Bicuspid Aortic Valve 06012007 Bicuspid aortic valve n

Bicuspid Aortic Valve 06/01/2007

Bicuspid aortic valve n Definition: – Two functional aortic valve leaflets with two complete commissures § AKA “Bicommissural aortic valve”

Bicuspid aortic valve n Felt to represent a complex continuum – Unicommissural, Bicommissural, Tricuspid, and Quadricuspid n Not simply a fusion of two normal cusps
 Unequally sized cusps – Larger")
Bicuspid aortic valve n Three criteria: n 1. ) Unequally sized cusps – Larger leaflet is the "conjoined" leaflet

http: //www. nucleusinc. com
 Presence of a central ridge (raphe) – Usually")
Bicuspid Aortic Valve n 2. ) Presence of a central ridge (raphe) – Usually in the center of the conjoined leaflet
 Smooth cusp margins – Excludes tricuspid valves which")
Bicuspid Aortic Valve n 3. ) Smooth cusp margins – Excludes tricuspid valves which fused due to inflammatory processes (eg, rheumatic fever) § Irregularity and scarring within the raphe.
 leaflet – Left-right")
Morphology n Orientation: – Anterior-posterior § Left leaflet § Right (conjoined) leaflet – Left-right § Anterior (conjoined) leaflet § Posterior leaflet

Physiology n Normally functioning bicuspid valve – Abnormal folding and creasing – Restricted motion – Turbulent flow n Prolonged stress leads to valve damage

Statistics n Estimated overall incidence of 1 -2% n M: F at least 2: 1 n Familial clustering suggests AD with variable penetrance n No race or geographical predilection

Associated Anomalies n Left dominant coronary artery – Up to 50% § 10% with tricuspid valve n Short left main coronary artery – Less than 5 mm

Associated Anomalies n Coarctation of the aorta n Interrupted aortic arch – >50% have bicuspid aortic valve

Associated Anomalies n Turner's Syndrome – Up to 30% n William's Syndrome – Up to 10%

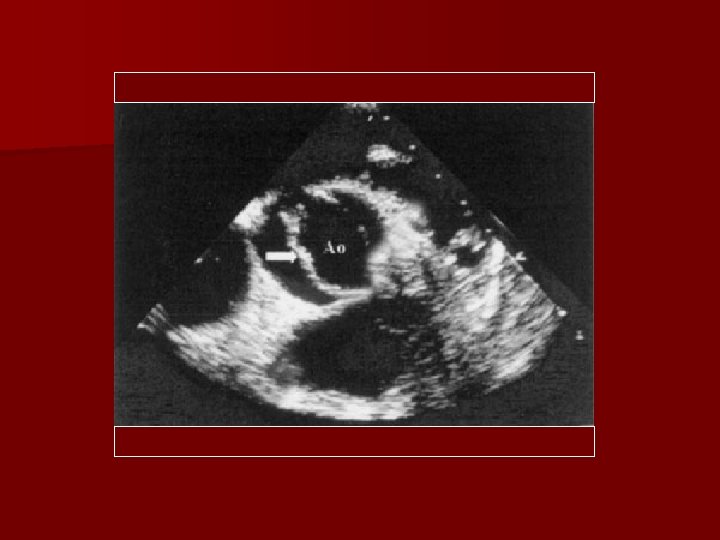
Imaging n Echocardiography – Modality of choice § Long-axis shows systolic doming due to limited valve opening § Short-axis allows examination of the commisures, leaflet morphology, and mobility.

Radiographs n Usually normal in pediatric population n Aortic root enlargement n Left ventricular enlargement n May see calcified raphe or leaflets

