The procedure • The risks • Survey of IR across SW UK • Conclusions

Biliary intervention; patients/ pathology • Biliary obstruction; carcinoma pancreas, cholangiocarcinoma, Lymph nodes/ adjacent tumours, hepatic metastases, benign causes. • Elderly, chronic ill-health, near end of life
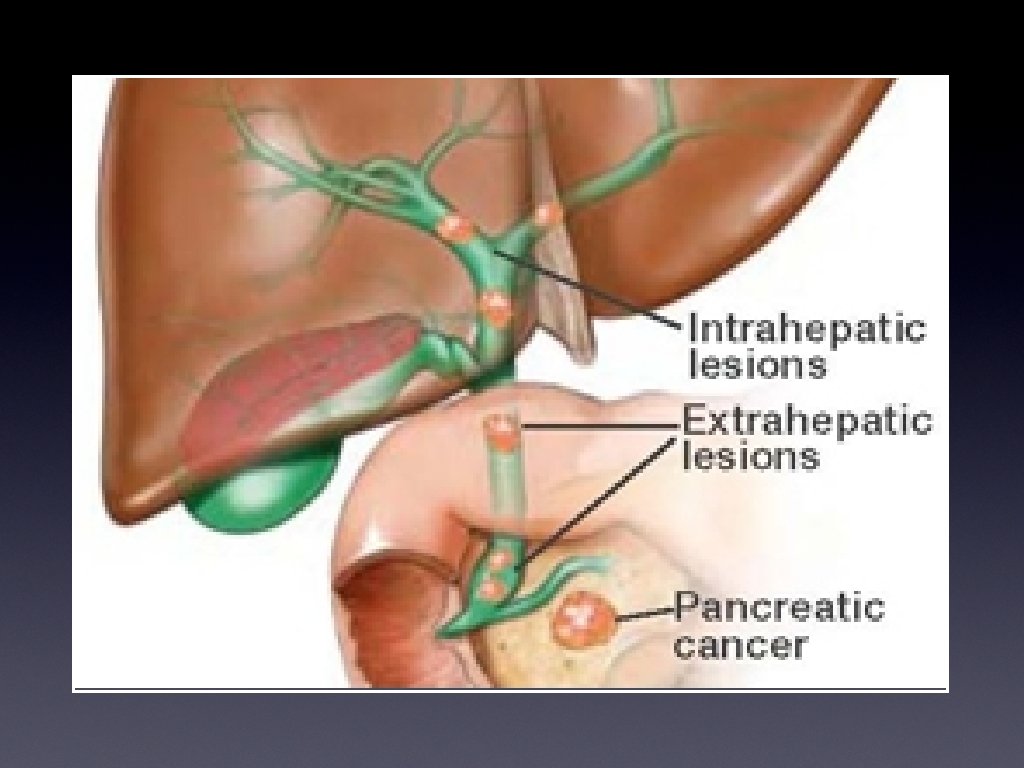

Presentation • Painless jaundice • Obstructive; pale stool, dark urine • Weight loss • Abdominal or back pain • Other indicators of primary or secondary disease

