Bifurcations A Simplified Approach Disclosures None Bifurcations account

Bifurcations: A Simplified Approach

Disclosures None

Bifurcations account for 30% of lesions in pts with MVD 70 -80% of LM interventions involve the bifurcation We are all here at 6: 30 am to attend Over a 1000 published studies on the subject since Colombo conducted the first randomized A bifurcation workshop trial In 2002 -2003 A dedicated European bifurcation club formed in 2004

Side-Branch Loss Ta r ge Peri-Procedural MI STENT THROMBOSIS RESTENOSIS t. V es se l. F ail ur e

BIFURCATIONS What have we learned from the published data ?

NORDIC Trial 5 Year Follow-UP EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY JACC 2013; 62: 30 -34
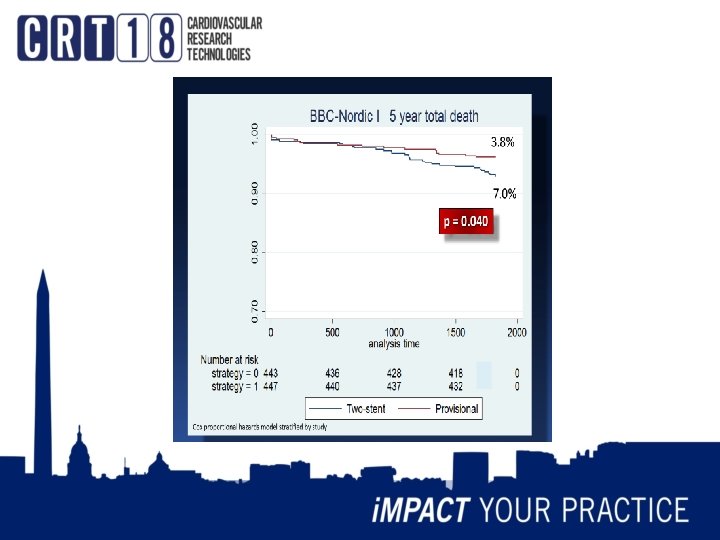

Based on the totality of evidence in published data: A provisional single stent strategy should remain the default primary approach in the vast majority of cases
 Angle B (Bifurcation) Angle A: The more acute")
Diameters & Angles Angle A (Approach) Angle B (Bifurcation) Angle A: The more acute the more difficult side branch access becomes, the more obtuse The easier SB access becomes Angle B: The more acute the higher the likelihood of carina shift and SB occlusion

MEDINA CLASSFICATION SB Size & importance/Ostial involvment/disease extension into SB/liklihood of plaque carina shift (bifurcation angle), difficulty in wiring SB (approach angle) MB (proximal) Size relative to size of SB & MB (distal) (D 1 = 0. 67(D 2 + D 3) . EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY

STENT SIZING & CARINA/PLAQUE SHIFT EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY

EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY © 2016 Europa Digital & Publishing. All rights reserved. PROVISIONAL STENTING WITH FINAL KISSING BALLOON
 in Jailed SB No lesion with <75%")
Correlation Between FFR and percent stenosis (QCA) in Jailed SB No lesion with <75% arestenosis lly hica. FFR<0. 75. phad > 75% a r g o i g n yo a m e R r F a F t y a b h t ns sed o e i s s s e a l f n o e h Among 73 lesions with nt w a c i f i Only 30% n g i s ally c i ≥ 75% stenosis, only 20 m a n y d o m e a h lesions were functionally significant. Koo BK et al J Am Coll Cardiol 2005; 46: 633– 7)

� When BAILOUT STENTING - Decreased TIMI flow - High grade stenosis (especially with chest pain) remember angiographic appearance can overestimate functional severity - Dissection of SB � How - TAP/T Stenting - Culloette � ALWAYS A FINAL KISSING BALLOON DILITATION ONCE YOU CONVERT TO TWO STENT BAILOUT
 True")
When one might consider an upfront complex two stent strategy ? � 1) True Bifurcation Lesion (111, 011, 101) Especially if Long lesion (> 10 mm) in a sizable SB (> 2. 5 mm) � 2) Risk of SB occlusion may be associated with serious HD consequences (very large SB with limited ostial extension, poor myocardial reserve, high jepordy score) � 3) Difficult access to SB (Acute approach angle)

