Biliary Ducts Anatomy Dr Mohamed Kandeel Prof of

Biliary Ducts Anatomy Dr. Mohamed Kandeel Prof. of General Surgery. Faculty of Medicine Ain Shams University

Physiology of biliary system • The biliary ducts convey bile from the liver to the duodenum. • Bile is produced continuously by the liver and stored and concentrated in the gallbladder, which releases it intermittently when fat enters the duodenum. • Bile emulsifies the fat, so that it can be absorbed in the distal intestine.

Anatomy of biliary system • The hepatocytes secrete bile into the bile canaliculi formed between them. • The canaliculi drain into the small interlobular biliary ducts.

• The interlobular biliary ducts then drain into large collecting bile ducts of the intrahepatic portal triad, which merges to form the right and left hepatic ducts.

• Shortly after leaving the porta hepatis, the right and left hepatic ducts unite to form the common hepatic duct, which is joined by the cystic duct to form the bile duct, which conveys the bile to the duodenum.

• The right hepatic duct is short and intrahepatic, • The left hepatic duct has a long superficial transverse extrahepatic course beneath segment IV making it accessible through an extending transverse incision for sizable hepaticoenterostomy when more distal anastomoses are not feasible

1 ry branches of portal triad to each liver 2 ry branches to each division 3 ry segmental branches

Variations of intra-heptic biliary system • Variations of intraheptic biliary system exist which represents special challenge in hepatic resection surgery particularly in hepatic living donor transplantation patients.

Common bile duct - CBD • The common bile duct forms in the free edge of the lesser omentum by the union of the cystic duct and the common hepatic duct. • The length of the bile duct varies from 5 to 15 cm, depending on where the cystic duct joins the common hepatic duct. • The bile duct descends posterior to the first part of the duodenum and lies in a groove on the posterior surface of the head of the pancreas.
 side of the second part of the duodenum,")
• On the left (medial) side of the second part of the duodenum, the bile duct comes into contact with the main pancreatic duct. • These ducts run obliquely through the wall of this part of the duodenum, where they unite to form the hepatopancreatic ampulla (ampulla of Vater). • The distal end of the ampulla opens into the duodenum through the major duodenal papilla.

Variation of union of Bile and pancreatic ducts

Sphincter of Oddi • The circular muscle around the distal end of the bile duct is thickened to form the sphincter of the bile duct. • Sphincter of Oddi which is a combination of sphincter papillae, bile duct sphincter, and pancreatic sphincter plays an important role in preventing reflux cholangitis

• Having a common channel in a good pecentage of population, a pancreatic neoplasm cause biliary obstruction while a stone impacted in the ampulla may cause acute pancreatitis.

Acute pancreatitis INDEX

Arterial supply of the bile duct • Cystic artery: supplying the proximal part of the duct. • Right hepatic artery: supplying the middle part of the duct. • Posterior superior pancreaticoduodenal artery and gastroduodenal artery: supplying the retroduodenal part of the duct.

• The network of vessels from above and below form a delicate epicholedochal plexus on the surface of the duct. This plexus is easily injured by dissection and cautery and this may result in later stricture.

Venous drainage • The veins from the proximal part of the bile duct and the hepatic ducts usually enter the liver directly. • The posterior superior pancreaticoduodenal vein drains the distal part of the bile duct and empties into the portal vein or one of its tributaries.

Lymphatics • The lymphatic vessels from the gallbladder and bile duct pass to the cystic lymph nodes near the neck of the gallbladder, the node of the omental foramen, and the hepatic lymph nodes. • Efferent lymphatic vessels from the bile duct pass to the celiac lymph nodes. • The lymphatic vessels of the gallbladder and biliary passages anastomose superiorly with those of the liver and inferiorly with those of the pancreas.

Nerve supply • The sympathetic nerve supply is vasomotor in the liver and biliary system. • Although parasympathetic innervation can open the sphincter of the bile duct (and the weaker sphincter of the hepatopancreatic ampulla) and contract the gallbladder, typically these are hormonally regulated responses to fat entering the duodenum
 lies in the fossa for the")
Gallbladder • The gallbladder (7 -10 cm long) lies in the fossa for the gallbladder on the visceral surface of the liver. • In its natural position the body of the gallbladder lies anterior to the duodenum, and its neck and the cystic duct are immediately superior to the duodenum.

Gallbladder, cont • The pear-shaped gallbladder can hold up to 50 ml of bile. • Peritoneum completely surrounds the fundus of the gallbladder and binds its body and neck to the liver. • The hepatic surface of the gallbladder attaches to the liver by connective tissue of the fibrous capsule of the liver.

• The gallbladder has three parts – Fundus: the wide end of the organ, projects from the inferior border of the liver and is usually located at the tip of the right 9 th costal cartilage in the MCL. – Body: contacts the visceral surface of the liver, the transverse colon, and the first part of the duodenum. – Neck: narrow and tapered; directed toward the porta hepatis; it makes an S-shaped bend and joins the cystic duct.

Infundibulum of the Gallbladder • In diseased states of the gallbladder, a dilation or pouch appears at the junction of the neck of the gallbladder and the cystic duct. • This pouch is called the infundibulum of the gallbladder (Hartmann pouch). • Gallstones commonly collect in the infundibulum.