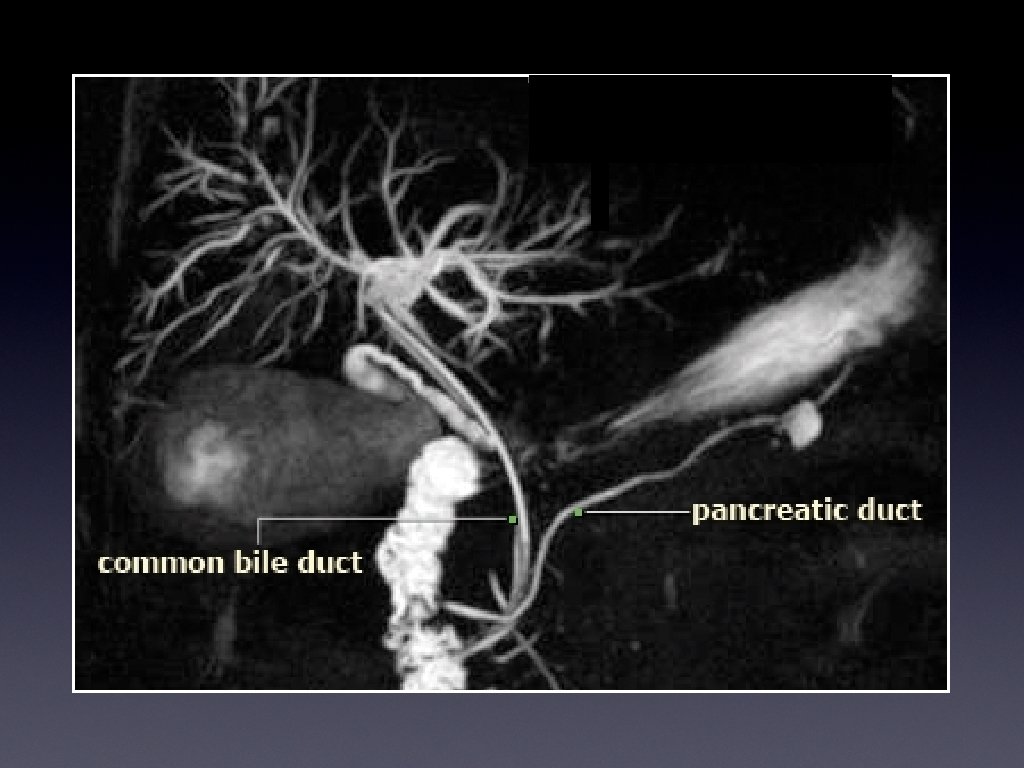
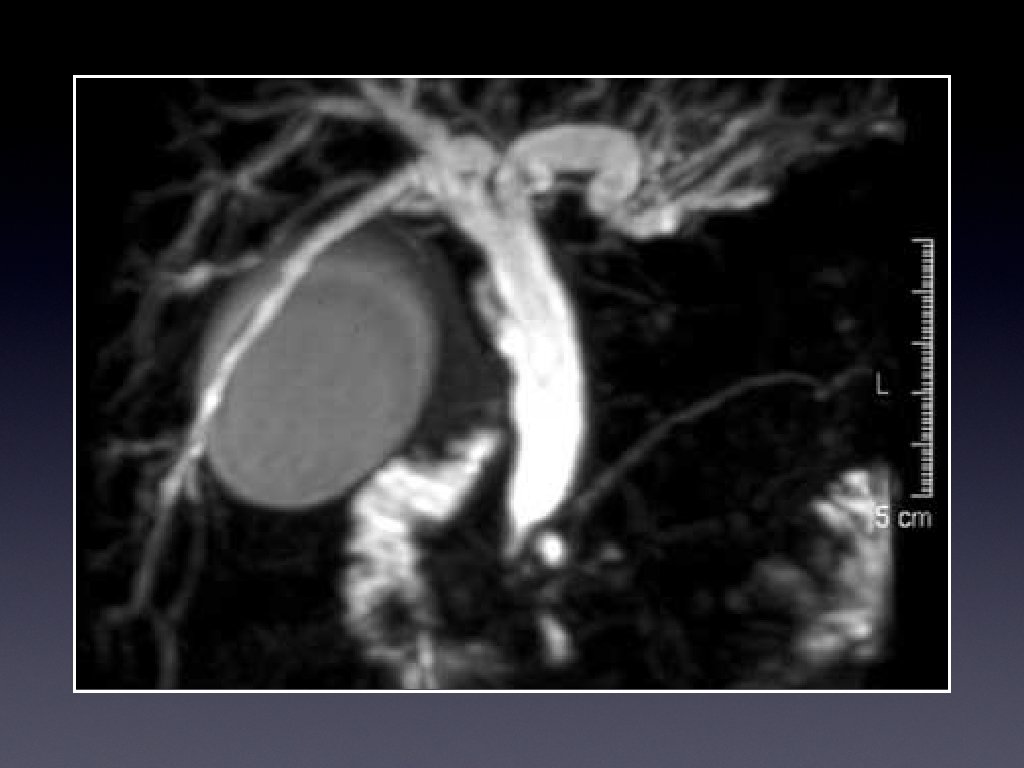
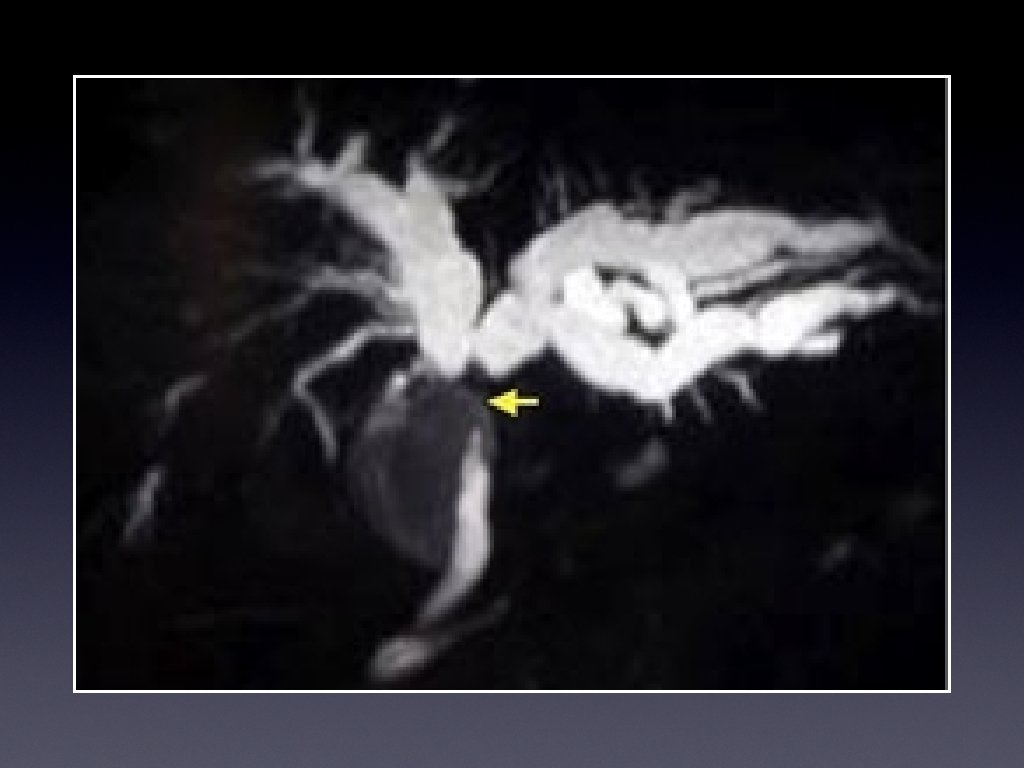
Investigations • Ultrasound • CT for evaluation, and full staging • Magnetic resonance cholangiography (MRCP)