IS THERE A PREFFERED A PRIORI TWO STENT STRATEGY �Simple answer NO �But…. . . �Get familiar with one or two and perfect them rather than trying to learn all

IS THERE A PREFFERED A PRIORI TWO STENT STRATEGY �My prefered strategies are - TAP (easy & suitable for most bailout situations after failed provisional strategy & as a priori 2 stent strategy in cases with a wide bifurcation angle) - DK-CRUSH (accumilating evidence in both LM & non. LM PCI that it may be a superior strategy with the caveat it is more technically demanding)

TWO STENT STRATEGY: DK-CRUSH . EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY

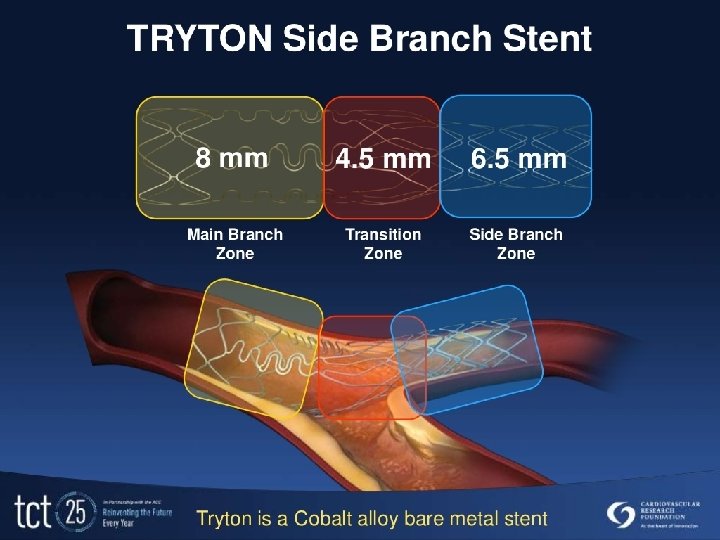
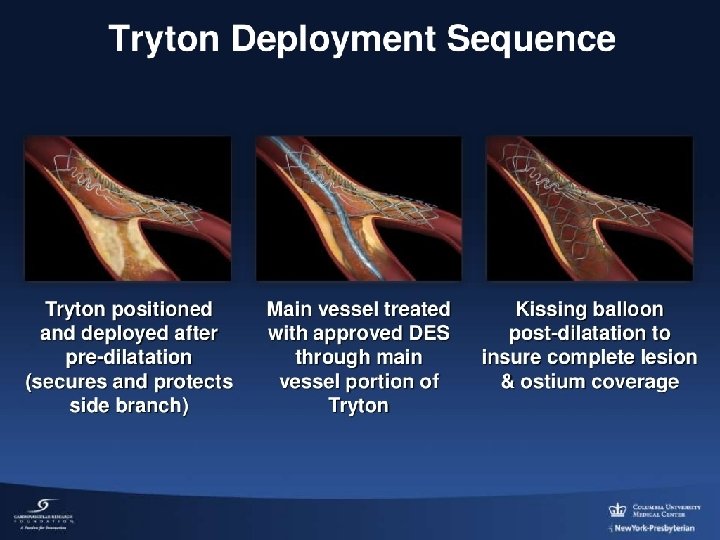