Mobile Gallbladder • The gallbladder has a short mesentery in approximately 4% of people. • Such gallbladders are subject to vascular torsion and infarction

• The distal end of the ampulla of Vater is the narrowest part of the biliary passages and is the common site for impaction of gallstones. • The infundibulum of the gallbladder is another common site for impaction. • Gallstones may also lodge in the hepatic and cystic ducts.

• In the event that a gallstone causes biliary obstruction, the gallbladder is shrunken owing to fibrosis and is unlikely to be distensible. • With other causes of obstruction, the gallbladder distends as a result of the back-pressure from obstructed bile flow. • Courvoisier's law states that in the presence of a palpable gall bladder, jaundice is unlikely to be caused by gall stones

Patients with obstructive jaundice & GB mass – think of malignant obstruction Liver Gall bladder (markedly dilated) Cancer head Kidney IVC Aorta INDEX
 the tissue boundaries between the")
Gallstone ileus • Continued inflammation may break down (ulcerate) the tissue boundaries between the gallbladder and a part of the alimentary tract adherent to it (duodenum, transverse colon), resulting in a cholecystenteric fistula and gallstone ileus.


 connects the neck of")
Cystic duct • The cystic duct (3 -4 cm long) connects the neck of the gallbladder to the common hepatic duct. • The mucosa of the neck spirals into spiral fold (spiral valve).

• This spiral fold helps keep the cystic duct open; thus – bile can easily be diverted into the gallbladder when the distal end of the bile duct is closed by the sphincter of the bile duct and/or hepatopancreatic sphincter, or – bile can pass to the duodenum as the gallbladder contracts.

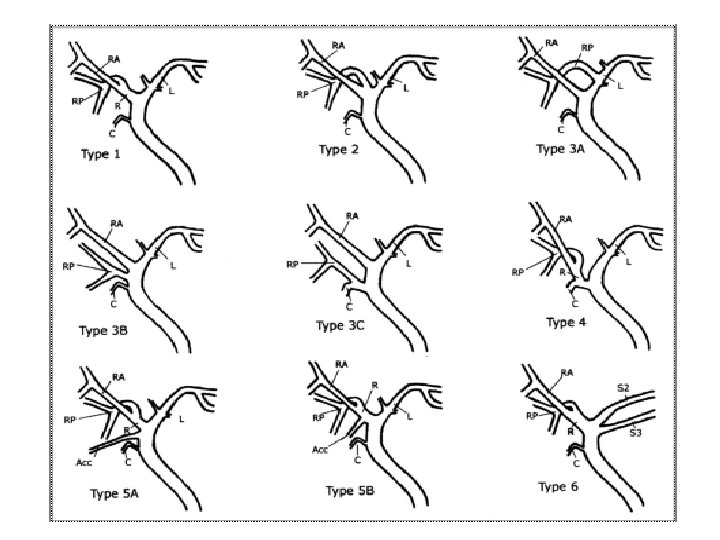
Variations in the Cystic and Hepatic Ducts • Understanding the variations in arteries and bile duct formation is important for surgeons when they ligate the cystic duct during cholecystectomy

Variations in the Cystic and Hepatic Ducts

Accessory Hepatic Ducts • An accessory duct is a normal segmental duct that joins the biliary system outside the liver instead of within it. • Accessory (aberrant) hepatic ducts are common and are in positions of danger during cholecystectomy. • Because it drains a normal segment of the liver, it leaks bile if inadvertently cut during surgery

Accessory Hepatic Ducts

Blood supply • The cystic artery supplies the gallbladder and cystic duct. • It commonly arises from the right hepatic artery in the angle between the common hepatic duct and the cystic duct (cystohepatic triangle, Calot triangle). • Variations occur in the origin and course of the cystic artery and hepatic arteries. • Awareness of such variations is essential to avoid their injuries specially with increased era of laparoscopic surgery.

Aberrant Hepatic Arteries • Right or left hepatic artery that arises commonly as a terminal branch of the hepatic artery proper may be replaced in part or entirely by an aberrant (accessory or replaced) artery arising from another source. • The most common source of an aberrant right hepatic artery is the SMA. The most common source of an aberrant left hepatic artery is the left gastric artery.

Aberrant Hepatic Arteries

Variations in the Relationships of the Hepatic Arteries • In most people, the right hepatic artery crosses anterior to the portal vein • However, in some people, the artery crosses posterior to the portal vein. • In most people, the right hepatic artery runs posterior to the common hepatic duct. • In some individuals the right hepatic artery crosses anterior to the common hepatic duct, or • The right hepatic artery arises from the SMA and so does not cross the common hepatic duct at all.

Variations in the Relationships of the Hepatic Arteries

Variation in origin and course of cystic artery

Venous drainage • The cystic veins, draining the neck of the gallbladder and cystic duct, – enter the liver directly or – drain through the portal vein to the liver, after joining the veins draining the hepatic ducts and upper bile duct. • The veins from the fundus and body of the gallbladder pass directly into the visceral surface of the liver and drain into the hepatic sinusoids.

Lymphatics • The lymphatic drainage of the gallbladder is to the hepatic lymph nodes, often through cystic lymph nodes located near the neck of the gallbladder. • Efferent lymphatic vessels from these nodes pass to the celiac lymph nodes.
- Slides: 46