Investigations • Ultrasound • CT for evaluation, and full staging • Magnetic resonance cholangiography (MRCP)
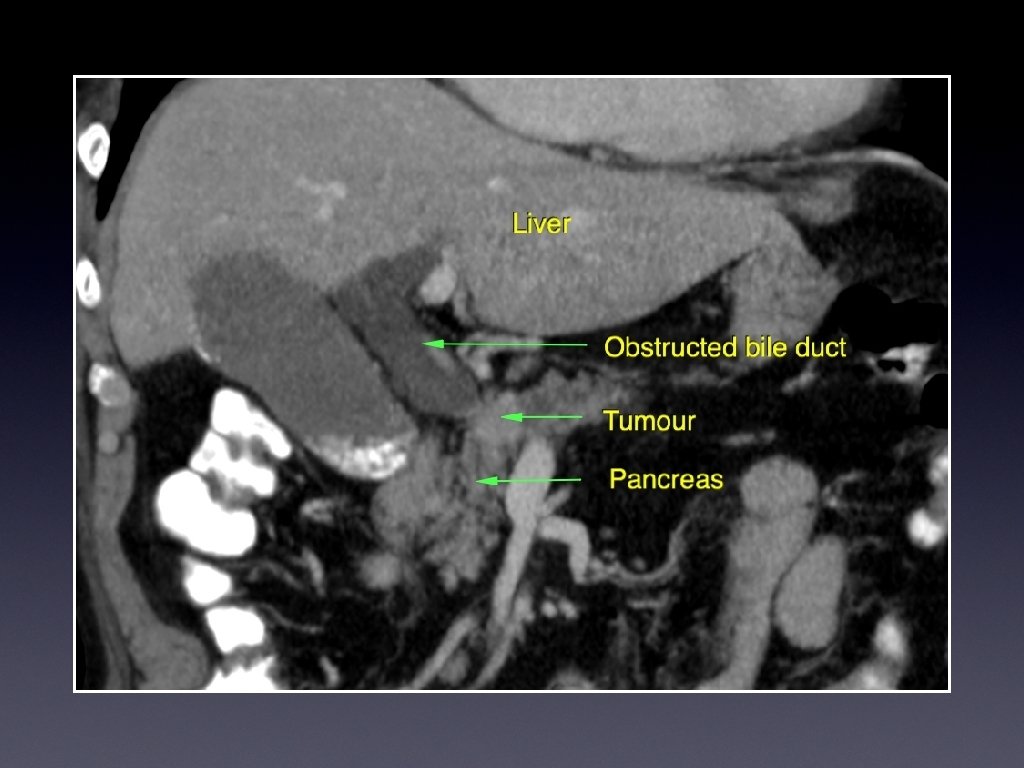