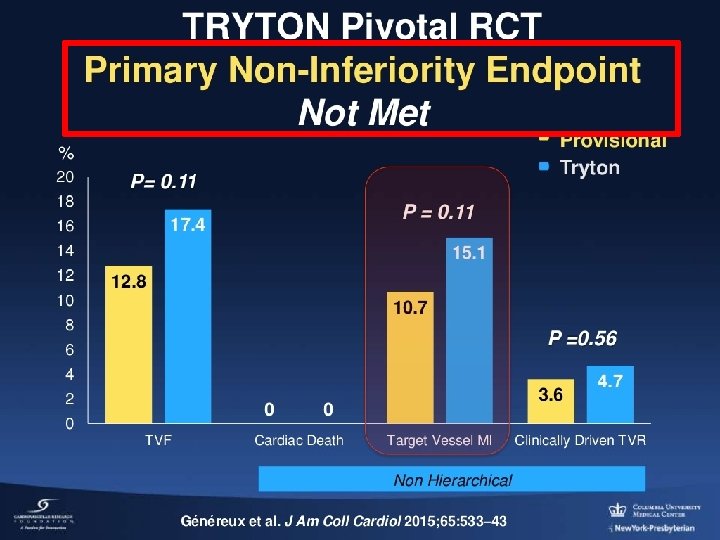
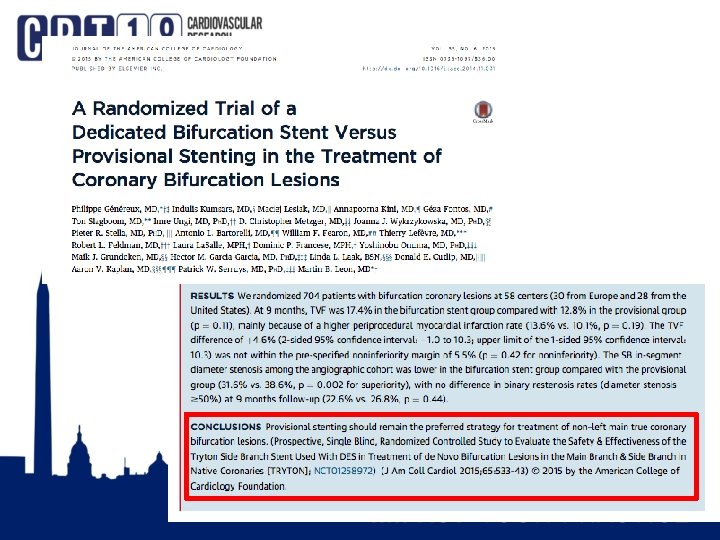
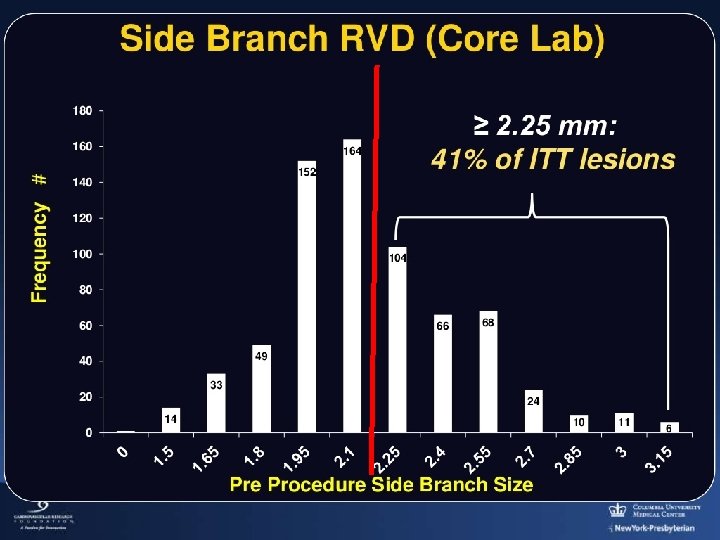
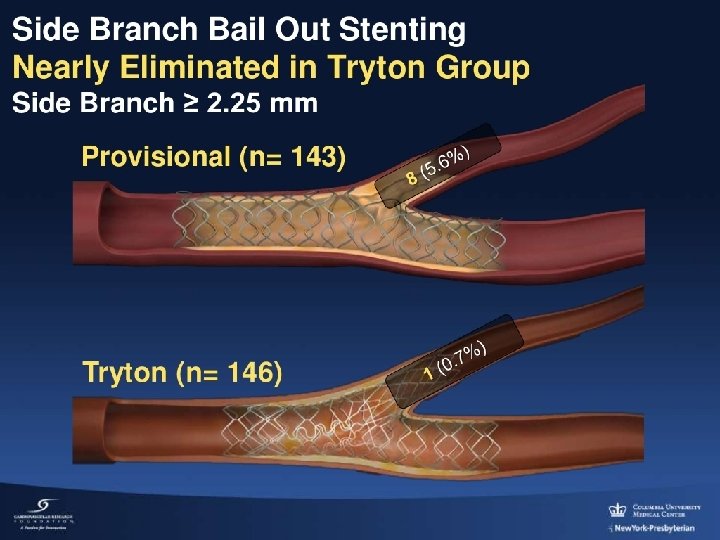
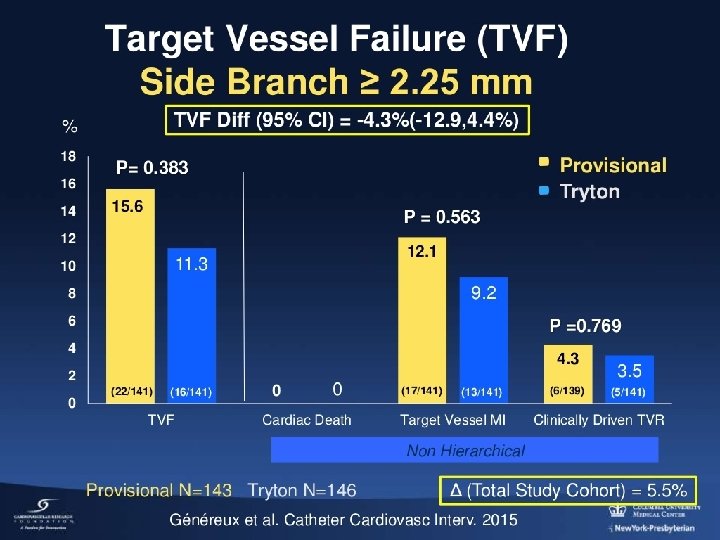
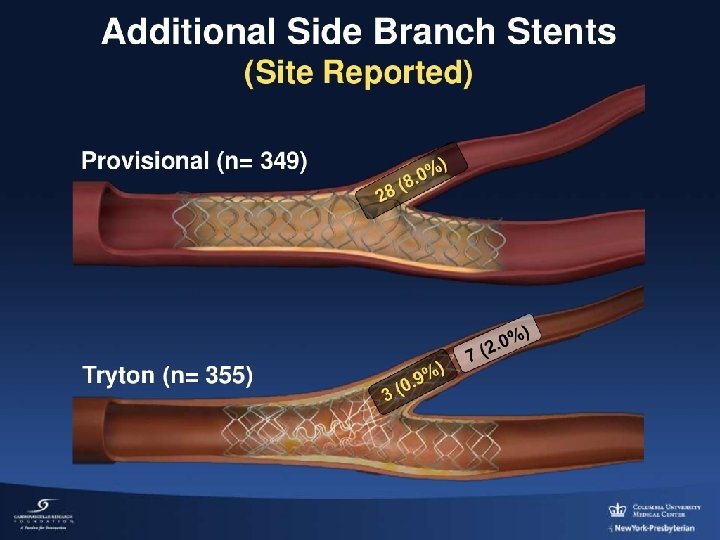
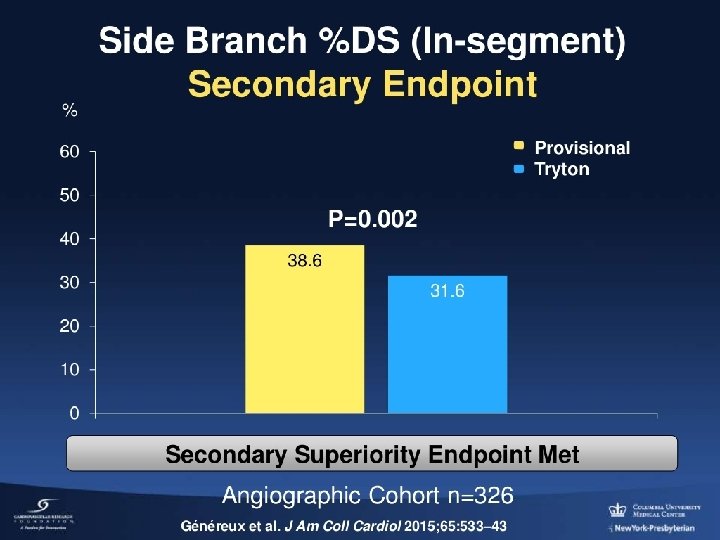
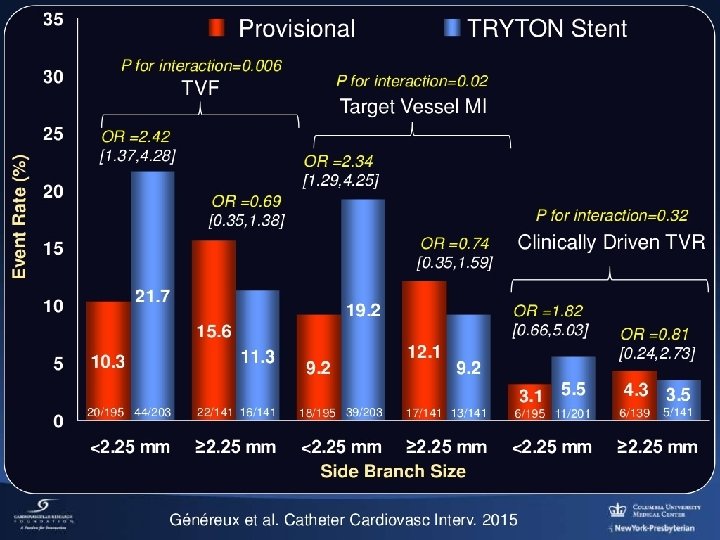
WHAT ABOUT DEDICATED BIFURCATION STENTS