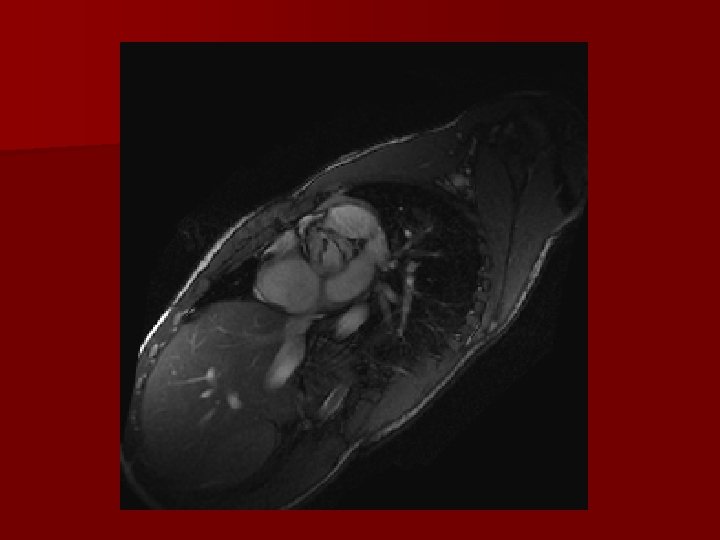
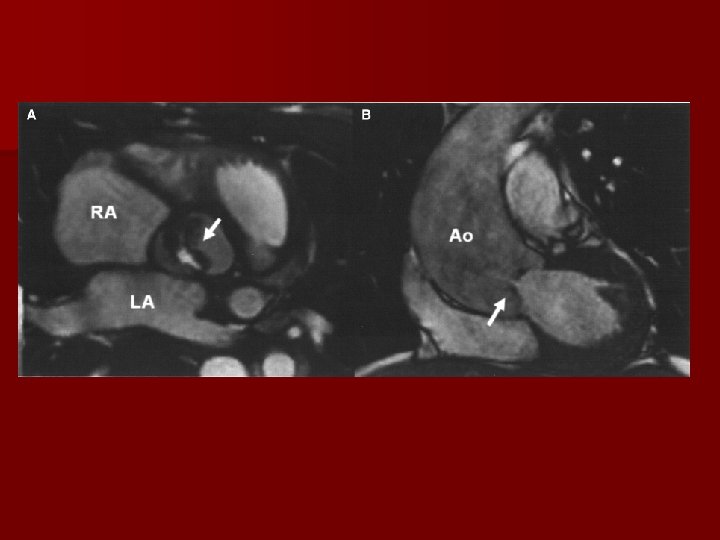
CT/MRI n Allows for evaluation of the aorta and coronary arteries n Functional information

http: //medirec. ncvc. go. jp/

Pathology n Aortic Stenosis n Aortic Insufficiency n Bacterial Endocarditis n Aortic Dissection

Aortic Stenosis n Poorly functioning valves may have incomplete systolic opening n Responsible for 80 -95 % of aortic valve disease detected in infancy – May cause rapid deterioration – Progression over years is more common

Aortic Stenosis n Bicuspid valve may be prone to accelerated aging – Sclerosis begins in the second decade of life – Estimated that 50% of adults with severe AS have bicuspid valves.

Aortic Stenosis n Cusps oriented in the AP direction demonstrate more rapid progression n Presence of risk factors can also expedite the process – High LDL, high lipoprotein (A) and smoking

Aortic Insufficiency n Isolated AI n AI with aortic root dilatation

Aortic Insufficiency n Isolated AI – Prolapse of redundant larger cusp § Rarely severe

Aortic Insufficiency n Disruption of the elastic tissue within the upper aortic ring/sinotubular junction – May occur due to inherent abnormality – May be due to coarctation of the aorta or bacterial endocarditis § Often severe with high mortality

Bacterial Endocarditis n Estimated 10 -30% of patients with bicuspid aortic valve – 25% of cases of endocarditis occur on bicuspid valves – Tetralogy of Fallot, VSD, and MVP are the other lesions associated with SBE n Prophylactic antibiotics for dental/surgical procedures

Bacterial Endocarditis n Responsible for half of cases of severe AI in patients with bicuspid valve – Many due to cusp perforation n Unexplained systemic emboli should raise suspicion

Aortic Dissection n Approximately 5% of patients – Etiology is unclear § Abnormal response to hemodynamic stress – Cystic medial necrosis similar to Marfan’s – Dysfunctional microfibrillar proteins, endothelial nitric oxide synthetase, etc.

Medical Management n Lifestyle – Exercise, heart healthy diet, no smoking n Cholesterol and hypertensive medication

Medical Management n Surveillance echocardiography n Early surgical referral n First-degree relative screening

Surgical Treatment n Severe valvular dysfunction or aortic root dilatation n Symptomatic patients n Evidence of abnormal LV dimensions and function

Surgical Treatment n Pediatric cases – Balloon Valvuloplasty § Without calcified valves n Isolated Aortic Insufficiency – Valve Repair n Valve replacement – With or without aortic root replacement § Prosthetic/Bioprosthetic/Homograft § Ross procedure

References n n n Fedak PWM, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation. 2002; 106: 900 – 904 Ward, C. Clinical significance of the bicuspid aortic valve. Heart 2000 83: 81 -85 Pediatric Cardiac Surgery, Mavroudis et al. , 3 rd edition, Mosby, St. Louis. Aboulhosn, J, Child, JS. Left ventricular outflow obstruction: subaortic stenosis, bicuspid aortic valve, supravalvar aortic stenosis, and coarctation of the aorta. Circulation. 2006 Nov 28; 114(22): 2412 -22. http: //www. emedicine. com/ped/topic 2486. htm
- Slides: 35