Investigations • Ultrasound • CT for evaluation, and full staging • Magnetic resonance cholangiography (MRCP)

Overview • Background of patients and pathology, and imaging • The procedure • The risks • Survey of IR across SW UK • Conclusions

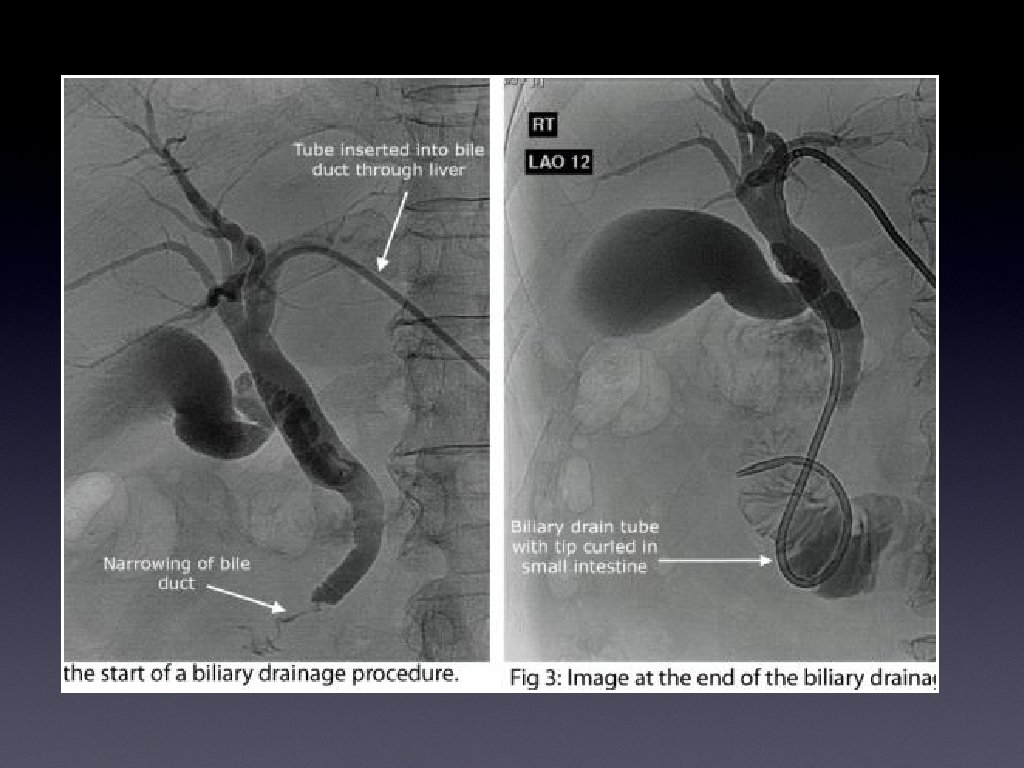
Intervention for biliary obstruction • MDT; Surgical, palliative, or best supportive care • Planning for intervention • ERCP- Endoscopic retrograde cholangiopancreatography and stent. 1 st line • PTC- percutaneous transhepatic cholangiography/ drainage/ stent. 2 nd line, unless known duodenal compression or proximal lesions.