MY BIFURCATION STRATEGY FKB +/NO DISEASE OR DISEASE EXTENDS < 5 mm PROVISIONAL STENT STRATEGY BAILOUT STENT (TAP or T) SIDE BRANCH OSTIUM LONG OSTIAL DISEASE or SB ACCESS DIFFICULT TAP or T TWO STENT STRATEGY DK-CRUSH

MY BIFURCATION RULES �Always size to the distal MV �Always perform a proximal optomization (POT) �With any 2 stent strategy ALWAYS perform FKB �If having difficulty crossing stent struts with wire or balloon NEVER use excessive force consider repeating POT at higher pressure or bigger balloon &/or rewiring after a repeat POT �An undersized compliant balloon has a better crossing profile than a high pressure non-compliant balloon and can facilitate subsequent recrossing with a high pressure balloon


WATCH THIS SPACE

EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY The PCR-EAPCI Textbook – Percutaneous interventional cardiovascular medicine Bifurcation lesions Yves Louvard, Thierry Lefèvre, Marie-Claude Morice © 2016 Europa Digital & Publishing. All rights reserved. Figure 24

EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY The PCR-EAPCI Textbook – Percutaneous interventional cardiovascular medicine Bifurcation lesions Yves Louvard, Thierry Lefèvre, Marie-Claude Morice © 2016 Europa Digital & Publishing. All rights reserved. Figure 7

EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY The PCR-EAPCI Textbook – Percutaneous interventional cardiovascular medicine Bifurcation lesions Yves Louvard, Thierry Lefèvre, Marie-Claude Morice © 2016 Europa Digital & Publishing. All rights reserved. Figure 22

DK-Crush Technique © 2016 Europa Digital & Publishing. All rights reserved. EDUCATIONAL CONTENT ENDORSED BY EAPCI, A REGISTERED BRANCH OF THE EUROPEAN SOCIETY OF CARDIOLOGY
- Slides: 41