Percutaneous biliary intervention • Percutaneous drain or stent • U/S and flouroscopic guidance; in Radiology Dept • Hydration, antibiotics, clotting, preliminary U/S to confirm extent of duct dilation • WHO/ RCR pre IR checklist

 • Zilver (Cook Medical)")
Metallic biliary stent • Wall stent (Boston Sci) • Zilver (Cook Medical)

Overview • Background of patients and pathology, and imaging • The procedure • The risks • Survey of IR across SW UK • Conclusions

High Risk • Percutaneous biliary interventions are high risk procedures, with data suggesting immediate mortality of between 0. 6 and 5. 6% (1 -4) • The UK Percutaneous Biliary Drainage Audit (2012) showed mortality at 30 days in the region of 19%*. • *British Society of Interventional Radiology: Biliary Drainage and Stenting Registry (BDSR) Cardiovasc Intervent Radiol (2012) 35: 127 -138

High risk stratification* Immediate • Albumen less than 30 • Ascities • WCC greater than 14, CRP greater than 50 • Hb less than 11 Early Urea greater than 12 Bilirubin greater than 300, and ALT greater than 150. *Eur Radiol (2011) 21: 1948 -1955

Summary • Patients, pathology, imaging • MDT planning • Types of intervention • High Risk

Overview • Background of patients and pathology, and imaging • The procedure • The risks • Survey of IR across SW UK • Conclusions

Regional Survey • Regional survey of Interventional Radiologists across the South West of the United Kingdom • Approx 60 interventional Radiologists, and 40 IR nurses • Southampton – Oxford – Bristol – Plymouth – Cardiff • CIRSE; Cardiovascular and Interventional Radiology Society Europe, Lisbon 2015

% patients Patient pain

2. The % of patients that appear to experience MORE than moderate pain, or move during procedure

Overall level of analgesia and sedation % Respondents
 and interventionalists")
Comments/ Conclusions • Although a small number of both IR nurses (28%) and interventionalists (16%) feel that an anaesthetist is unnecessary for these procedures, 57% IR nurses, and 64% of interventionalists felt that patients experience moderate to severe pain, and 72% of nurses felt that an anaesthetist would improve the patient experience. • 37% of interventionalists stated they never had an anaesthetist but would like one, and more than 50% said they did not due to a difficulty to organise at short notice (and small case load). • 50 % of IR teams have never had formal training in sedation. • Only 5% of teams routinely have anaesthetic support.

Qualitative responses • IR nurses… • Procedure often poorly tolerated • PTC patients deserve and require better pain relief • We are aware of occasions when a patient will be in a lot of pain • Radiologists… • Difficult to predict • Highly variable • Sedation and analgesia is somewhere between poor and satisfactory • I strongly believe anaesthetic cover should be the norm • Not normally a problem • Pain can be severe, and difficult to control

Anaesthetic role • Pre-intervention clinical review • Maximise pre-operative state; renal, hydration, cardiac, infective • Sedation and analgesia • Patient relaxed, reassured, pain free, and still • Post operative care

Overview • Background of patients and pathology, and imaging • The procedure • The risks • Survey of IR across SW UK • Conclusions
 Second opinion for IR")
Conclusions Benefits; (based on medical rationale and quality of care) Second opinion for IR team Maximise pre-operative state Analgesia – per and post operative Properly trained in sedating, and monitoring analgesic levels Problems; (issues of management and logistical limitations) Short notice Small and un-predictable caseload number

Biliary intervention; sedation and analgesia. Is it good enough? Dr CKL Cook Interventional Radiologist

Biliary intervention; sedation and analgesia. Is it good enough? No, not without an anaesthetist Dr CKL Cook Interventional Radiologist
 Percutaneous biliary")
References • 1. Mueller PR, van stonnenberg E, Ferrucci JT Jr (1982) Percutaneous biliary drainage: technical and catheter-related problems in 200 procedures. AJR Am J Roentgenol 138: 17 -23 • 2. Yee ACM Ho CS (1987) Complications of percutaneous biliary drainage: benign vs malignant diseases. AJR Am J Roentgenol 148: 1207 -1209 • 3. Clark RA, Mitchell SE, Colley DP, Alexander E (1981) Percutaneous catheter biliary decompression. AJR Am J Roentgenol 137: 503 -509 • 4. Carrasco CH, Zornoza J, Bechtel WJ (1984) Malignant biliary obstruction: complications of percutaneous biliary drainage. Radiology 152: 343 -346 • 5. Uberoi R, Das N, Moss J, Robertson I. British Society of Interventional Radiology: Biliary Drainage and Stenting Registry (BDSR) Cardiovasc Intervent Radiol (2012) 35: 127 -138 • 6. Tapping CR, Byass OR, Cast JEI Percutaneous transhepatic biliary drainage (PTBD) with or without stent complications, re-stent rate and a new risk stratification score. Eur Radiol (2011) 21: 1948 -1955
- Slides: 38